


 Sign Out
Sign Out

Medical examination: Prior to the initiation of Norcolut a complete medical history (including family history) should be taken and pregnancy must be ruled out. Blood pressure should be measured and a physical examination should be performed, guided by the contraindications, and warning. The medical examination should include measuring blood pressure, examination of the breasts, abdomen and internal and external genital organs, a cervical smear and appropriate laboratory tests. The frequency and nature of these assessments should be based upon relevant guidelines which should be adapted to the individual woman.
Ethinyloestradiol is an active metabolite of norethisterone, therefore the general warnings associated with the use of ethinyloestradiol should also be considered. If any of the conditions or risk factors mentioned as follows is present, the therapy with Norcolut should be discontinued immediately.
Venous thromboembolism: The use of any combined hormonal contraceptive (CHC) increases the risk of venous thromboembolism (VTE) compared with no use. Differences exist between CHCs in their risk of VTE depending on the type of progestogen they contain. Currently available data indicate that CHCs containing the progestogens levonorgestrel, norethisterone or norgestimate have the lowest risk of VTE.
Out of 10,000 women who are using a combined hormonal contraceptive that contains levonorgestrel, norethisterone, or norgestimate about 5-7 will develop a blood clot in a year.
Careful consideration should be given to the individual woman's current risk factors when prescribing a CHC, particularly those for VTE, and the difference in risk of VTE between products. CHCs are contraindicated if a woman has any serious risk factors that puts the woman at high risk of blood clots.
Patients with a history of VTE or known thrombophilic states have an increased risk of VTE. The treatment with steroid hormone may add to this risk.
A patient who develops symptoms suggestive of thromboembolic complications should stop treatment immediately. The need for treatment should be reassessed before continuing therapy. Generally recognised risk factors for venous thromboembolism (VTE) include: (see Table 3.)
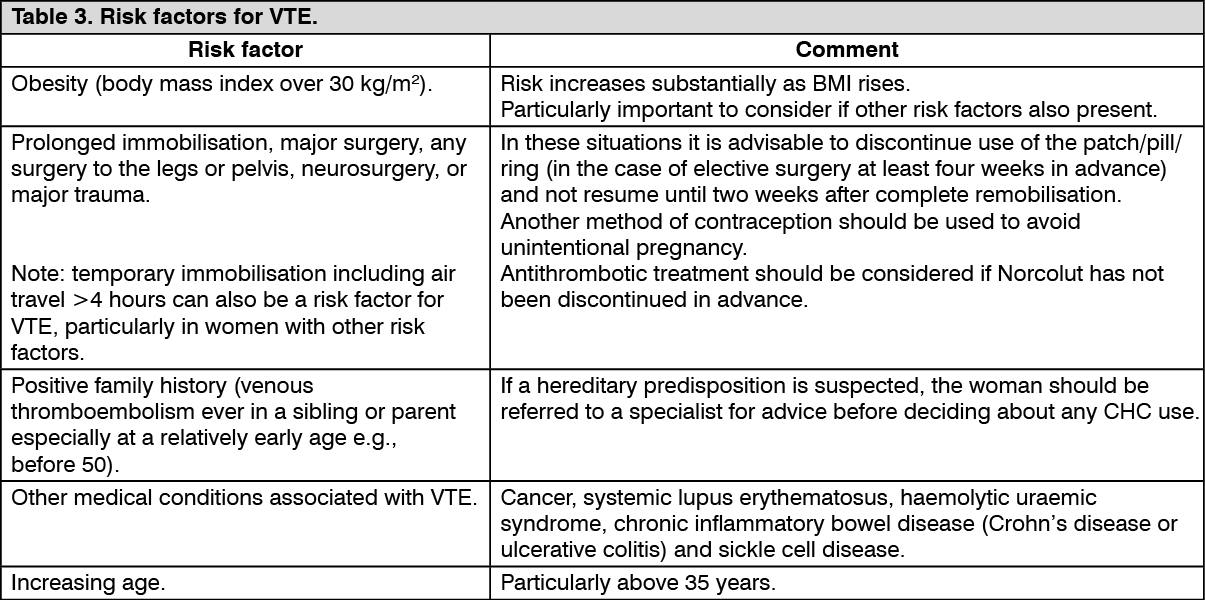 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThere is no consensus about the possible role of varicose veins and superficial thrombophlebitis in the onset or progression of venous thrombosis.
The increased risk of thromboembolism in pregnancy, and particularly the 6-week period of the puerperium, must be considered (for information, see Use in Pregnancy & Lactation).
Where a patient is already taking anticoagulants, the risk and benefits of progestogen therapy should be carefully considered.
Symptoms of VTE (deep vein thrombosis and pulmonary embolism): In the event of symptoms women should be advised to seek urgent medical attention and to inform the healthcare professional that she is taking a CHC.
Symptoms of deep vein thrombosis (DVT) can include: unilateral swelling of the leg and/or foot or along a vein in the leg; pain or tenderness in the leg which may be felt only when standing or walking; increased warmth in the affected leg; red or discoloured skin on the leg.
Symptoms of pulmonary embolism (PE) can include: sudden onset of unexplained shortness of breath or rapid breathing; sudden coughing which may be associated with haemoptysis; sharp chest pain; severe light headedness or dizziness; rapid or irregular heartbeat.
Some of these symptoms (e.g., "shortness of breath", "coughing") are non-specific and might be misinterpreted as more common or less severe events (e.g. respiratory tract infections).
Other signs of vascular occlusion can include: sudden pain, swelling and slight blue discoloration of an extremity.
If the occlusion occurs in the eye symptoms can range from painless blurring of vision which can progress to loss of vision. Sometimes loss of vision can occur almost immediately.
Arterial thromboembolic events: Risk factors for ATE: The risk of arterial thromboembolic complications or of a cerebrovascular accident in CHC users increases in women with risk factors (see Table 4). Norcolut is contraindicated if a woman has one serious or multiple risk factors for ATE that puts the woman at high risk of arterial thrombosis (see Contraindications). If a woman has more than one risk factor, it is possible that the increase in risk is greater than the sum of the individual factors - in this case the total risk should be considered. If the balance of benefits and risks is considered to be negative a CHC should not be prescribed (see Contraindications). (See Table 4.)
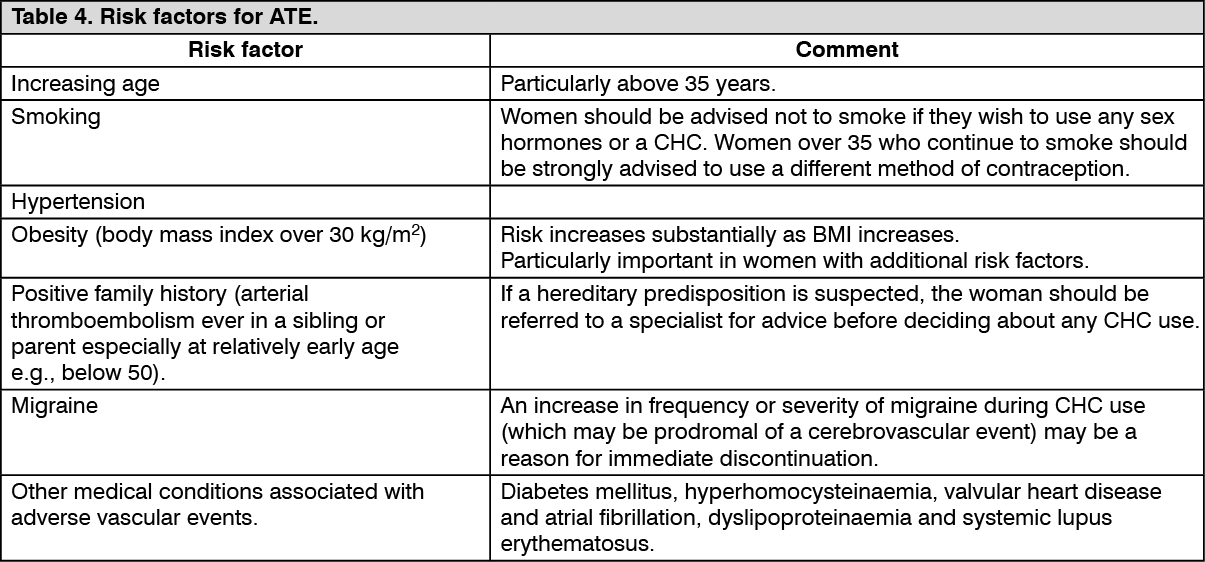 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSymptoms of ATE: In the event of symptoms women should be advised to seek urgent medical attention and to inform the healthcare professional that they are taking a CHC.
Symptoms of a cerebrovascular accident can include: sudden numbness or weakness of the face, arm or leg, especially on one side of the body; sudden trouble walking, dizziness, loss of balance or coordination; sudden confusion, trouble speaking or understanding; sudden trouble seeing in one or both eyes; sudden, severe or prolonged headache with no known cause; loss of consciousness or fainting with or without seizure.
Temporary symptoms suggest the event is a transient ischaemic attack (TIA).
Symptoms of myocardial infarction (MI) can include: pain, discomfort, pressure, heaviness, sensation of squeezing or fullness in the chest, arm, or below the breastbone; discomfort radiating to the back, jaw, throat, arm, stomach; feeling of being full, having indigestion or choking; sweating, nausea, vomiting or dizziness; extreme weakness, anxiety, or shortness of breath; rapid or irregular heartbeats.
Liver tumours: In rare cases, benign liver tumours, and even more rarely, malignant liver tumours have been reported in users of hormonal substances. In isolated cases, these tumours have led to life-threatening intra-abdominal haemorrhages. If severe upper abdominal complaints, liver enlargement or signs of intra-abdominal haemorrhage occur, a liver tumour should be included in the differential diagnosis and, if necessary, the preparation should be withdrawn.
Acute or chronic disturbances of liver function may necessitate the discontinuation of Norcolut use until markers of liver function return to normal.
Recurrence of cholestatic jaundice which occurred first during pregnancy or previous use of sex steroids necessitates the discontinuation of Norcolut.
Cervical cancer: The most important risk factor for cervical cancer is persistent HPV infection. Some epidemiological studies have indicated that long-term use of sex hormones may further contribute to this increased risk but there continues to be controversy about the extent to which this finding is attributable to confounding effects, e.g. sexual behaviour.
Breast cancer: Epidemiological studies reported that there is a slightly increased relative risk of having breast cancer diagnosed in women who are currently using products containing sex hormones. The excess risk gradually disappears during the course of the 10 years after cessation of the use of sex hormones. Because breast cancer is rare in women under 40 years of age, the excess number of breast cancer diagnoses in current and recent users of products containing sex hormones is small in relation to the overall risk of breast cancer. These studies do not provide evidence for causation. The breast cancers diagnosed in ever-users tend to be less advanced clinically than the cancers diagnosed in never-users.
Hyperlipidaemias: Oestrogen may slightly increase triglyceride levels, therefore women with hypertriglyceridemia, or a family history thereof, may be at increased risk of pancreatitis.
Increase in blood pressure: Although small increases in blood pressure have been reported in many women taking products containing sex hormones clinically relevant increases are rare. However, if a sustained clinically significant hypertension develops during the use of a Norcolut then it is prudent for the physician to withdraw the norethisterone and treat the hypertension.
However sex hormone-induced hypertension is not common, its recognition is important because hypertensive women using Norcolut appear to be at increased risk of MI and stroke relative to nonusers.
Depression: Progestins may cause or exacerbate depressive symptoms in certain subpopulations of women, including those with a history of premenstrual syndrome or mood disorders. Therefore, it is suggested that clinicians should often monitor the patients with depression and the drug should be discontinued if the depression recurs to a serious degree.
Carbohydrate metabolism: Although oestrogen and progestogen may have an effect on peripheral insulin resistance and glucose tolerance, there is no evidence for a need to alter the therapeutic regimen in diabetics using sex hormones. Parameters of carbohydrate metabolism should be examined carefully in all diabetics before and regularly during treatment.
Others: In women with hereditary angioedema exogenous oestrogens may induce or exacerbate symptoms of angioedema.
The use of exogenous hormone may be a contributing factors of chloasma especially in women with a history of chloasma gravidarum. Women with a tendency to chloasma should minimise exposure to the sun or ultraviolet radiation when taking Norcolut.
Oestrogens and progestogens may cause fluid retention. Special care should be taken when prescribing norethisterone in patients with conditions which might be aggravated by this factor: epilepsy, migraine, asthma, cardiac dysfunction, renal dysfunction.
There are inconsistent data in the scientific literature about the role of exogenous hormone in the development of inflammatory bowel disease (Crohn's disease, ulcerative colitis). However, cessation of Norcolut use should be considered in those women who remain symptomatic despite conventional drug therapy.
If menstrual bleeding should fail to follow a course of Norcolut, or if the patient wishes to postpone menstruation in special circumstances, the possibility of pregnancy must be excluded before a further course is given.
The following conditions have been reported to occur or deteriorate with both pregnancy and exogenous hormone use, but the evidence of an association with the use of sex hormones is inconclusive: jaundice and/or pruritus related to cholestasis; gallstones; porphyria; systemic lupus erythematosus; haemolytic uraemic syndrome; Sydenham's chorea; herpes gestationis; otosclerosis-related hearing loss.
ALT elevations: During clinical trials with patients treated for hepatitis C virus infections (HCV) with the medicinal products containing ombitasvir/paritaprevir/ritonavir and dasabuvir with or without ribavirin, transaminase (ALT) elevations higher than 5 times the upper limit of normal (ULN) occurred significantly more frequent in women using ethinyloestradiol-containing medications (see Contraindications and Interactions).
ALT elevations were also observed during concomitant use of combination glecaprevir/pibrentasvir and CHCs containing ethinyloestradiol in clinical trials (see Contraindications and Interactions).
Lactose: Norcolut tablet contains lactose. Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicine.