


 Sign Out
Sign Out

In placebo-controlled atopic dermatitis clinical trials, for up to 16 weeks, the most commonly reported ADRs occurring in ≥ 2 % of patients treated with Olumiant monotherapy or in combination with topical corticosteroids were similar to those observed in rheumatoid arthritis, except for increased LDL cholesterol (13.2 %) and herpes simplex (6.1 %). In patients treated with baricitinib in the atopic dermatitis clinical trials, the frequency of herpes zoster was very rare.
Tabulated list of adverse reactions: Rheumatoid Arthritis: A total of 3,770 patients were treated with Olumiant in clinical studies in rheumatoid arthritis representing 10,127 patient-years of exposure. Of these, 2,960 rheumatoid arthritis patients were exposed to Olumiant for at least one year.
Seven placebo-controlled studies were integrated (1142 patients on 4 mg once daily and 1215 patients on placebo) to evaluate the safety of Olumiant in comparison to placebo for up to 16 weeks after treatment initiation.
Atopic Dermatitis: A total of 2,531 patients were treated with Olumiant in clinical studies in atopic dermatitis representing a total of 2,247 patient-years of exposure. Of these, 1,106 atopic dermatitis patients were exposed to Olumiant for at least one year.
Five placebo-controlled studies were integrated (489 patients on 4 mg once daily and 743 patients on placebo) to evaluate the safety of Olumiant in comparison to placebo for up to 16 weeks after treatment initiation.
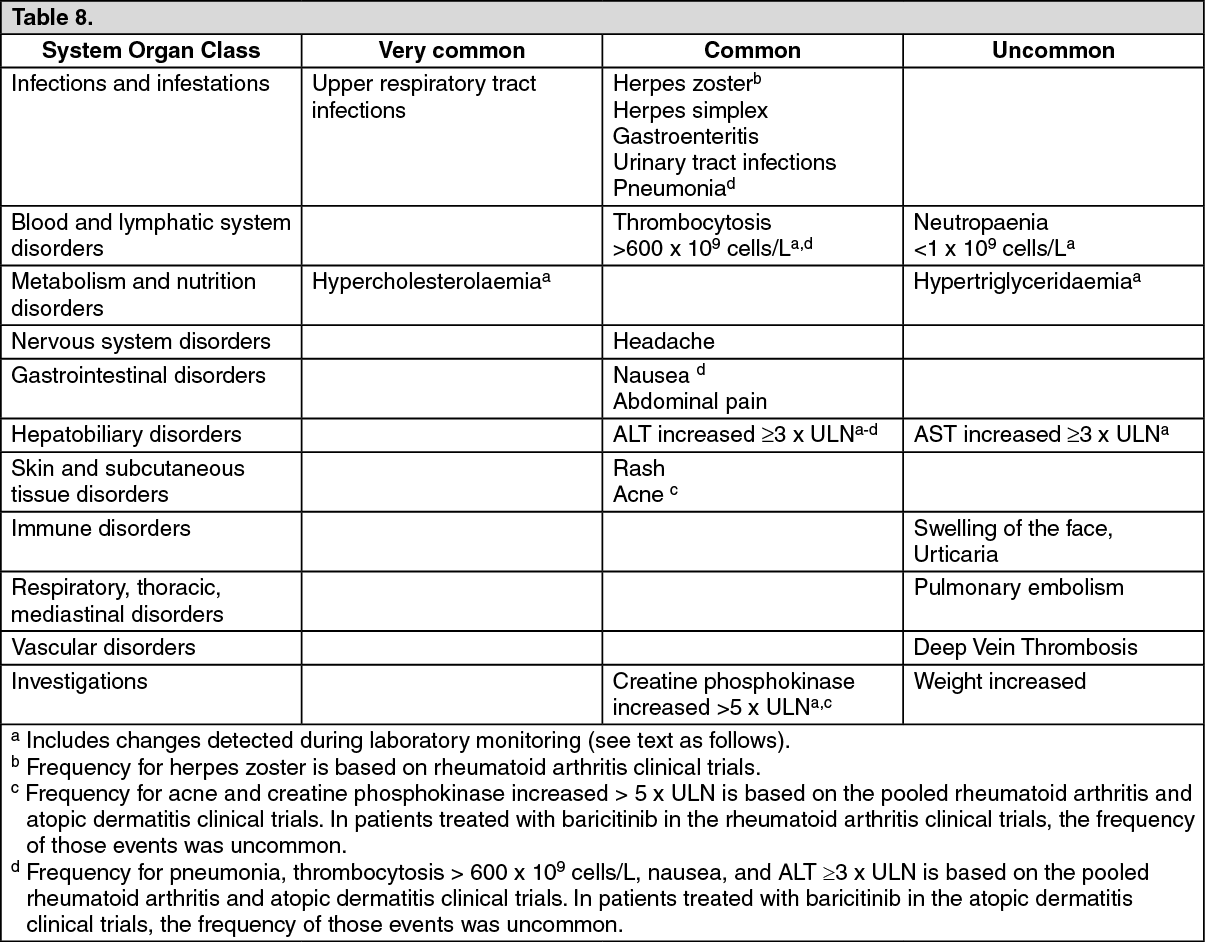
Frequency estimate: Very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000). The frequencies in Table 8 are based on integrated data across both rheumatoid arthritis and atopic dermatitis indications unless stated otherwise; where notable differences in frequency are observed in one indication alone, these are presented in the footnotes below the table. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Gastrointestinal disorders: In rheumatoid arthritis clinical studies, in treatment-naïve patients, through 52 weeks, the frequency of nausea was greater for the combination treatment of methotrexate and Olumiant (9.3 %) compared to methotrexate alone (6.2 %) or Olumiant alone (4.4 %). Nausea was most frequent during the first 2 weeks of treatment. In atopic dermatitis clinical studies, for up to 16 weeks, the frequency of nausea with Olumiant was 0.8 %.
In rheumatoid arthritis controlled studies, for up to 16 weeks, abdominal pain occurred in 2.1 % of patients treated with Olumiant 4 mg and 1.4 % of patients treated with placebo. The frequency of abdominal pain in atopic dermatitis clinical studies was similar. The cases were usually mild, transient, not associated with infectious or inflammatory gastrointestinal disorders, and did not lead to treatment interruption.
Infections: Rheumatoid Arthritis: In controlled studies, for up to 16 weeks, the incidence rate of all infections (rate of patients with ≥ 1 event per 100 patient-years of exposure) was 101 with Olumiant compared to 83 in the placebo group. Most infections were mild to moderate in severity. In studies which included both doses, infections were reported in 31.9 %, 28.8 % and 24.1 % of patients up to 16 weeks in the 4 mg, 2 mg and placebo groups, respectively. Reporting rates for Olumiant compared to placebo for the infection-related ADRs were: Upper respiratory tract infections (14.7 % vs. 11.7 %), urinary tract infections (3.4 % vs. 2.7 %), gastroenteritis (1.6 % vs. 0.8 %), herpes simplex (1.8 % vs. 0.7 %), and herpes zoster (1.4 % vs. 0.4 %). In treatment-naïve patients, for up to 52 weeks, the frequency of upper respiratory tract infections was greater for the combination treatment of methotrexate and Olumiant (26.0 %) compared to methotrexate alone (22.9 %) or Olumiant alone (22.0 %). The rate of serious infections with Olumiant (1.1 %) was similar to placebo (1.2 %). For Olumiant, the most common serious infections were herpes zoster, and cellulitis. The rate of serious infections remained stable during long-term exposure. The overall incidence rate of serious infections in the clinical trial programme was 3.2 per 100 patient-years.
Atopic Dermatitis: In controlled studies, for up to 16 weeks, the incidence rate of all infections (rate of patients with ≥ 1 event per 100 patient-years of exposure) was 155 with Olumiant 4 mg compared to 118 in the placebo group. Most infections were mild to moderate in severity. Infections were reported in 31.5 %, 29.8 % and 24.2 % of patients up to 16 weeks in the 4 mg, 2 mg and placebo groups, respectively. The percentage of patients reporting infection-related ADRs for Olumiant 4 mg compared to placebo were: Upper respiratory tract infections (17.5 % vs. 14.1 %), urinary tract infections (2.0 % vs. 0.8 %), gastroenteritis (1.2 % vs. 0.5 %), herpes simplex (6.1 % vs. 2.7 %), herpes zoster (0 % vs. 0.3 %) and pneumonia (0 % vs 0.1 %). In atopic dermatitis clinical studies, the frequency of infections was generally similar to those observed in rheumatoid arthritis patients except for pneumonia which was uncommon and herpes zoster which was very rare. There were less skin infections requiring antibiotic treatment with Olumiant 4 mg (3.4 %) than with placebo (4.4 %). The same percentage of patients with serious infections was observed with Olumiant 4 mg and placebo (0.6 %). The overall incidence rate of serious infections with baricitinib in the atopic dermatitis clinical trial programme was 2.1 per 100 patient-years.
Hepatic transaminase elevations: In rheumatoid arthritis controlled studies, for up to 16 weeks, alanine transaminase (ALT) and aspartate transaminase (AST) elevations ≥ 3 x upper limit of normal (ULN) were observed in 1.4 % and 0.8 % of patients treated with Olumiant, compared to 1.0 % and 0.8 % respectively of patients treated with placebo.
In treatment-naïve patients, the combination of Olumiant with potentially hepatotoxic medicinal products, such as methotrexate, resulted in increased frequency of these elevations. For up to 52 weeks, the frequency of ALT and AST elevations ≥ 3 x ULN were greater for the combination treatment of methotrexate and Olumiant (7.5 % and 3.8 %) compared to methotrexate alone (2.9 % and 0.5 %) or Olumiant alone (1.9 % and 1.3 %).
In atopic dermatitis controlled studies, for up to 16 weeks, ALT and AST elevations ≥ 3 x ULN were uncommonly observed in 0.2 % and 0.5 % of patients treated with Olumiant 4 mg, compared to 0.8 % and 0.8 % respectively of patients treated with placebo.
Across indications, most cases of hepatic transaminase elevations were asymptomatic and transient. The pattern and incidence of elevation in ALT/AST remained stable over time including in the long-term extension study.
Lipid elevations: In rheumatoid arthritis clinical studies, baricitinib treatment was associated with dose-dependent increases in lipid parameters including total cholesterol, triglycerides, LDL cholesterol, and HDL cholesterol. There was no change in the LDL/HDL ratio. Elevations were observed at 12 weeks and remained stable thereafter at a higher value than baseline including in the long-term extension study.
In studies which included both doses, a dose-relationship was observed with increased total cholesterol ≥ 5.17 mmol/L reported in 48.8 %, 34.7 % and 17.8 % of patients up to 16 weeks in the 4 mg, 2 mg and placebo groups, respectively.
Elevations in LDL cholesterol decreased to pre-treatment levels in response to statin therapy.
In atopic dermatitis clinical studies, baricitinib treatment was associated with increases in lipid parameters including total cholesterol, LDL cholesterol, and HDL cholesterol. Elevations were observed at 12 weeks and mean total and LDL cholesterol increased through week 52. There was no increase in the LDL/HDL ratio. No dose-relationships were observed in controlled studies, for up to 16 weeks for total cholesterol, LDL cholesterol, or HDL cholesterol. There was no increase in triglycerides levels.
In controlled studies, for up to 16 weeks, the following frequencies were observed for Olumiant 4 mg vs. placebo: Increased total cholesterol ≥ 5.17 mmol/L: Rheumatoid Arthritis: 49.1 % vs. 15.8 %, respectively; Atopic Dermatitis: 20.7 % vs. 10.0 %, respectively.
Increased LDL cholesterol ≥ 3.36 mmol/L: Rheumatoid Arthritis: 33.6 % vs. 10.3 %, respectively; Atopic Dermatitis: 13.2 % vs. 6.3 %, respectively.
Increased HDL cholesterol ≥ 1.55 mmol/L: Rheumatoid Arthritis: 42.7 % vs. 13.8 %, respectively; Atopic Dermatitis: 25.3 % vs. 14.7 %, respectively.
Increased triglycerides ≥ 5.65 mmol/L: Rheumatoid Arthritis: 0.4 % vs. 0.5 %, respectively; Atopic Dermatitis: 0.7 % vs. 0.8 %, respectively.
Creatine phosphokinase (CPK): In rheumatoid arthritis controlled studies, for up to 16 weeks, increases in CPK values were uncommon. Significant increases (> 5 x ULN) occurred in 0.8 % of patients treated with Olumiant and 0.3 % of patients treated with placebo. A dose relationship was observed with CPK elevations ≥ 5 x ULN of normal reported in 1.5 %, 0.8 % and 0.6 % of patients at 16 weeks in the 4 mg, 2 mg and placebo groups, respectively. In atopic dermatitis controlled studies, for up to 16 weeks, increases in CPK values were common and occurred in 3.3 %, 2.5 %, and 1.9 % of patients treated with Olumiant 4 mg, 2 mg, and placebo, respectively. Across indications, most cases were transient and did not require treatment discontinuation. In rheumatoid arthritis and atopic dermatitis clinical trials, there were no confirmed cases of rhabdomyolysis. Elevations of CPK were observed at 4 weeks and remained stable at a higher value than baseline thereafter including in the long-term extension study.
Neutropaenia: In rheumatoid arthritis and atopic dermatitis controlled studies, for up to 16 weeks, decreases in neutrophil counts below 1 x 109 cells/L occurred in 0.3 % of patients treated with Olumiant compared to 0 % of patients treated with placebo. There was no clear relationship between decreases in neutrophil counts and the occurrence of serious infections. However, in clinical studies, treatment was interrupted in response to ANC < 1 x 109 cells/L. The pattern and incidence of decreases in neutrophil counts remained stable at a lower value than baseline over time including in the long-term extension study.
Thrombocytosis: In rheumatoid arthritis controlled studies, for up to 16 weeks, increases in platelet counts above 600 x 109 cells/L occurred in 2.0 % of patients treated with Olumiant 4 mg and 1.1 % of patients treated with placebo. In atopic dermatitis controlled studies, for up to 16 weeks, increases in platelet counts above 600 x 109 cells/L occurred in 0.6 % of patients treated with Olumiant 4 mg and 0 % of patients treated with placebo. The frequency of thrombocytosis in atopic dermatitis studies was uncommon and lower than that observed in the rheumatoid arthritis patients.
No association was observed between increased platelet counts and adverse events of a thrombotic nature. The pattern and incidence of increases in platelet counts remained stable at a higher value than baseline over time including in the long-term extension study.
View ADR Monitoring Form