Active Ingredient: Each film coated tablet contains: Clopidogrel Bisulphate (Clopidogrel 75 mg): 97.875 mg.
Clopidogrel Bisulphate (Clopidogrel 300 mg): 391.5 mg.
Pharmacotherapeutic group: Platelet aggregation inhibitors.
Pharmacology: Pharmacodynamics: Mechanism of action: Clopidogrel is a prodrug, one of whose metabolites is an inhibitor of platelet aggregation. Clopidogrel must be metabolised by CYP450 enzymes to produce the active metabolite that inhibits platelet aggregation. The active metabolite of clopidogrel selectively inhibits the binding of adenosine diphosphate (ADP) to its platelet P2Y12 receptor and the subsequent ADP-mediated activation of the glycoprotein GPIIb/IIIa complex, thereby inhibiting platelet aggregation. Due to the irreversible binding, platelets exposed are affected for the remainder of their lifespan (approximately 7-10 days) and recovery of normal platelet function occurs at a rate consistent with platelet turnover. Platelet aggregation induced by agonists other than ADP is also inhibited by blocking the amplification of platelet activation by released ADP. Because the active metabolite is formed by CYP450 enzymes, some of which are polymorphic or subject to inhibition by other medicinal products, not all patients will have adequate platelet inhibition.
Pharmacodynamic effects: Repeated doses of 75 mg per day produced substantial inhibition of ADP-induced platelet aggregation from the first day; this increased progressively and reached steady state between Day 3 and Day 7. At steady state, the average inhibition level observed with a dose of 75 mg per day was between 40% and 60%. Platelet aggregation and bleeding time gradually returned to baseline values, generally within 5 days after treatment was discontinued.
Pharmacokinetics: Absorption: After single and repeated oral doses of 75 mg per day, clopidogrel is rapidly absorbed. Mean peak plasma levels of unchanged clopidogrel (approximately 2.2-2.5 ng/ml after a single 75 mg oral dose) occurred approximately 45 minutes after dosing. Absorption is at least 50%, based on urinary excretion of clopidogrel metabolites.
Distribution: Clopidogrel and the main circulating (inactive) metabolite bind reversibly in vitro to human plasma proteins (98% and 94% respectively). The binding is non-saturable in vitro over a wide concentration range.
Biotransformation: Clopidogrel is extensively metabolised by the liver. In vitro and in vivo, clopidogrel is metabolised according to two main metabolic pathways: one mediated by esterases and leading to hydrolysis into its inactive carboxylic acid derivative (85% of circulating metabolites), and one mediated by multiple cytochromes P450. Clopidogrel is first metabolised to a 2-oxo-clopidogrel intermediate metabolite. Subsequent metabolism of the 2-oxo-clopidogrel intermediate metabolite results in formation of the active metabolite, a thiol derivative of clopidogrel. The active metabolite is formed mostly by CYP2C19 with contributions from several other CYP enzymes, including CYP1A2, CYP2B6 and CYP3A4. The oxidative step is regulated primarily by Cytochrome P450 ISOENZYMES 2B6, 3A4, 1A1, 1A2 and 2C19. The active thiol metabolite which has been isolated in vitro, binds rapidly and irreversibly to platelet receptors, thus inhibiting platelet aggregation.
The Cmax of the active metabolite is twice as high following a single 300-mg clopidogrel loading dose as it is after four days of 75-mg maintenance dose. Cmax occurs approximately 30 to 60 minutes after dosing.
Elimination: After a single oral dose of 75 mg, clopidogrel has a half-life of approximately 6 hours. The elimination half-life of the main circulating (inactive) metabolite was 8 hours after single and repeated administration.
Special populations: The pharmacokinetics of the active metabolite of clopidogrel is not known in these special populations.
Race: The prevalence of CYP2C19 alleles that result in intermediate and poor CYP2C19 metabolism differs according to race/ethnicity. From literature, limited data in Asian populations are available to assess the clinical implication of genotyping of this CYP on clinical outcome events.
Plax Film Coated Tablet 75 mg: Secondary prevention of atherothrombotic events.
Clopidogrel is indicated in: Adult patients suffering from myocardial infarction (from a few days until less than 35 days), ischaemic stroke (from 7 days until less than 6 months) or established peripheral arterial disease.
Adult patients suffering from acute coronary syndrome: Non-ST segment elevation acute coronary syndrome (unstable angina or non-Q-wave myocardial infarction), including patients undergoing a stent placement following percutaneous coronary intervention, in combination with acetylsalicylic acid (ASA).
ST segment elevation acute myocardial infarction, in combination with ASA in medically treated patients eligible for thrombolytic therapy.
Prevention of atherothrombotic and thromboembolic events in atrial fibrillation: In adult patients with atrial fibrillation who have at least one risk factor for vascular events, are not suitable for treatment with Vitamin K antagonists (VKA) and who have a low bleeding risk, clopidogrel is indicated in combination with ASA for the prevention of atherothrombotic and thromboembolic events, including stroke.
Plax Film Coated Tablet 300 mg: Secondary prevention of atherothrombotic events.
Clopidogrel is indicated in: Adult patients suffering from myocardial infarction (from a few days until less than 35 days), ischaemic stroke (from 7 days until less than 6 months) or established peripheral arterial disease.
Adult patients suffering from acute coronary syndrome: Non-ST segment elevation acute coronary syndrome (unstable angina or non-Q-wave myocardial infarction), including patients undergoing a stent placement following percutaneous coronary intervention, in combination with acetylsalicylic acid (ASA).
ST segment elevation acute myocardial infarction, in combination with ASA in medically treated patients eligible for thrombolytic therapy.
Posology: Adults and elderly: Plax film coated tablet 75 mg: Clopidogrel should be given as a single daily dose of 75 mg.
Plax film coated tablets 300 mg: Clopidogrel should be given as single daily dose of 300 mg. This 300 mg tablet of clopidogrel is intended for use as a loading dose for patient suffering from acute coronary syndrome.
In patients suffering from acute coronary syndrome: Non-ST segment elevation acute coronary syndrome (unstable angina or non-Q-wave myocardial infarction): Clopidogrel treatment should be initiated with a single 300-mg loading dose and then continued at 75 mg once a day (with acetylsalicylic acid (ASA) 75 mg-325 mg daily). Since higher doses of ASA were associated with higher bleeding risk it is recommended that the dose of ASA should not be higher than 100 mg. The optimal duration of treatment has not been formally established.
ST segment elevation acute myocardial infarction: Clopidogrel should be given as a single daily dose of 75 mg initiated with a 300-mg loading dose in combination with ASA and with or without thrombolytics. For patients over 75 years of age clopidogrel should be initiated without a loading dose. Combined therapy should be started as early as possible after symptoms start and continued for at least four weeks.
In patients with atrial fibrillation, clopidogrel should be given as a single daily dose of 75 mg. ASA (75-100 mg daily) should be initiated and continued in combination with clopidogrel.
If a dose is missed: Within less than 12 hours after regular scheduled time: Patients should take the dose immediately and then take the next dose at the regular scheduled time.
For more than 12 hours: Patients should take the next dose at the regular scheduled time and should not double the dose.
Paediatric population: Clopidogrel should not be used in children because of efficacy concerns.
Renal impairment: Therapeutic experience is limited in patients with renal impairment.
Hepatic impairment: Therapeutic experience is limited in patients with moderate hepatic disease who may have bleeding diatheses.
Route of Administration: For oral use. It may be given with or without food.
Overdose following clopidogrel administration may lead to prolonged bleeding time and subsequent bleeding complications. Appropriate therapy should be considered if bleedings are observed.
No antidote to the pharmacological activity of clopidogrel has been found. If prompt correction of prolonged bleeding time is required, platelet transfusion may reverse the effects of clopidogrel.
Hypersensitivity to the active substance or to any of the excipients.
Severe hepatic impairment.
Active pathological bleeding such as peptic ulcer or intracranial haemorrhage.
Bleeding and haematological disorders: Due to the risk of bleeding and haematological adverse reactions, blood cell count determination and/or other appropriate testing should be promptly considered whenever clinical symptoms suggestive of bleeding arise during the course of treatment. As with other antiplatelet agents, clopidogrel should be used with caution in patients who may be at risk of increased bleeding from trauma, surgery or other pathological conditions and in patients receiving treatment with ASA, heparin, glycoprotein IIb/IIIa inhibitors or non-steroidal anti-inflammatory drugs (NSAIDs) including COX-2 inhibitors, or selective serotonin reuptake inhibitors (SSRIs), or other medicinal products associated with bleeding risk such as pentoxifylline. Patients should be followed carefully for any signs of bleeding including occult bleeding, especially during the first weeks of treatment and/or after invasive cardiac procedures or surgery. The concomitant administration of clopidogrel with oral anticoagulants is not recommended since it may increase the intensity of bleedings.
If a patient is to undergo elective surgery and antiplatelet effect is temporarily not desirable, clopidogrel should be discontinued 7 days prior to surgery. Patients should inform physicians and dentists that they are taking clopidogrel before any surgery is scheduled and before any new medicinal product is taken. Clopidogrel prolongs bleeding time and should be used with caution in patients who have lesions with a propensity to bleed (particularly gastrointestinal and intraocular).
Patients should be told that it might take longer than usual to stop bleeding when they take clopidogrel (alone or in combination with ASA), and that they should report any unusual bleeding (site or duration) to their physician.
Thrombotic Thrombocytopenic Purpura (TTP): Thrombotic Thrombocytopenic Purpura (TTP) has been reported very rarely following the use of clopidogrel, sometimes after a short exposure. It is characterised by thrombocytopenia and microangiopathic haemolytic anaemia associated with either neurological findings, renal dysfunction or fever. TTP is a potentially fatal condition requiring prompt treatment including plasmapheresis.
Acquired haemophilia: Acquired haemophilia has been reported following use of clopidogrel. In cases of confirmed isolated activated Partial Thromboplastin Time (aPTT) prolongation with or without bleeding, acquired haemophilia should be considered. Patients with a confirmed diagnosis of acquired haemophilia should be managed and treated by specialists, and clopidogrel should be discontinued.
Recent ischaemic stroke: In view of the lack of data, clopidogrel cannot be recommended during the first 7 days after acute ischaemic stroke.
Cytochrome P450 2C19 (CYP2C19): Pharmacogenetics: In patients who are poor CYP2C19 metabolisers, clopidogrel at recommended doses forms less of the active metabolite of clopidogrel and has a smaller effect on platelet function. Tests are available to identify a patient's CYP2C19 genotype.
Since clopidogrel is metabolised to its active metabolite partly by CYP2C19, use of medicinal products that inhibit the activity of this enzyme would be expected to result in reduced drug levels of the active metabolite of clopidogrel. The clinical relevance of this interaction is uncertain. As a precaution concomitant use of strong or moderate CYP2C19 inhibitors should be discouraged.
Cytochrome P450 22C19 (CYP22C19): Pharmacogenetics: Based on literature data, patients with genetically reduced CYP22C19 function (intermediate or poor metabolisers) have lower systemic exposure to the active metabolite of clopidogrel and diminished antiplatelet responses, and generally exhibit higher cardiovascular event rates following myocardial infarction than patients with normal CYP2C19 function.
CYP2C8 substrates: Caution is required in patients treated concomitantly with clopidogrel and CYP2C8 substrate medicinal products.
Cross-reactions among thienopyridines: Patients should be evaluated for history of hypersensitivity to thienopyridines (such as clopidogrel, ticlopidine, prasugrel) since cross-reactivity among thienopyridines has been reported. Thienopyridines may cause mild to severe allergic reactions such as rash, angioedema, or haematological cross-reactions such as thrombocytopaenia and neutropaenia. Patients who had developed a previous allergic reaction and/or haematological reaction to one thienopyridine may have an increased risk of developing the same or another reaction to another thienopyridine. Monitoring for signs of hypersensitivity in patients with a known allergy to thienopyridines is advised.
Renal impairment: Therapeutic experience with clopidogrel is limited in patients with renal impairment. Therefore clopidogrel should be used with caution in these patients.
Hepatic impairment: Experience is limited in patients with moderate hepatic disease who may have bleeding diatheses. Clopidogrel should therefore be used with caution in this population.
Effects on ability to drive and use machines: Clopidogrel has no or negligible influence on the ability to drive and use machines.
Pregnancy: As no clinical data on exposure to clopidogrel during pregnancy are available, it is preferable not to use clopidogrel during pregnancy as a precautionary measure.
Breast-feeding: It is unknown whether clopidogrel is excreted in human breast milk. As a precautionary measure, breast-feeding should not be continued during treatment with clopidogrel.
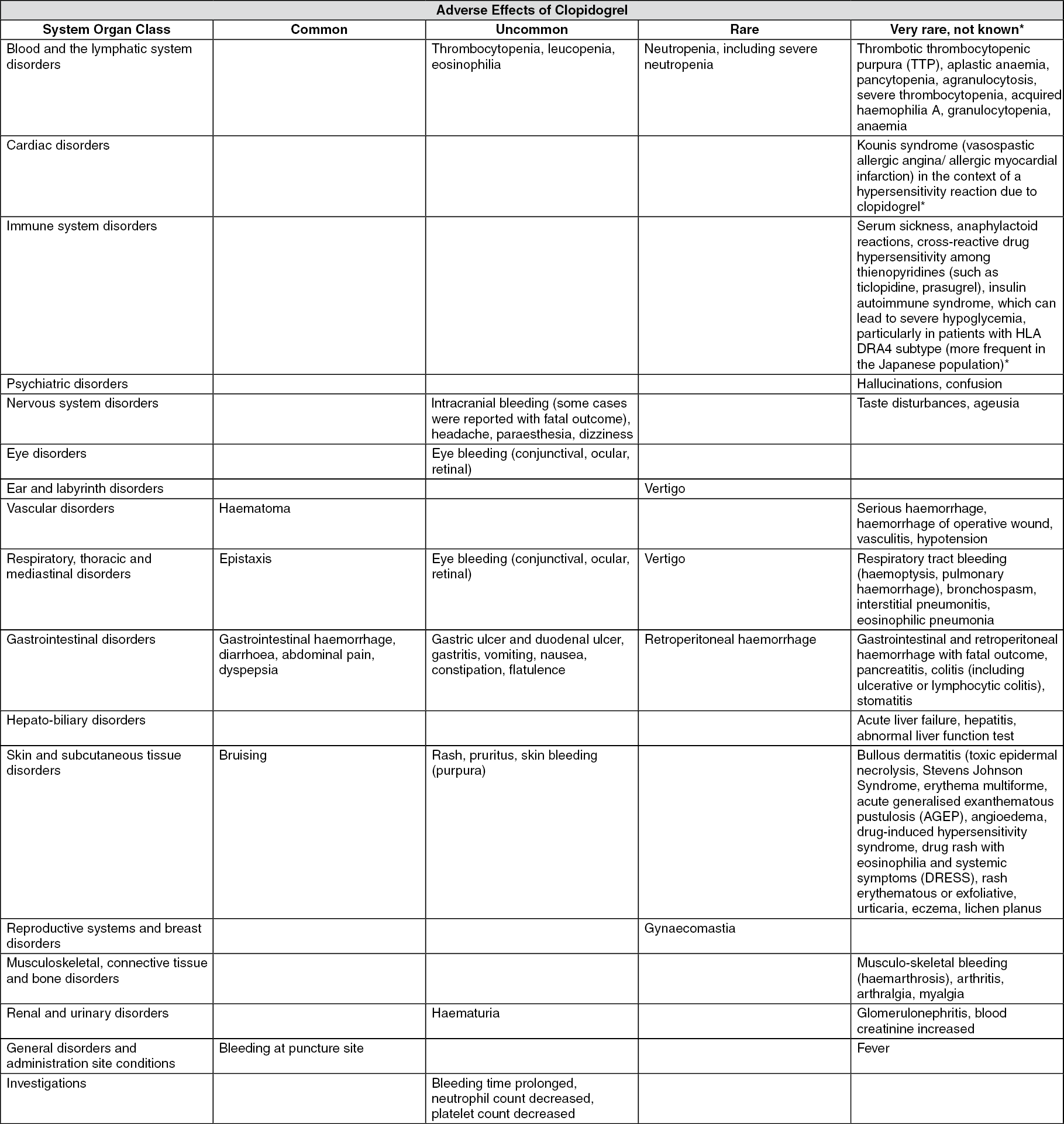
Bleeding is the most common reaction reported during the first month of treatment.
Tabulated list of adverse reactions: Within each system organ class, adverse reactions are presented in order of decreasing seriousness. (See table.)
 Click on icon to see table/diagram/image
Reporting of suspected adverse reactions:
Click on icon to see table/diagram/image
Reporting of suspected adverse reactions:
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
Medicinal products associated with bleeding risk: There is an increased risk of bleeding due to the potential additive effect. The concomitant administration of medicinal products associated with bleeding risk should be undertaken with caution.
Oral anticoagulants: The concomitant administration of clopidogrel with oral anticoagulants is not recommended since it may increase the intensity of bleedings.
Glycoprotein IIb/IIIa inhibitors: Clopidogrel should be used with caution in patients who receive concomitant glycoprotein IIb/IIIa inhibitors.
Acetylsalicylic acid (ASA): A pharmacodynamic interaction between clopidogrel and acetylsalicylic acid is possible, leading to increased risk of bleeding. Therefore, concomitant use should be undertaken with caution.
Heparin: Co-administration of heparin had no effect on the inhibition of platelet aggregation induced by clopidogrel. A pharmacodynamic interaction between clopidogrel and heparin is possible, leading to increased risk of bleeding. Therefore, concomitant use should be undertaken with caution.
Thrombolytics: The incidence of clinically significant bleeding was similar to that when thrombolytic agents and heparin are co-administered with ASA.
NSAIDs: The concomitant administration of clopidogrel and naproxen increased occult gastrointestinal blood loss. Consequently, NSAIDs including COX-2 inhibitors and clopidogrel should be co-administered with caution.
SSRIs: Since SSRIs affect platelet activation and increase the risk of bleeding, the concomitant administration of SSRIs with clopidogrel should be undertaken with caution.
Other concomitant therapy: Since clopidogrel is metabolised to its active metabolite partly by CYP2C19, use of medicinal products that inhibit the activity of this enzyme would be expected to result in reduced drug levels of the active metabolite of clopidogrel. As a precaution concomitant use of strong or moderate CYP2C19 inhibitors should be discouraged.
Medicinal products that are strong or moderate CYP2C19 inhibitors include, for example, omeprazole and esomeprazole, fluvoxamine, fluoxetine, moclobemide, voriconazole, fluconazole, ticlopidine, carbamazepine, and efavirenz.
Proton Pump Inhibitors (PPI): As a precaution, concomitant use of omeprazole or esomeprazole should be discouraged.
Clopidogrel can be administered with pantoprazole.
There is no evidence that other medicinal products that reduce stomach acid such as H2 blockers or antacids interfere with antiplatelet activity of clopidogrel.
CYP2C8 substrate medicinal products: Due to the risk of increased plasma concentrations, concomitant administration of clopidogrel and drugs primarily cleared by CYP2C8 metabolism (e.g., repaglinide, paclitaxel) should be undertaken with caution.
Store at temperature below 30°C. Protect it from light and moisture.
Shelf Life: 2 years.
B01AC04 - clopidogrel ; Belongs to the class of platelet aggregation inhibitors excluding heparin. Used in the treatment of thrombosis.
Plax FC tab 300 mg
10 × 10's;100 × 10's;3 × 10's;50 × 10's
Plax FC tab 75 mg
10 × 10's;100 × 10's;3 × 10's;50 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
