Immunosuppressant.
ATC code: L04A A10.
Pharmacology: Pharmacodynamics: Mechanism of Action: Sirolimus inhibits T-lymphocyte activation and proliferation that occurs in response to antigenic and cytokine (Interleukin [IL]-2, IL-4, and IL-15) stimulation by a mechanism that is distinct from that of other immunosuppressants. Sirolimus also inhibits antibody production. In cells, sirolimus binds to the immunophilin, FK Binding Protein-12 (FKBP-12), to generate an immunosuppressive complex. The sirolimus: FKBP-12 complex has no effect on calcineurin activity. This complex binds to and inhibits the activation of the mammalian Target Of Rapamycin (mTOR), a key regulatory kinase. This inhibition suppresses cytokine-driven T-cell proliferation, inhibiting the progression from the G
1 to the S phase of the cell cycle.
Studies in experimental models show that sirolimus prolongs allograft (kidney, heart, skin, islet, small bowel, pancreatico-duodenal, or bone marrow) survival in mice, rats, pigs, dogs, and/or primates. Sirolimus reverses acute rejection of heart and kidney allografts in rats and prolongs the graft survival in presensitized rats. In some studies, the immunosuppressive effect of sirolimus lasts up to 6 months after discontinuation of therapy. This tolerization effect is alloantigen specific.
In rodent models of autoimmune disease, sirolimus suppresses immune-mediated events associated with systemic lupus erythematosus, collagen-induced arthritis, autoimmune type I diabetes, autoimmune myocarditis, experimental allergic encephalomyelitis, graft-versus-host disease, and autoimmune uveoretinitis.
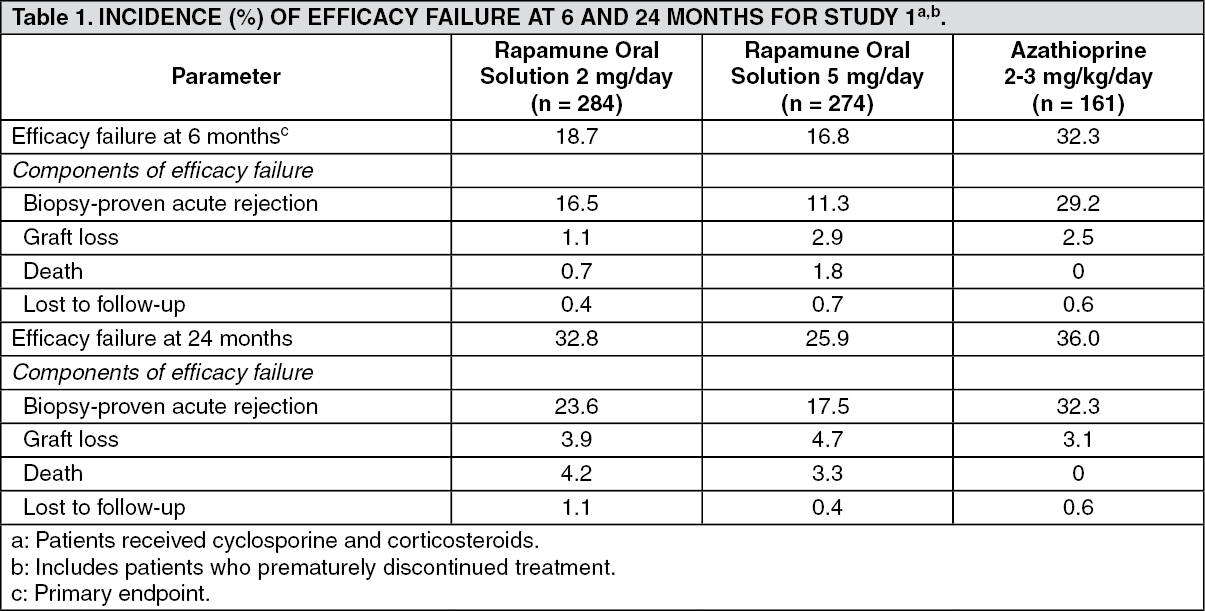
Clinical trials data on efficacy: Prophylaxis of Organ Rejection: The safety and efficacy of Rapamune for the prevention of organ rejection following renal transplantation were assessed in two randomized, double-blind, multicenter, controlled trials. These studies compared two dose levels of Rapamune (2 mg and 5 mg, once daily) with azathioprine or placebo when administered in combination with cyclosporine and corticosteroids. The study of Rapamune (2 mg and 5 mg, once daily) compared to azathioprine was conducted in the United States at 38 sites. Seven hundred nineteen (719) patients were enrolled in this trial and randomized following transplantation; 284 were randomized to receive Rapamune 2 mg/day, 274 were randomized to receive Rapamune 5 mg/day, and 161 to receive azathioprine 2-3 mg/kg/day. The study of Rapamune (2 mg and 5 mg, once daily) compared to placebo control was conducted in Australia, Canada, Europe, and the United States, at a total of 34 sites. Five hundred seventy-six (576) patients were enrolled in this trial and randomized before transplantation; 227 were randomized to receive Rapamune 2 mg/day, 219 were randomized to receive Rapamune 5 mg/day, and 130 to receive placebo. Efficacy failure was defined as the first occurrence of an acute rejection episode (confirmed by biopsy), graft loss, or death.
The primary efficacy analyses from these trials determined that Rapamune, at doses of 2 mg/day and 5 mg/day, significantly reduced the incidence of efficacy failure at 6 months following transplantation compared to both azathioprine and placebo. The reduction in the incidence of first biopsy-confirmed acute rejection (BCAR) episodes in Rapamune-treated patients compared to the control groups included a reduction in all grades of rejection.
The graft and patient survival rates, which were co-primary endpoints, were similar in the Rapamune-treated and comparator-treated patients at 1 year.
The tables as follows summarize the results of the primary efficacy analyses from these trials. Rapamune Oral Solution, at doses of 2 mg/day and 5 mg/day, significantly reduced the incidence of efficacy failure (statistically significant at the <0.025 level; nominal significance level adjusted for multiple [2] dose comparisons) at 6 months following transplantation compared with both azathioprine and placebo. (See Tables 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patient and graft survival at 1 year were co-primary endpoints. The following table shows graft and patient survival at 1 and 2 years in Study 1, and 1 and 3 years in Study 2. The graft and patient survival rates were similar in patients treated with Rapamune and comparator-treated patients. (See Table 3.)
Click on icon to see table/diagram/image
The reduction in the incidence of first biopsy-confirmed acute rejection episodes in patients treated with Rapamune compared with the control groups included a reduction in all grades of rejection.
In the study of Rapamune (2 mg and 5 mg, once daily) with azathioprine comparator, which was prospectively stratified by race within center, efficacy failure was similar for Rapamune 2 mg/day and lower for Rapamune 5 mg/day compared to azathioprine in Black patients. In the placebo-controlled study of Rapamune (2 mg and 5 mg, once daily), which was not prospectively stratified by race, efficacy failure was similar for both Rapamune doses compared to placebo in Black patients. (See Table 4.)
Click on icon to see table/diagram/image
Mean glomerular filtration rates (GFR) at one year post-transplant were calculated using the Nankivell equation for all subjects in each study who had serum creatinine measured at 12 months. In both studies, mean GFR at one year was lower in patients treated with cyclosporine and Rapamune compared to those treated with cyclosporine and the respective azathioprine or placebo control. Within each treatment group in both of these studies, mean GFR at one year post-transplant was lower in patients who experienced at least one episode of biopsy-proven acute rejection, compared to those who did not.
The safety and efficacy of Rapamune as a maintenance regimen were assessed following cyclosporine withdrawal at 3 to 4 months post renal transplantation. In a randomized, multicenter, controlled trial conducted at 57 centers in Australia, Canada, and Europe, five hundred twenty-five (525) patients were enrolled. All patients in this study received the tablet formulation. This study compared patients who were administered Rapamune, cyclosporine, and corticosteroids continuously, with patients who received the same standardized therapy for the first 3 months after transplantation (pre-randomization period) followed by the withdrawal of cyclosporine. During cyclosporine withdrawal, the Rapamune dosages were adjusted to achieve targeted sirolimus whole blood trough concentration ranges (16 to 24 ng/mL until month 12, then 12 to 20 ng/mL thereafter through month 60). At 3 months, 430 patients were equally randomized to either Rapamune with cyclosporine therapy, or Rapamune as a maintenance regimen following cyclosporine withdrawal. Eligibility for randomization included no Banff Grade 3 acute rejection episode or vascular rejection in the 4 weeks before random assignment; serum creatinine ≤4.5 mg/dL; and adequate renal function to support cyclosporine withdrawal (in the opinion of the investigator). The primary efficacy endpoint was graft survival at 12 months after transplantation. Secondary efficacy endpoints were the rate of biopsy-confirmed acute rejection, patient survival, incidence of efficacy failure (defined as the first occurrence of either biopsy-proven acute rejection, graft loss, or death), and treatment failure (defined as the first occurrence of either discontinuation, acute rejection, graft loss, or death).
Based upon the analysis of data from 36 months and beyond, which showed a growing difference in graft survival and renal function, as well as significantly lower blood pressure in the cyclosporine withdrawal group, it was decided by the sponsor to discontinue subjects from the Rapamune with cyclosporine group. When the protocol was amended all subjects had reached 48 months and some completed the 60 months of the study.
The following table summarizes the resulting graft and patient survival at 12, 24, 36, 48 and 60 months for this trial. At 48 months, there was a statistically significant difference in graft survival between the two groups for both analyses (including and excluding loss to follow-up). (See Table 5.)
Click on icon to see table/diagram/image
The following table summarizes the results of first biopsy-proven acute rejection at 12 and 60 months. There was a significant difference in first biopsy-proven rejection between the two groups during post-randomization through 12 months. However at month 60, the difference between the two groups was not significant (6.5% versus 10.2%, respectively). Most of the post-randomization acute rejections occurred in the first 3 months following randomization. (See Table 6.)
Click on icon to see table/diagram/image
The following table summarizes the mean calculated GFR after cyclosporine withdrawal. (See Table 7.)
Click on icon to see table/diagram/image
The mean GFR at 12, 24, 36, 48 and 60 months, calculated by the Nankivell equation, was significantly higher for patients receiving Rapamune as a maintenance regimen following cyclosporine withdrawal than for those in the Rapamune with cyclosporine therapy group. At month 60, patients with an acute rejection at any time after transplantation had a significantly higher mean calculated GFR for patients receiving Rapamune as a maintenance regimen following cyclosporine withdrawal than for those in the Rapamune with cyclosporine therapy group.
The safety and efficacy of conversion from calcineurin inhibitors (CNI) to Rapamune were assessed in maintenance renal transplant patients. This study was a randomized, multicenter, controlled trial conducted at 111 centers globally, including US and Europe. Eight hundred thirty (830) patients were enrolled and stratified by baseline calculated glomerular filtration rate (GFR, 20-40 mL/min versus greater than 40 mL/min). Enrollment in the patient stratum with baseline calculated GFR less than 40 mL/min was discontinued due to an imbalance in safety events (see Precautions and Adverse Reactions).
This study compared renal transplant patients (6-120 months after transplantation) who were converted from calcineurin inhibitors to Rapamune, with patients who continued to receive calcineurin inhibitors. Concomitant immunosuppressive medications included mycophenolate mofetil (MMF), azathioprine (AZA), and corticosteroids. Rapamune was initiated with a single loading dose of 12-20 mg, after which dosing was adjusted to achieve a target sirolimus whole blood trough concentration of 8-20 ng/mL (chromatographic method). The primary efficacy endpoint was calculated GFR at 12 months post-randomization. Secondary endpoints included biopsy-confirmed acute rejection, graft loss, and death. Enrollment in the patient stratum with baseline calculated GFR less than 40 mL/min was discontinued due to an imbalance in safety events (see Precautions and Adverse Reactions). Findings in the patient stratum with baseline calculated GFR greater than 40 mL/min (Rapamune conversion, n = 497; CNI continuation, n = 246) are summarized as follows: There was no clinically or statistically significant improvement in Nankivell GFR compared to baseline. (See Table 8.)
Click on icon to see table/diagram/image
In the patient stratum with baseline calculated GFR greater than 40 mL/min (Rapamune conversion, n = 497; CNI continuation, n = 246), renal function and the rates of acute rejection, graft loss, and death were similar at 1 and 2 years. Treatment-emergent adverse events occurred more frequently during the first 6 months after Rapamune conversion. The rates of pneumonia were significantly higher for the sirolimus conversion group.
While the mean and median values for urinary protein to creatinine ratio were similar between treatment groups at baseline, significantly higher mean and median levels of urinary protein excretion were seen in the Rapamune conversion arm at 1 year and at 2 years, as shown in the table as follows. In addition, when compared to patients who continued to receive calcineurin inhibitors, a higher percentage of patients had urinary protein to creatinine ratios >1 at 1 and 2 years after sirolimus conversion. This difference was seen in both patients who had a urinary protein to creatinine ratio ≤1 and those who had a protein to creatinine ratio >1 at baseline. More patients in the sirolimus conversion group developed nephrotic range proteinuria, as defined by a urinary protein to creatinine ratio >3.5 (46/482 [9.5%] versus 9/239 [3.8%]), even when the patients with baseline nephrotic range proteinuria were excluded. The rate of nephrotic range proteinuria was significantly higher in the sirolimus conversion group compared to the calcineurin inhibitor continuation group with baseline urinary protein to creatinine ratio >1 (13/29 versus 1/14), excluding patients with baseline nephrotic range proteinuria. (See Table 9.)
Click on icon to see table/diagram/image
The previous information should be taken into account when considering conversion from calcineurin inhibitors to Rapamune in stable renal transplant patients due to the lack of evidence showing that renal function improves following conversion, and the finding of a greater increment in urinary protein excretion, and an increased incidence of treatment-emergent nephrotic range proteinuria following conversion to Rapamune. This was particularly true among patients with existing abnormal urinary protein excretion prior to conversion.
In the stratum with baseline calculated GFR greater than 40 mL/min, the mean and median values for urinary protein to creatinine ratio were similar between treatment groups at baseline (mean: 0.35 and 0.28; median: 0.13 and 0.11 for the Rapamune conversion and CNI continuation groups, respectively). At 24 months, the mean and median urinary protein to creatinine ratios were significantly higher in the Rapamune conversion group as compared to those of the (CNI) continuation group (mean: 0.87 and 0.48, p<0.002; median: 0.33 and 0.13, p<0.001, for the Rapamune conversion and CNI continuation groups, respectively) (see Precautions). New-onset nephrosis (nephrotic syndrome) was also reported (see Adverse Reactions).
At 2 years, the rate of non-melanoma skin malignancies was significantly lower in the Rapamune conversion group as compared to the CNI continuation group (1.8% and 6.9%, respectively, p<0.001). This difference in skin malignancy rates persisted after exclusion of patients with a prior history of skin malignancies (0.7% and 4.1% for the Rapamune conversion and CNI continuation groups, respectively, p<0.002). It should be noted that Study 4 was not designed to consider malignancy risk factors or systematically screen subjects for malignancy.
In a subset of study patients with a baseline GFR greater than 40 mL/min and normal urinary protein excretion, calculated GFR was higher at 1 and 2 years in patients converted to Rapamune (n = 197) than for the corresponding subset of CNI continuation patients (n = 102). The rates of acute rejection, graft loss, and death were similar, but urinary protein excretion was increased in the Rapamune treatment arm of the subset.
In an open-label, randomized, comparative, multicenter study where renal transplant patients were either converted from tacrolimus to sirolimus 3 to 5 months post-transplant or remained on tacrolimus, there was no significant difference in renal function at 2 years. There were more adverse events (99.2% versus 91.1%, p=0.002) and more discontinuations from the treatment due to adverse events (26.7% versus 4.1%, p<0.001) in the group converted to sirolimus compared to the tacrolimus group. The incidence of biopsy-confirmed acute rejection was higher (p=0.020) for patients in the sirolimus group (11, 8.4%) compared to the tacrolimus group (2, 1.6%) through 2 years; most rejections were mild in severity (8 of 9 [89%] T-cell BCAR, 2 of 4 [50%] antibody-mediated BCAR) in the sirolimus group. Patients who had both antibody-mediated rejection and T-cell-mediated rejection on the same biopsy were counted once for each category. More patients converted to sirolimus developed new onset diabetes mellitus defined as 30 days or longer of continuous or at least 25 days non-stop (without gap) use of any diabetic treatment after randomization, a fasting glucose ≥126 mg/dL or a non-fasting glucose ≥200 mg/dL after randomization (18.3% versus 5.6%, p=0.025). A lower incidence of squamous cell carcinoma of the skin was observed in the sirolimus group (0% versus 4.9%).
Rapamune was studied in a one-year, randomized, open-label, controlled clinical trial in high risk patients who were defined as Black transplant recipients and/or repeat renal transplant recipients who lost a previous allograft for immunologic reason and/or patients with high-panel reactive antibodies (PRA; peak PRA level >80%). Patients were randomized 1:1 to concentration-controlled sirolimus and tacrolimus or concentration-controlled sirolimus and cyclosporine (MODIFIED), and both groups received corticosteroids per local practice. Antibody induction was allowed per protocol as prospectively defined at each transplant center, and was used in 85.3% of patients. The study was conducted at 35 centers in the United States. Baseline demography was well-balanced in both groups; 77.7% of those receiving sirolimus and tacrolimus were Black, and 77.2% of those receiving sirolimus and cyclosporine were Black. The evaluable intention-to-treat population (defined as all patients who were randomized and received a transplant, and at least one dose of study medication) included 224 patients who received sirolimus and tacrolimus and 224 patients who received sirolimus and cyclosporine. The co-primary endpoints, all measured at 12 months in the evaluable ITT population, were efficacy failure (defined as the first occurrence of biopsy-confirmed acute rejection, graft loss, or death), first occurrence of graft loss or death, and renal function as measured by the calculated GFR using the Nankivell formula. The table as follows summarizes the co-primary endpoints. The overall rates of efficacy failure and the first occurrence of graft loss or death were similar in both groups. (See Table 10.)
Click on icon to see table/diagram/image
Patient survival at 12 months was 95.1% in patients who received sirolimus and tacrolimus versus 94.6% in patients who received sirolimus and cyclosporine. The incidence of biopsy-confirmed acute rejection was 13.8% in patients who received sirolimus and tacrolimus versus 17.4% in patients who received sirolimus and cyclosporine. Although acute rejection was numerically lower in patients who received sirolimus and tacrolimus, the severity of rejection was statistically greater compared with those who received sirolimus and cyclosporine. On-therapy renal function was consistently higher in patients who received sirolimus and tacrolimus as compared with patients who received sirolimus and cyclosporine.
A clinical study in liver transplant patients randomized to conversion from a CNI-based regimen to a sirolimus-based regimen versus continuation of a CNI-based regimen 6-144 months post-liver transplantation failed to demonstrate superiority in baseline-adjusted GFR at 12 months (-4.45 mL/min and -3.07 mL/min, respectively). The study also failed to demonstrate non-inferiority of the rate of combined graft loss, missing survival data, or death for the sirolimus conversion group compared to the CNI continuation group. The number of deaths in the sirolimus conversion group was higher than the CNI continuation group, although the difference was not statistically significant. The rates of premature study discontinuation, adverse events overall (and infections, specifically), and biopsy-proven acute liver graft rejection at 12 months were all significantly greater in the sirolimus conversion group compared to the CNI continuation group.
Rapamune was evaluated in a 36-month, open-label, randomized, controlled clinical trial at 14 North American centers in pediatric (aged 3 to <18 years) renal transplant recipients considered to be at high immunologic risk for developing chronic allograft nephropathy, defined as a history of one or more acute allograft rejection episodes and/or the presence of chronic allograft nephropathy on a renal biopsy. Seventy-eight (78) subjects were randomized in a 2:1 ratio to Rapamune (sirolimus target concentrations of 5 to 15 ng/mL, by chromatographic assay, n = 53) in combination with a calcineurin inhibitor and corticosteroids or to continue calcineurin-inhibitor-based immunosuppressive therapy (n = 25). The primary endpoint of the study was efficacy failure as defined by the first occurrence of biopsy-confirmed acute rejection, graft loss, or death, and the trial was designed to show superiority of Rapamune added to a calcineurin-inhibitor-based immunosuppressive regimen compared to a calcineurin-inhibitor-based regimen. The cumulative incidence of efficacy failure up to 36 months was 45.3% in the Rapamune group compared to 44.0% in the control group, and did not demonstrate superiority. There was one death in each group. The use of Rapamune in combination with calcineurin inhibitors and corticosteroids was associated with an increased risk of deterioration of renal function, serum lipid abnormalities (including but not limited to increased serum triglycerides and cholesterol), and urinary tract infections. This study does not support the addition of Rapamune to calcineurin-inhibitor-based immunosuppressive therapy in this subpopulation of pediatric renal transplant patients (see Dosage & Administration and Pharmacokinetics as follows).
Disclaimer: Data on Rapamune Oral Solution is provided only as a reference and Rapamune Oral Solution is not marketed in Malaysia.
Pharmacokinetics: Absorption: Following administration of Rapamune oral solution, sirolimus is rapidly absorbed, with a mean time-to-peak concentration (t
max) of approximately 1 hour after a single dose of Rapamune in healthy subjects and approximately 2 hours after multiple oral doses of Rapamune in renal transplant recipients. Following administration of Rapamune tablet, sirolimus t
max was approximately 3 hours after single doses in healthy volunteers and multiple doses in renal transplant patients.
The systemic availability (F) of sirolimus from Rapamune oral solution was estimated to be approximately 14%. After Rapamune tablet administration, F was estimated to be approximately 17%. Bioequivalence between 1 mg, 2 mg, and 5 mg tablets has been generally shown in healthy volunteers. The exception was that t
max was longer for the 5 mg tablets compared with the other tablets.
Sirolimus concentrations are dose proportional between 3 and 12 mg/m
2 after administration of Rapamune oral solution in stable renal transplant patients, and between 5 and 40 mg after administration of Rapamune tablets in healthy volunteers.
Distribution: The mean (± SD) blood-to-plasma ratio of sirolimus was 36 (± 17.9) in stable renal allograft recipients after administration of Rapamune oral solution, indicating that sirolimus is extensively partitioned into formed blood elements. The mean volume of distribution (Vss/F) of sirolimus by Rapamune oral solution is 12 ± 7.52 L/kg. Sirolimus is extensively bound (approximately 92%) to human plasma proteins.
In human whole blood, the binding of sirolimus was shown mainly to be associated with serum albumin (97%), α1-acid glycoprotein, and lipoproteins.
Metabolism: Sirolimus is a substrate for both CYP3A4 and P-glycoprotein. Sirolimus is extensively metabolized by O-demethylation and/or hydroxylation. Seven major metabolites, including hydroxy-, demethyl-, and hydroxydemethyl, are identifiable in whole blood. Some of these metabolites are also detectable in plasma, fecal, and urine samples. The glucuronide and sulfate conjugates are not present in any of the biologic matrices. Sirolimus is the major component in human whole blood and contributes to greater than 90% of the immunosuppressive activity.
Elimination: After a single dose of [
14C]sirolimus by oral solution in healthy subjects, the majority (91%) of radioactivity was recovered from the feces, and only a minor amount (2.2%) was excreted in urine. The mean ± SD terminal elimination half-life (t
½) of sirolimus after multiple dosing by Rapamune oral solution in stable renal transplant patients was estimated to be about 62 ± 16 hours.
Effect of Food: In 22 healthy subjects, a high fat breakfast (860 kcal, 55% kcal from fat) altered the bioavailability characteristics of sirolimus after administration by Rapamune oral solution. Compared to fasting, a 34% decrease in the peak blood sirolimus concentration (C
max), a 3.5-fold increase in the time to peak concentration (t
max), and a 35% increase in mean total exposure (AUC) was observed. In an otherwise identical study, Rapamune was administered by tablet to 24 healthy subjects. The values for C
max, t
max, and AUC showed increases of 65%, 32%, and 23%, respectively. Thus, a high-fat meal produced differences in the two formulations with respect to rate of absorption but not in extent of absorption. Evidence from a large randomized multicenter controlled trial comparing Rapamune oral solution to tablets supports that the differences in absorption rates do not effect the efficacy of the drug.
Rapamune should be taken consistently with or without food to minimize blood level variability. Bioequivalence testing based on AUC and C
max showed that Rapamune administered with orange juice is equivalent to administration with water. Therefore, orange juice and water may be used interchangeably to dilute Rapamune for oral solution. Grapefruit juice reduces CYP3A4-mediated drug metabolism and potentially enhances P-gp mediated drug counter transport from enterocytes of the small intestine and must not be taken with Rapamune (see Interactions).
Renal transplant patients: Mean (± SD) pharmacokinetic parameters for sirolimus given daily by Rapamune oral solution in combination with cyclosporine and corticosteroids in renal transplant patients were determined at months 1, 3, and 6 after transplantation. There were no significant differences in C
max, t
max, AUC, or CL/F with respect to treatment group or month.
After daily administration of Rapamune in renal transplant patients by oral solution and tablet, estimates of C
max, AUC, and CL/F did not appear to be different; but t
max was significantly different.
Upon repeated twice daily administration of Rapamune oral solution without an initial loading dose in a multiple-dose study, the average trough concentration of sirolimus increased approximately 2- to 3-fold over the initial 6 days of therapy at which time steady-state was reached. Mean whole blood sirolimus trough concentrations in patients receiving Rapamune by tablet with a loading dose of three times the maintenance dose achieved steady-state concentrations within 24 hours after the start of dose administration.
High-risk patients: Average Rapamune doses and sirolimus whole blood trough concentrations for tablets administered daily in combination with cyclosporine or tacrolimus, and corticosteroids in high-risk renal transplant patients (see Pharmacodynamics previously) are summarized in the table as follows. (See Table 11.)
Click on icon to see table/diagram/image
Patients treated with the combination of Rapamune and tacrolimus required larger Rapamune doses to achieve the target sirolimus concentrations than patients treated with the combination of Rapamune and cyclosporine.
The pharmacokinetic parameters of sirolimus in adult renal transplant patients following multiple dosing with Rapamune 2 mg daily, in combination with cyclosporine and corticosteroids, is summarized in the following table. (See Table 12.)
Click on icon to see table/diagram/image
Whole blood trough sirolimus concentrations, as measured by LC/MS/MS in renal transplant patients, were significantly correlated with AUCτ,ss. Upon repeated, twice-daily administration without an initial loading dose in a multiple-dose study, the average trough concentration of sirolimus increases approximately 2- to 3-fold over the initial 6 days of therapy, at which time steady-state is reached. A loading dose of 3 times the maintenance dose will provide near steady-state concentrations within 1 day in most patients.
Sirolimus Concentrations (Chromatographic Equivalent) Observed in Phase 3 Clinical Studies: The following sirolimus concentrations (chromatographic equivalent) were observed in phase 3 clinical studies (see Pharmacodynamics previously). (See Table 13.)
Click on icon to see table/diagram/image
The withdrawal of cyclosporine and concurrent increases in sirolimus trough concentrations to steady-state required approximately 6 weeks. Following cyclosporine withdrawal, larger Rapamune doses were required due to the absence of the inhibition of sirolimus metabolism and transport by cyclosporine and to achieve higher target sirolimus trough concentrations during concentration-controlled administration.
Patients with Renal Impairment: There is minimal renal excretion of the drug or its metabolites. The pharmacokinetics of sirolimus would be expected to be similar in various populations with renal function ranging from normal to absent (dialysis patients).
Patients with Hepatic Impairment: The rate of absorption of sirolimus was not altered by hepatic disease, as evidenced by no changes in C
max and t
max values. The maintenance dose of Rapamune should be reduced by approximately one third in patients with mild to moderate hepatic impairment and by approximately one half in patients with severe hepatic impairment (see Dosage and Administration). In patients with hepatic impairment, it is necessary that sirolimus whole blood trough levels be monitored. In patients with severe hepatic impairment, consideration should be given to monitoring every 5 to 7 days for a longer period of time after dose adjustment or after loading dose due to the delay in reaching steady-state because of the prolonged half-life.
Children: Sirolimus pharmacokinetic data were collected in concentration-controlled trials of pediatric renal transplant patients who were also receiving cyclosporine and corticosteroids. The target ranges for trough concentrations were either 10 - 20 ng/mL for the 21 children receiving tablets. The children aged 6 - 11 years (n = 8) received mean ± SD doses of 1.75 ± 0.71 mg/day (0.064 ± 0.018 mg/kg, 1.65 ± 0.43 mg/m
2).
The children aged 12 - 18 years (n = 14) received mean ± SD doses of 2.79 ± 1.25 mg/day (0.053 ± 0.0150 mg/kg, 1.86 ± 0.61 mg/m
2). At the time of sirolimus blood sampling for pharmacokinetic evaluation, the majority (80%) of these pediatric patients received the sirolimus dose at 16 hours after the once daily cyclosporine dose. (See Table 14.)
Click on icon to see table/diagram/image
Elderly: Clinical studies of Rapamune did not include a sufficient number of patients >65 years of age to determine whether they will respond differently than younger patients.
Gender: Rapamune oral dose clearance after Rapamune oral solution in males was 12% lower than that in females; male subjects had a significantly longer t
½ than did female subjects (72.3 hours versus 61.3 hours). Similar gender effects on oral-dose clearance and t
½ were obtained after administration of Rapamune by tablets. These pharmacokinetic differences do not require dose adjustment based on gender.
Race: In large phase III trials using Rapamune and cyclosporine microemulsion [(cyclosporine, USP) MODIFIED], there were no significant differences in mean trough sirolimus concentrations or AUC over time between Black (n = 139) and Non-Black (n = 724) patients during the first 6 months after transplantation at Rapamune doses of 2 mg/day.
Disclaimer: Data on Rapamune Oral Solution is provided only as a reference and Rapamune Oral Solution is not marketed in Malaysia.
Toxicology: Preclinical safety data: Carcinogenicity: Carcinogenicity studies were conducted in mice and rats. In an 86-week female mouse study at 4 dosages that were approximately 16 to 135 times the clinical doses (adjusted for body surface area) there was a statistically significant increase in malignant lymphoma at all dose levels compared with controls. In a second mouse study at dosages that were approximately 3 to 16 times the clinical doses (adjusted for body surface area), hepatocellular adenoma and carcinoma (males) were considered sirolimus related. In the 104-week rat study at dosages that were approximately 0.4 to 1 times the clinical doses (adjusted for body surface area), there was a statistically significant increased incidence of testicular adenoma in the highest dose group.
Mutagenicity: Sirolimus was not genotoxic in the
in vitro bacterial reverse mutation assay, the Chinese hamster ovary cell chromosomal aberration assay, the mouse lymphoma cell forward mutation assay, or the
in vivo mouse micronucleus assay.
Reproductive Toxicology: Sirolimus was embryo/fetal toxic in rats at dosages of 0.1 mg/kg and above (approximately 0.2 to 0.5 the clinical doses adjusted for body surface area). Embryo/fetal toxicity was manifested as mortality and reduced fetal weights (with associated delays in skeletal ossification). However, no teratogenesis was evident. In combination with cyclosporine, rats had increased embryo/fetal mortality compared to sirolimus alone. There were no effects on rabbit development at the maternally toxic dosage of 0.05 mg/kg (approximately 0.3 to 0.8 times the clinical doses adjusted for body surface area).
There was no effect on fertility in female rats following the administration of sirolimus at dosages up to 0.5 mg/kg (approximately 1 to 3 times the clinical doses adjusted for body surface area). In male rats, there was a slight reduction in fertility compared to controls in one study at a dosage of 2 mg/kg (approximately 4 to 11 times the clinical doses adjusted for body surface area). A second study failed to confirm these findings. Reductions in testicular weights and/or histological lesions (e.g., tubular atrophy and tubular giant cells) were observed in rats following dosages of 0.65 mg/kg (approximately 1 to 3 times the clinical doses adjusted for body surface area) and above and in a monkey study at 0.1 mg/kg (approximately 0.4 to 1 times the clinical doses adjusted for body surface area) and above. Sperm counts were reduced in male rats following the administration of sirolimus for 13 weeks at a dosage of 6 mg/kg (approximately 12 to 32 times the clinical doses adjusted for body surface area), but showed improvement by 3 months after dosing was stopped.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image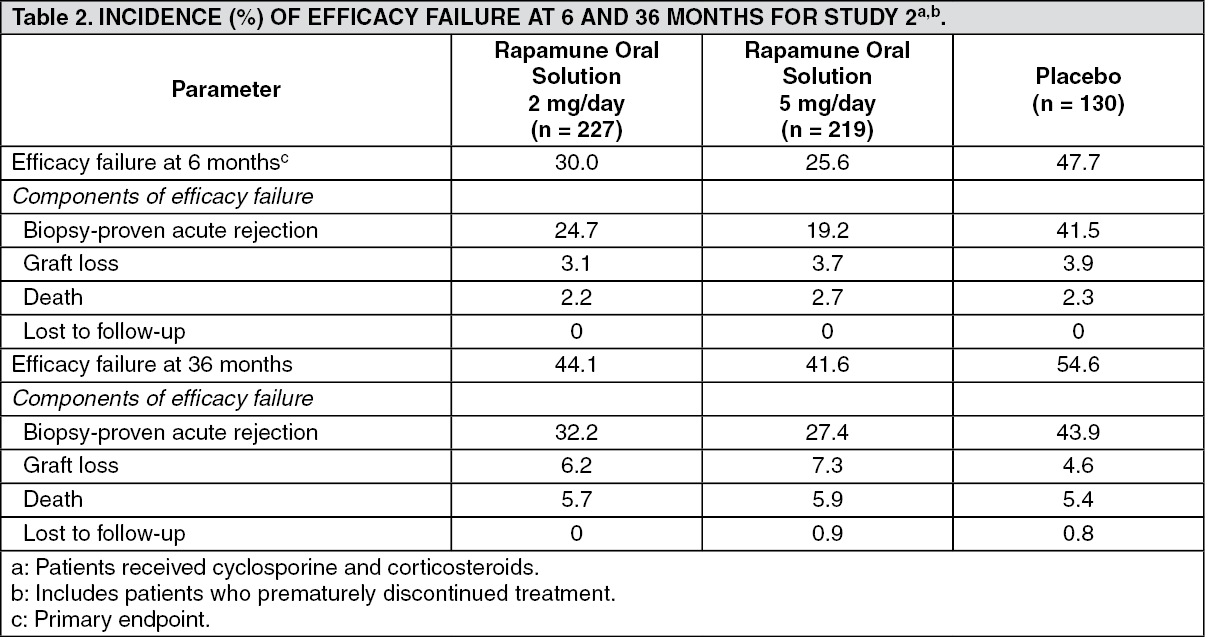 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image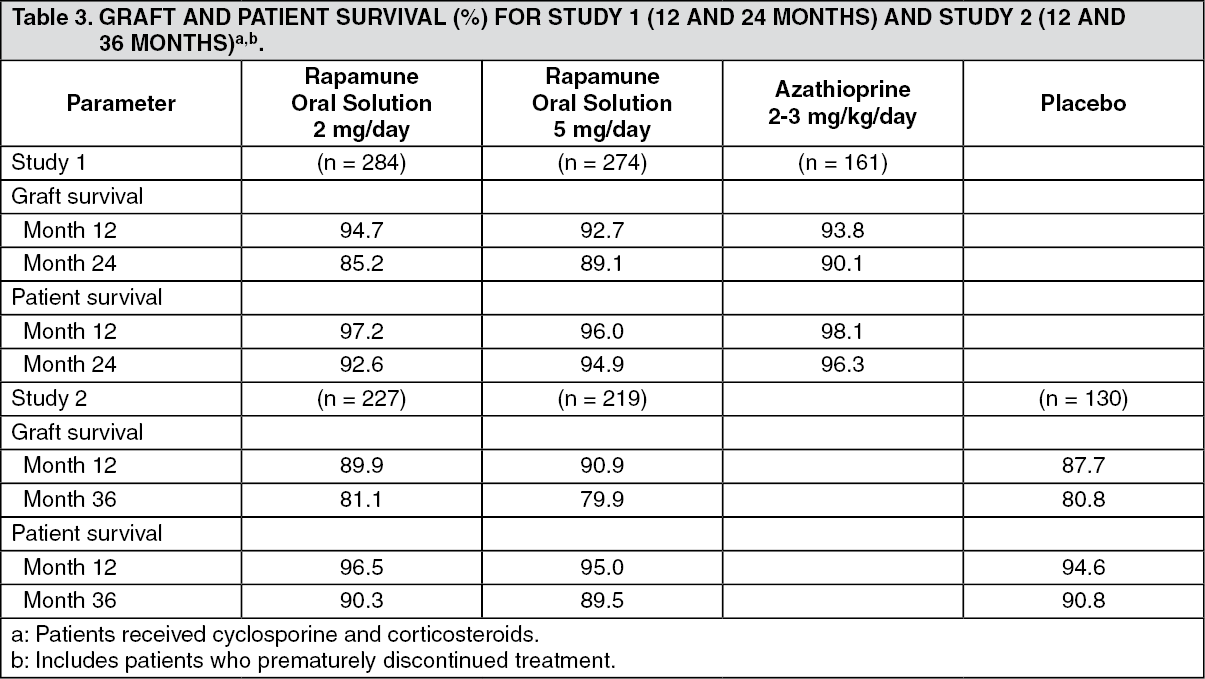 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image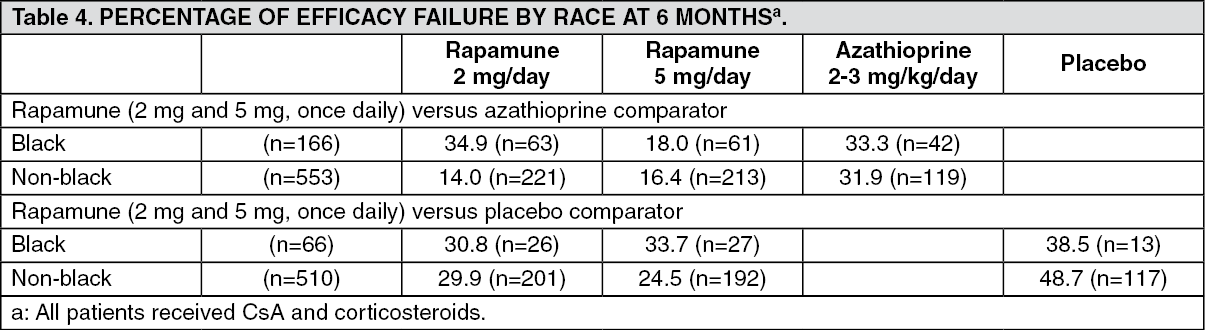 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image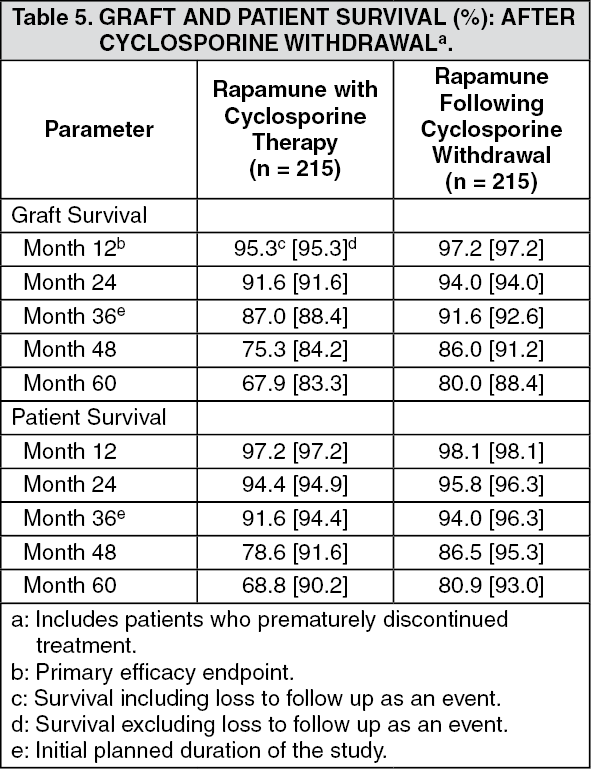 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image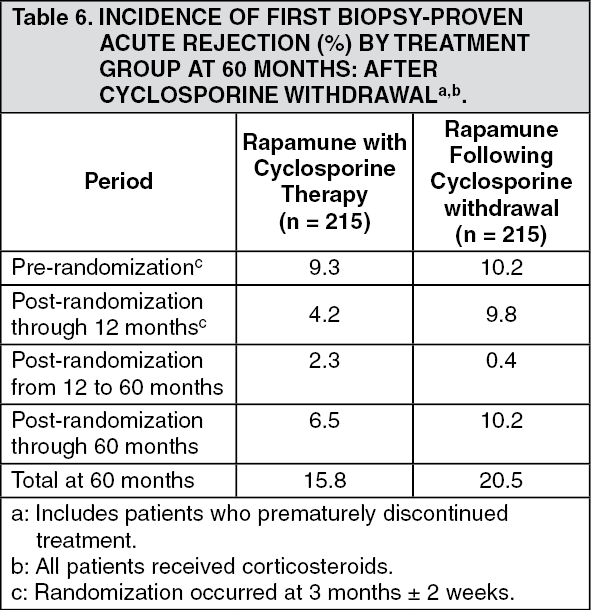 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image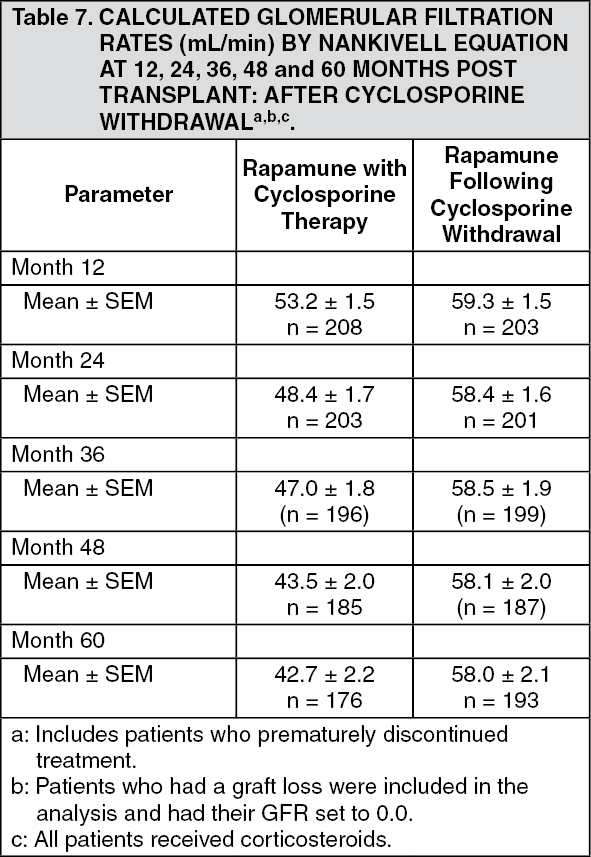 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image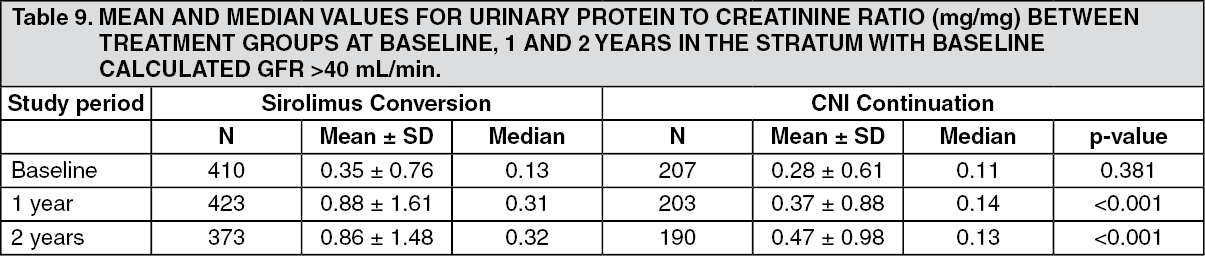 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image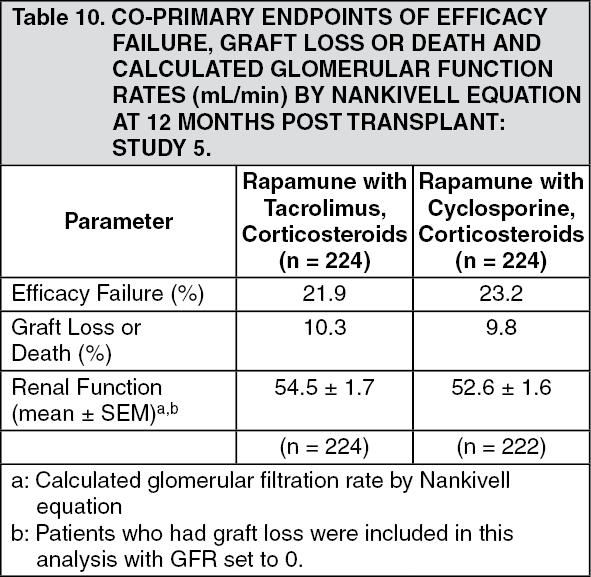 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image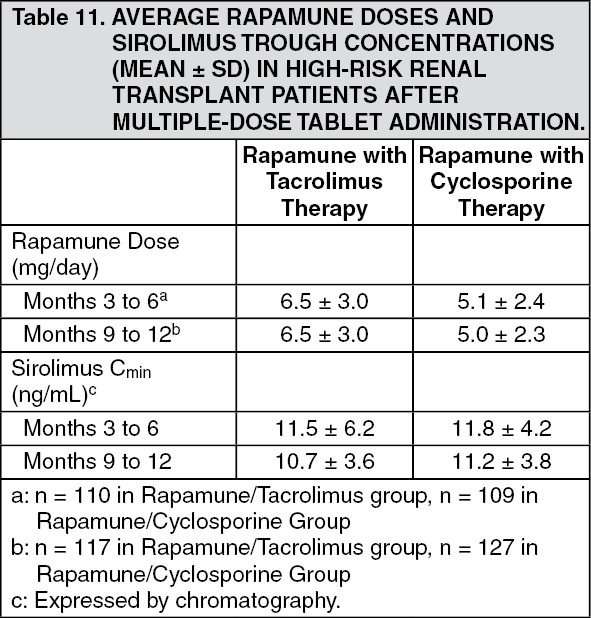 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image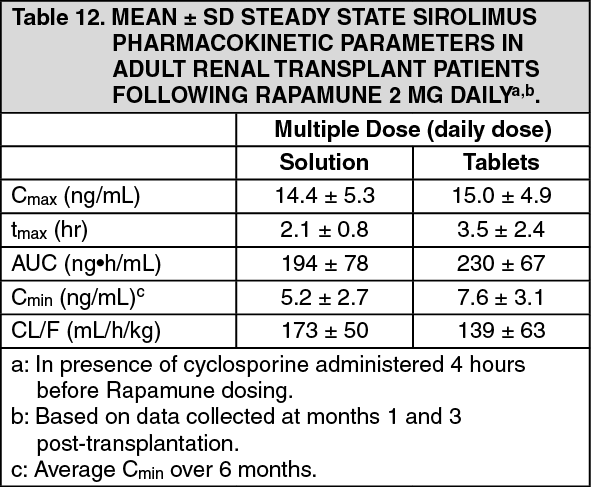 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image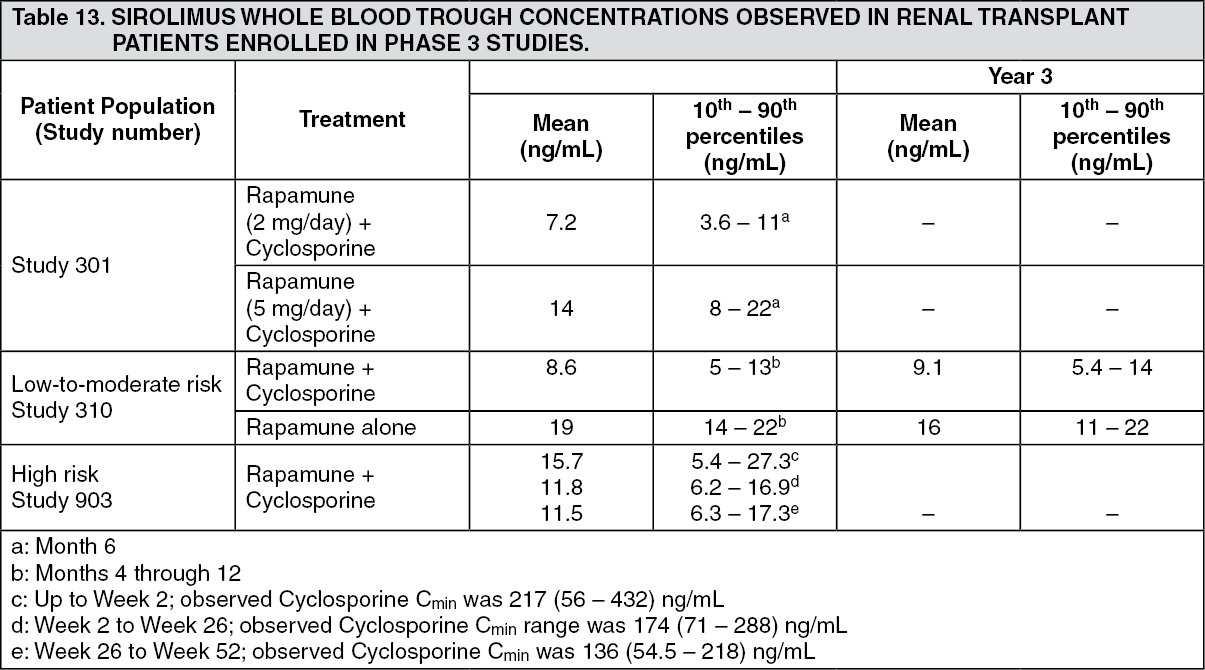 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image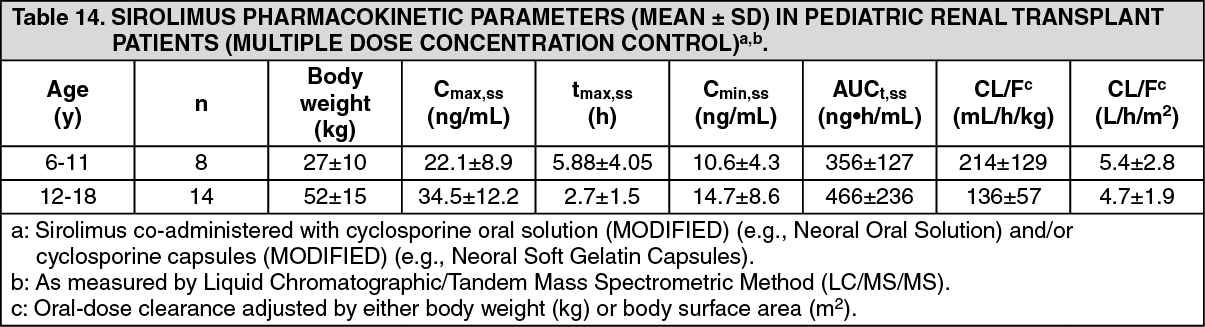 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image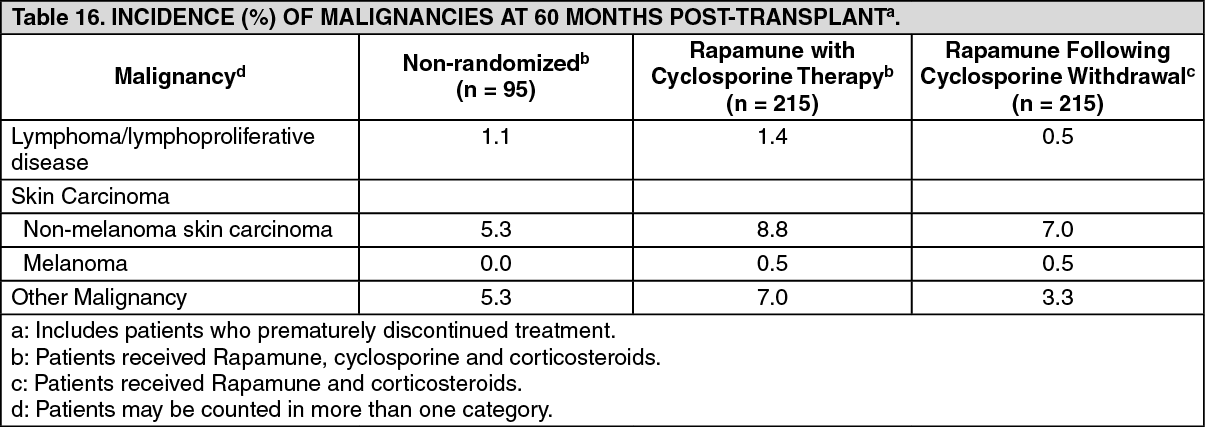 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
