


 Sign Out
Sign Out

Pemetrexed in combination with cisplatin: The recommended dose of Pemetrexed is 500mg/m2 of body surface area (BSA) administered as an intravenous infusion over 10 minutes on the first day of each 21-day cycle. The recommended dose of cisplatin is 75mg/m2 BSA infused over two hours approximately 30 minutes after completion of the pemetrexed infusion on the first day of each 21-day cycle. Patients must receive adequate anti-emetic treatment and appropriate hydration prior to and/or after receiving cisplatin.
Pemetrexed as single agent: In patients treated for non-small cell lung cancer after prior chemotherapy, the recommended dose of Pemetrexed is 500mg/m2 BSA administered as an intravenous infusion over 10 minutes on the first day of each 21-day cycle.
Pre-medication Regimen: To reduce the incidence and severity of skin reactions, a corticosteroid should be given the day prior to, on the day of, and the day after pemetrexed administration. The corticosteroid should be equivalent to 4mg of dexamethasone administered orally twice a day.
To reduce toxicity, patients treated with pemetrexed must also receive vitamin supplementation. Patients must take oral folic acid or a multivitamin containing folic acid (350 to 1,000 micrograms) on a daily basis. At least five doses of folic acid must be taken during the seven days preceding the first dose of pemetrexed, and dosing must continue during the full course of therapy and for 21 days after the last dose of pemetrexed. Patients must also receive an intramuscular injection of vitamin B12 (1,000 micrograms) in the week preceding the first dose of pemetrexed and once every three cycles thereafter. Subsequent vitamin B12 injections may be given on the same day as pemetrexed.
Monitoring: Patients receiving pemetrexed should be monitored before each dose with a complete blood count, including a differential white cell count (WCC) and platelet count. Prior to each chemotherapy administration, blood chemistry tests should be collected to evaluate renal and hepatic function. Before the start of any cycle of chemotherapy, patients are required to have the following: absolute neutrophil count (ANC) should be ≥ 1,500 cells/mm3 and platelets should be ≥ 100,000 cells/mm3.
Creatinine clearance should be ≥ 45ml/min.
The total bilirubin should be ≤ 1.5-times upper limit of normal. Alkaline phosphatase (AP), aspartate aminotransferase (AST or SGOT), and alanine aminotransferase (ALT or SGPT) should be ≤ 3-times upper limit of normal. Alkaline phosphatase, AST, and ALT ≤ 5-times upper limit of normal is acceptable if liver has tumour involvement.
Dose Adjustments: Dose adjustments at the start of a subsequent cycle should be based on nadir haematologic counts or maximum non-haematologic toxicity from the preceding cycle of therapy. Treatment may be delayed to allow sufficient time for recovery. Upon recovery, patients should be re-treated using the guidelines in Tables 1, 2, and 3, which are applicable for Pemetrexed used as a single agent or in combination with cisplatin. (See Table 1.)
 Click on icon to see table/diagram/image
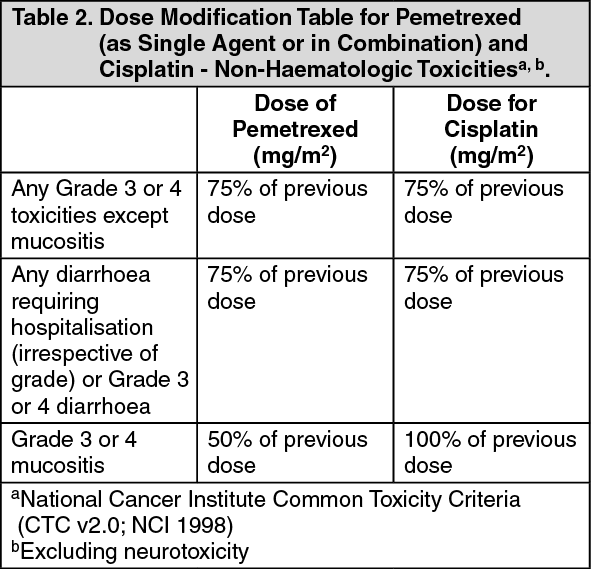
Click on icon to see table/diagram/imageIf patients develop non-haematologic toxicities ≥ Grade 3 (excluding neurotoxicity), Pemetrexed should be withheld until resolution to less than or equal to the patient's pre-therapy value. Treatment should be resumed according to the guidelines in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
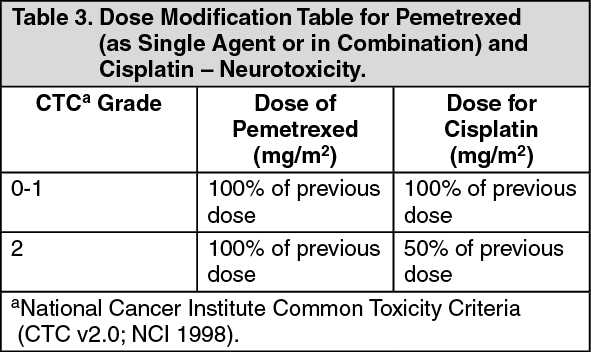
Click on icon to see table/diagram/imageIn the event of neurotoxicity, the recommended dose adjustment for Pemetrexed and cisplatin is documented in Table 3. Patients should discontinue therapy if Grade 3 or 4 neurotoxicity is observed. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTreatment with Pemetrexed should be discontinued if a patient experiences any haematologic or non-haematologic Grade 3 or 4 toxicity after 2 dose reductions or immediately if Grade 3 or 4 neurotoxicity is observed.
Elderly: In clinical studies, there has been no indication that patients 65 years of age or older are at increased risk of adverse events compared to patients younger than 65 years old. No dose reductions other than those recommended for all patients are necessary.
Paediatric population: There is no relevant use of Pemetrexed in the paediatric population in malignant pleural mesothelioma and non-small cell lung cancer.
Patients with renal impairment (standard Cockcroft and Gault formula or Glomerular Filtration Rate measured Tc99m DPTA serum clearance method): Pemetrexed is primarily eliminated unchanged by renal excretion. In clinical studies, patients with creatinine clearance of ≥ 45ml/min required no dose adjustments other than those recommended for all patients. There are insufficient data on the use of pemetrexed in patients with creatinine clearance below 45ml/min; therefore, the use of pemetrexed is not recommended.
Patients with hepatic impairment: No relationships between AST (SGOT), ALT (SGPT), or total bilirubin and pemetrexed pharmacokinetics were identified. However, patients with hepatic impairment, such as bilirubin > 1.5-times the upper limit of normal and/or aminotransferase > 3.0-times the upper limit of normal (hepatic metastases absent) or > 5.0-times the upper limit of normal (hepatic metastases present), have not been specifically studied.
Method of administration: Pemetrexed should be administered as an intravenous infusion over 10 minutes on the first day of each 21-day cycle. For instructions on reconstitution and dilution of Pemetrexed before administration, see Preparation and administration instructions under Cautions for Usage.