Pharmacotherapeutic group: anti-hypertensives, anti-hypertensives for pulmonary arterial hypertension.
ATC code: C02KX04.
Pharmacology: Pharmacodynamics: Mechanism of action: Endothelin (ET)-1 and its receptors (ETA and ETB) mediate a variety of effects such as vasoconstriction, fibrosis, proliferation, hypertrophy, and inflammation. In disease conditions such as PAH, the local ET system is upregulated and is involved in vascular hypertrophy and in organ damage.
Macitentan is an orally active potent endothelin receptor antagonist, active on both ETA and ETB receptors and approximately 100-fold more selective for ETA as compared to ETB in vitro. Macitentan displays high affinity and sustained occupancy of the ET receptors in human pulmonary arterial smooth muscle cells. This prevents endothelin-mediated activation of second messenger systems that result in vasoconstriction and smooth muscle cell proliferation.
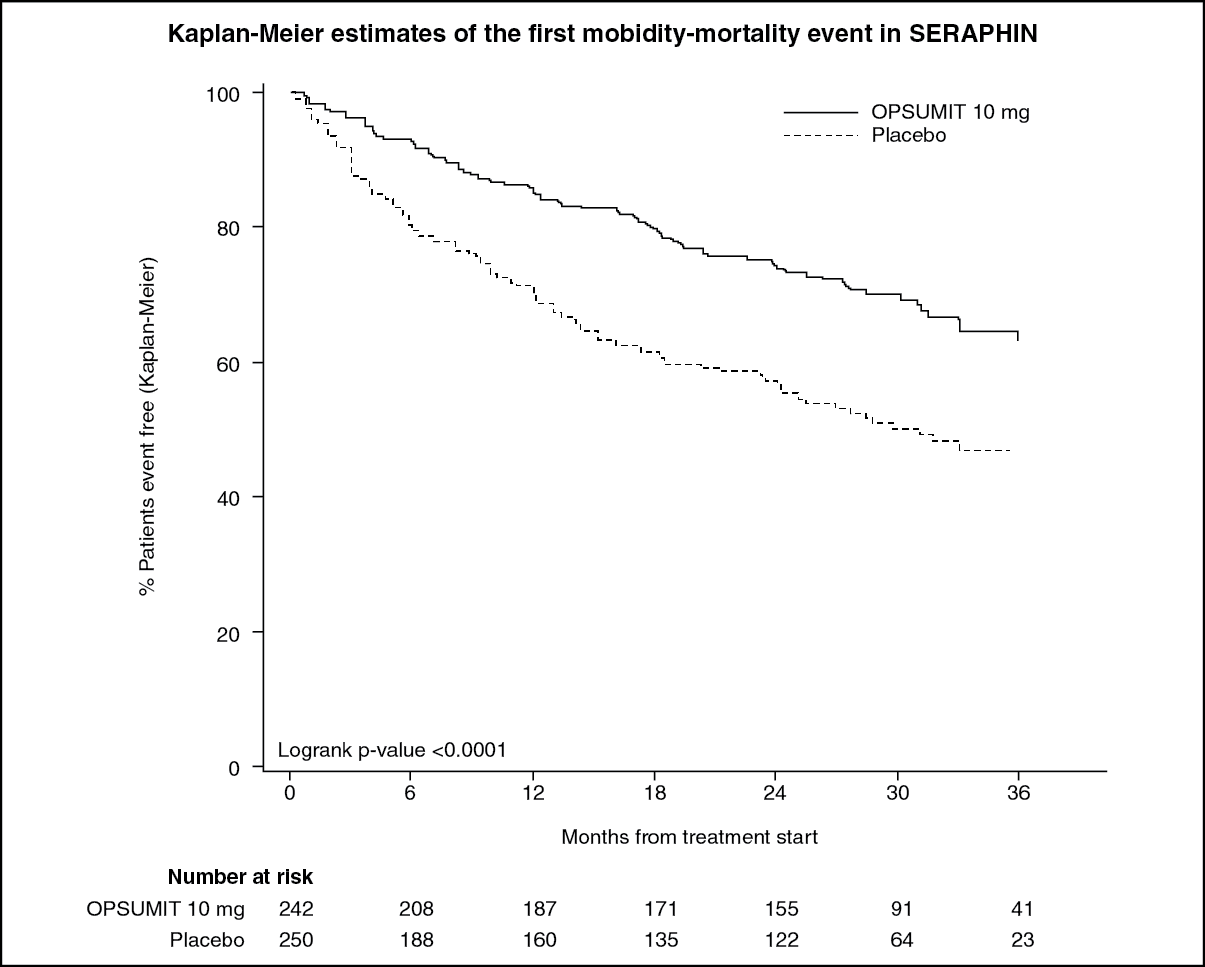
Clinical efficacy and safety: Efficacy in patients with pulmonary arterial hypertension: A multicenter, double-blind, placebo-controlled, parallel-group, event-driven, Phase 3 outcome study (AC-055-302/SERAPHIN) was conducted in 742 patients with symptomatic PAH, who were randomised to three treatment groups (placebo [N = 250], 3 mg [N = 250] or 10 mg [N = 242] of macitentan once daily), to assess the long-term effect on morbidity or mortality.
At baseline, the majority of enrolled patients (64%) were treated with a stable dose of specific therapy for PAH, either oral phosphodiesterase inhibitors (61%) and/or inhaled/oral prostanoids (6%).
The primary endpoint was the time to first occurrence of a morbidity or mortality event, up to the end of double-blind treatment, defined as death, or atrial septostomy, or lung transplantation, or initiation of intravenous (i.v.) or subcutaneous (s.c.) prostanoids, or other worsening of PAH. Other worsening of PAH was defined as the presence of all of the three following components: a sustained decrease in 6-minute walk distance (6MWD) of at least 15% from baseline; worsening of PAH symptoms (worsening of WHO FC or right heart failure); and need for new treatment for PAH. All events were confirmed by an independent adjudication committee, blinded to treatment allocation.
All patients were followed up to end-of-study (EOS) for vital status. EOS was declared when the predefined number of primary endpoint events was reached. In the period between end-of-treatment (EOT) and EOS, patients could receive open-label macitentan 10 mg or alternative PAH therapy. The overall median double-blind treatment duration was 115 weeks (up to a maximum of 188 weeks on macitentan).
The mean age of all patients was 46 years (range 12–85 years of age, including 20 patients below 18, 706 patients between 18–74 years, and 16 patients aged 75 and older) with the majority of subjects being Caucasian (55%) and female (77%). Approximately 52%, 46%, and 2% of patients were in WHO FC II, III, and IV, respectively.
Idiopathic or heritable PAH was the most common aetiology in the study population (57%), followed by PAH due to connective tissue disorders (31%), PAH associated with corrected simple congenital heart disease (8%), and PAH associated with other aetiologies (medicinal products and toxins [3%] and HIV [1%]).
Outcome endpoints: Treatment with macitentan 10 mg resulted in a 45% risk reduction (hazard ratio [HR] 0.55; 97.5% CI: 0.39 to 0.76; logrank p < 0.0001) of the composite morbidity-mortality endpoint up to EOT when compared to placebo [Figure 1 and Table 1]. The treatment effect was established early and was sustained.
Efficacy of macitentan 10 mg on the primary endpoint was consistent across subgroups of age, sex, ethnic origin, geographical region, aetiology, by monotherapy or in combination with another PAH therapy and by WHO FC (I/II and III/IV). (See Figure and Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The number of deaths of all causes up to EOS on macitentan 10 mg was 35 versus 44 on placebo (HR 0.77; 97.5% CI: 0.46 to 1.28).
The risk of PAH related death or hospitalisation for PAH up to EOT was reduced by 50% (HR 0.50; 97.5% CI: 0.34 to 0.75; logrank p < 0.0001) in patients receiving macitentan 10 mg (50 events) compared to placebo (84 events). At 36 months, 44.6% of patients on placebo and 29.4% of patients on macitentan 10 mg (Absolute Risk Reduction = 15.2%) had been hospitalised for PAH or died from a PAH-related cause.
Symptomatic endpoints: Exercise capacity was evaluated as a secondary endpoint. Treatment with macitentan 10 mg at Month 6 resulted in a placebo-corrected mean increase in 6MWD of 22 meters (97.5% CI: 3 to 41; p = 0.0078). Evaluation of 6MWD by functional class resulted in a placebo-corrected mean increase from baseline to Month 6 in FC III/IV patients of 37 meters (97.5% CI: 5 to 69) and in FC I/II of 12 meters (97.5% CI: −8 to 33). The increase in 6MWD achieved with macitentan was maintained for the duration of the study.
Treatment with macitentan 10 mg at Month 6 led to a 74% higher chance of WHO FC improvement relative to placebo (risk ratio 1.74; 97.5% CI: 1.10 to 2.74; p = 0.0063).
Macitentan 10 mg improved quality of life assessed by the SF-36 questionnaire.
Haemodynamic endpoints: Haemodynamic parameters were assessed in a subset of patients (placebo [N = 67], macitentan 10 mg [N = 57]) after 6 months of treatment. Patients treated with macitentan 10 mg achieved a median reduction of 36.5% (97.5% CI: 21.7 to 49.2%) in pulmonary vascular resistance and an increase of 0.58 L/min/m
2 (97.5% CI: 0.28 to 0.93 L/min/m
2) in cardiac index compared to placebo.
Long-term data in PAH: In long-term follow-up of 242 patients who were treated with macitentan 10 mg in the double-blind (DB) phase of the SERAPHIN study, 182 of which continued with macitentan in the open-label (OL) extension study (SERAPHIN OL) (DB/OL cohort), Kaplan-Meier estimates of survival at 1, 2, 5, 7 and 9 years were 95%, 89%, 73%, 63% and 53%, respectively. The median follow-up time was 5.9 years.
Pharmacokinetics: The pharmacokinetics of macitentan and its active metabolite have mainly been documented in healthy subjects. Exposure to macitentan in patients with PAH was approximately 1.2-fold greater than in healthy subjects. The exposure to the active metabolite in patients, which is approximately 5-fold less potent than macitentan, was approximately 1.3-fold higher than in healthy subjects. The pharmacokinetics of macitentan in PAH patients were not influenced by the severity of the disease.
After repeated administration, the pharmacokinetics of macitentan are dose-proportional up to and including 30 mg.
Absorption: Maximum plasma concentrations of macitentan are achieved about 8 hours after administration. Thereafter, plasma concentrations of macitentan and its active metabolite decrease slowly, with an apparent elimination half-life of approximately 16 hours and 48 hours, respectively.
In healthy subjects, the exposure to macitentan and its active metabolite is unchanged in the presence of food and, therefore, macitentan may be taken with or without food.
Distribution: Macitentan and its active metabolite are highly bound to plasma proteins (> 99%), primarily to albumin and to a lesser extent to alpha1-acid glycoprotein. Macitentan and its active metabolite ACT-132577 are well distributed into tissues as indicated by an apparent volume of distribution (Vss/F) of approximately 50 L and 40 L for macitentan and ACT-132577, respectively.
Biotransformation: Macitentan has four primary metabolic pathways. Oxidative depropylation of the sulfamide yields a pharmacologically active metabolite. This reaction is dependent on the cytochrome P450 system, mainly CYP3A4 (approximately 99%) with minor contributions of CYP2C8, CYP2C9 and CYP2C19. The active metabolite circulates in human plasma and may contribute to the pharmacological effect. Other metabolic pathways yield products without pharmacological activity. For these pathways, CYP2C plays a predominant role with minor contributions from CYP2C8, CYP2C19 and CYP3A4.
Elimination: Macitentan is only excreted after extensive metabolism. The major excretion route is via urine, accounting for about 50% of the dose.
Special populations: There is no clinically relevant effect of age, sex or ethnic origin on the pharmacokinetics of macitentan and its active metabolite.
Renal impairment: Exposure to macitentan and its active metabolite was increased by 1.3- and 1.6-fold, respectively, in patients with severe renal impairment. This increase is not considered clinically relevant (see Dosage & Administration and Precautions).
Hepatic impairment: Exposure to macitentan was decreased by 21%, 34%, and 6% and, for the active metabolite by 20%, 25%, and 25% in subjects with mild, moderate or severe hepatic impairment, respectively. This decrease is not considered clinically relevant (see Dosage & Administration and Precautions).
Toxicology: Preclinical safety data: In dogs, macitentan decreased blood pressure at exposures similar to the therapeutic human exposure. Intimal thickening of coronary arteries was observed at 17-fold the human exposure after 4 to 39 weeks of treatment. Due to the species-specific sensitivity and the safety margin, this finding is considered not relevant for humans.
Increased liver weight and hepatocellular hypertrophy were observed in mice, rats and dogs after treatment with macitentan. These changes were largely reversible and considered non-adverse adaptations of the liver to increased metabolic demand.
Macitentan induced minimal to slight mucosal hyperplasia and inflammatory infiltration in the submucosa of the nasal cavity in the mouse carcinogenicity study at all doses. No nasal cavity findings were noted in the 3-month mouse toxicity study or in rat and dog studies.
Macitentan was not genotoxic in a standard battery of
in vitro and
in vivo assays. Macitentan was not phototoxic
in vivo after single dose at exposures of up to 24-fold the human exposure. Carcinogenicity studies of 2 years' duration did not reveal a carcinogenic potential at exposures 18-fold and 116-fold the human exposure in rats and mice, respectively.
Testicular tubular dilatation was observed in chronic toxicity studies with male rats and dogs with safety margins of 11.6 and 5.8, respectively. Tubular dilatation was fully reversible. After 2 years of treatment, testicular tubular atrophy was seen in rats at 4-fold the human exposure.
Hypospermatogenesis was observed in the life-long carcinogenicity study in rats and in the repeat-dose toxicity studies in dogs at exposures that provide safety margins of 9.7 in rats and 23 in dogs. The safety margins for fertility were 18 for male and 44 for female rats. No testicular findings were noted in mice after treatment up to 2 years.
Macitentan was teratogenic in rabbits and rats at all doses tested. In both species there were cardiovascular and mandibular arch fusion abnormalities.
Administration of macitentan to female rats from late pregnancy through lactation at maternal exposures 5-fold the human exposure, caused reduced pup survival and impairment of the reproductive capability of the offspring, which was exposed to macitentan during late intrauterine life and via the milk during the suckling period.
Treatment of juvenile rats from postnatal Day 4 to Day 114 caused reduced body weight gain leading to secondary effects on development (slight delay of descensus testis, reversible reduction of long-bone length, prolonged estrous cycle). Slightly increased pre- and post-implantation loss, decreased mean number of pups, and decreased testis and epididymis weights, were observed at exposures 7-fold the human exposure. Testicular tubular atrophy, and minimal effects on reproductive variables and sperm morphology were recorded at exposures 3.8-fold the human exposure.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image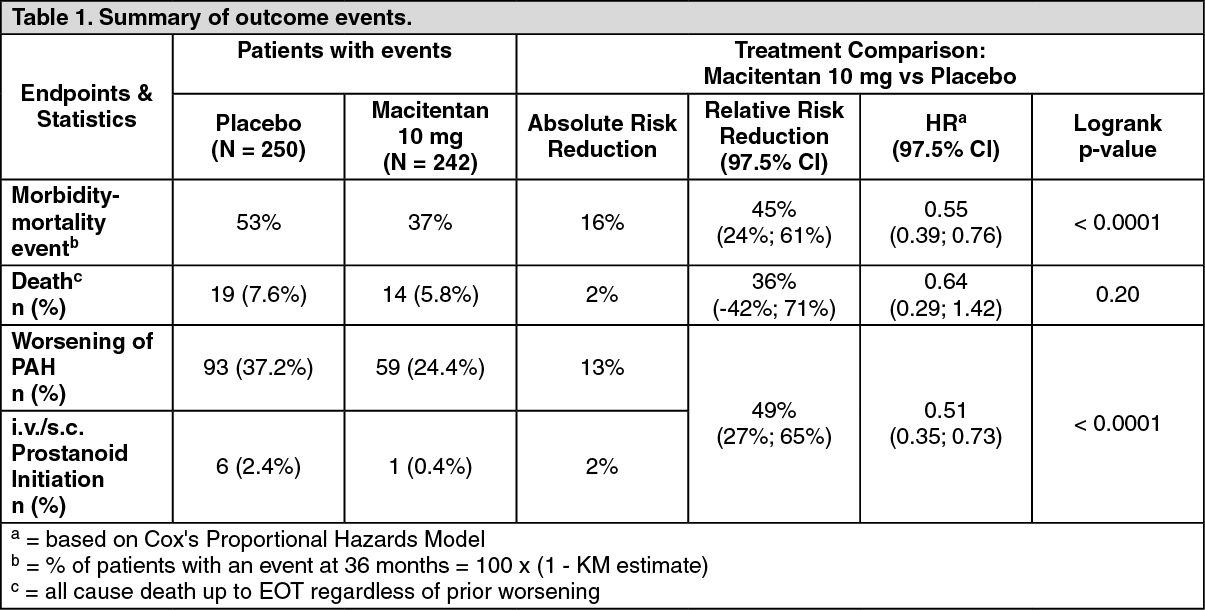 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
