The information highlighted (if any) are the most recent updates for this brand.
One tablet contains 1.5 mg indapamide and 6.935 mg amlodipine besilate equivalent to 5 mg amlodipine.
One tablet contains 1.5 mg indapamide and 13.87 mg amlodipine besilate equivalent to 10 mg amlodipine.
Excipient with known effect: 104.5 mg lactose monohydrate.
Excipients/Inactive Ingredients: Natrixam 1.5 mg / 5 mg modified-release tablets: Tablet core: Hypromellose (E464), Lactose monohydrate, Magnesium stearate (E572), Povidone (E1201), Anhydrous colloidal silica, Calcium hydrogen phosphate dihydrate, Microcrystalline cellulose (E460), Croscarmellose sodium (E468), Pregelatinized maize starch.
Tablet film-coating: Glycerol (E422), Hypromellose (E464), Macrogol 6000, Magnesium stearate (E572), Titanium dioxide (E171).
Natrixam 1.5 mg / 10 mg modified-release tablets: Tablet core: Hypromellose (E464), Lactose monohydrate, Magnesium stearate (E572), Povidone (E1201), Anhydrous colloidal silica, Calcium hydrogen phosphate dihydrate, Microcrystalline cellulose (E460), Croscarmellose sodium (E468), Pregelatinized maize starch.
Tablet film-coating: Glycerol (E422), Hypromellose (E464), Iron oxide red (E172), Macrogol 6000, Magnesium stearate (E572), Titanium dioxide (E171).
Pharmacotherapeutic group: calcium channel blockers and diuretics. ATC code: C08GA02.
Pharmacology: Pharmacodynamics: Mechanism of action: Indapamide is a sulfonamide derivative with an indole ring, pharmacologically related to thiazide diuretics, which acts by inhibiting the reabsorption of sodium in the cortical dilution segment. It increases the urinary excretion of sodium and chlorides and, to a lesser extent, the excretion of potassium and magnesium, thereby increasing urine output and having an antihypertensive action.
Amlodipine is a calcium ion influx inhibitor of the dihydropyridine group (slow channel blocker or calcium ion antagonist) and inhibits the transmembrane influx of calcium ions into cardiac and vascular smooth muscle.
The mechanism of the antihypertensive action of amlodipine is due to a direct relaxant effect on vascular smooth muscle.
Pharmacodynamic effects: Phase II and III studies using indapamide monotherapy have demonstrated an antihypertensive effect lasting 24 hours. This was present at doses where the diuretic effect was of mild intensity.
The antihypertensive activity of indapamide is related to an improvement in arterial compliance and a reduction in arteriolar and total peripheral resistance.
Indapamide reduces left ventricular hypertrophy.
Thiazide and related diuretics have a plateau therapeutic effect beyond a certain dose, while adverse effects continue to increase. The dose should not be increased if treatment is ineffective.
It has also been shown, in the short-, mid- and long-term in hypertensive patients, that indapamide: does not interfere with lipid metabolism: triglycerides, LDL-cholesterol and HDL-cholesterol; does not interfere with carbohydrate metabolism, even in diabetic hypertensive patients.
In patients with hypertension, once daily dosing of amlodipine provides clinically significant reductions of blood pressure in both the supine and standing positions throughout the 24 hour interval. Due to the slow onset of action, acute hypotension is not a feature of amlodipine administration.
Amlodipine has not been associated with any adverse metabolic effects or changes in plasma lipids and is suitable for use in patients with asthma, diabetes, and gout.
Clinical efficacy and safety: Natrixam has not been studied on morbidity and mortality.
In the case of amlodipine, a randomized double-blind morbidity-mortality study called the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) was performed to compare newer drug therapies: amlodipine 2.5-10 mg/d (calcium channel blocker) or lisinopril 10-40 mg/d (ACE-inhibitor) as first-line therapies to that of the thiazide-diuretic, chlorthalidone 12.5-25 mg/d in mild to moderate hypertension.
A total of 33,357 hypertensive patients aged 55 or older were randomized and followed for a mean of 4.9 years. The patients had at least one additional CHD risk factor, including: previous myocardial infarction or stroke (> 6 months prior to enrollment) or documentation of other atherosclerotic CVD (overall 51.5%), type 2 diabetes (36.1%), HDL-C < 35 mg/dL (11.6%), left ventricular hypertrophy diagnosed by electrocardiogram or echocardiography (20.9%), current cigarette smoking (21.9%).
The primary endpoint was a composite of fatal CHD or non-fatal myocardial infarction. There was no significant difference in the primary endpoint between amlodipine-based therapy and chlorthalidone-based therapy: RR 0.98 95% CI (0.90-1.07) p=0.65. Among secondary endpoints, the incidence of heart failure (component of a composite combined cardiovascular endpoint) was significantly higher in the amlodipine group as compared to the chlorthalidone group (10.2% vs. 7.7%, RR 1.38, 95% CI [1.25-1.52] p<0.001). However, there was no significant difference in all-cause mortality between amlodipine-based therapy and chlorthalidone-based therapy. RR 0.96 95% CI [0.89-1.02] p=0.20.
Paediatric population: No data are available with Natrixam in children.
Pharmacokinetics: The co-administration of indapamide and amlodipine does not change their pharmacokinetic properties by comparison to separate administration.
Indapamide: Indapamide 1.5 mg is supplied in a prolonged release dosage based on a matrix system in which the active substance is dispersed within a support which allows sustained release of indapamide.
Absorption: The fraction of indapamide released is rapidly and totally absorbed via the gastrointestinal digestive tract.
Eating slightly increases the rapidity of absorption but has no influence on the amount of the active substance absorbed.
Peak serum level following a single dose occurs about 12 hours after ingestion, repeated administration reduces the variation in serum levels between 2 doses. Intra-individual variability exists.
Distribution: Binding of indapamide to plasma proteins is 79%.
The plasma elimination half-life is 14 to 24 hours (mean 18 hours).
Steady state is achieved after 7 days.
Repeated administration does not lead to accumulation.
Elimination: Elimination is essentially urinary (70% of the dose) and faecal (22%) in the form of inactive metabolites.
High risk individuals: Pharmacokinetic parameters are unchanged in renal failure patients.
Amlodipine: Amlodipine is supplied in an immediate release dosage.
Absorption, distribution, plasma protein binding: After oral administration of therapeutic doses, amlodipine is well absorbed with peak blood levels between 6-12 hours post dose. Absolute bioavailability has been estimated to be between 64 and 80%. The volume of distribution is approximately 21 l/kg. In vitro studies have shown that approximately 97.5% of circulating amlodipine is bound to plasma proteins.
The bioavailability of amlodipine is not affected by food intake.
Biotransformation/elimination: The terminal plasma elimination half-life is about 35-50 hours and is consistent with once daily dosing. Amlodipine is extensively metabolised by the liver to inactive metabolites with 10% of the parent compound and 60% of metabolites excreted in the urine.
Use in hepatic impairment: Very limited clinical data are available regarding amlodipine administration in patients with hepatic impairment. Patients with hepatic insufficiency have decreased clearance of amlodipine resulting in a longer half-life and an increase in AUC of approximately 40-60%.
Use in older people: The time to reach peak plasma concentrations of amlodipine is similar in elderly and younger subjects. Amlodipine clearance tends to be decreased with resulting increases in AUC and elimination half-life in elderly patients. Increases in AUC and elimination half-life in patients with congestive heart failure were as expected for the patient age group studied.
Toxicology: Preclinical safety data: Natrixam has not been studied in non clinical studies.
Indapamide: The highest doses administered orally to different animal species (40 to 8000 times the therapeutic dose) have shown an exacerbation of the diuretic properties of indapamide. The major symptoms of poisoning during acute toxicity studies with indapamide administered intravenously or intraperitoneally were related to the pharmacological action of indapamide, i.e. bradypnoea and peripheral vasodilation.
Indapamide has been tested negative concerning mutagenic and carcinogenic properties.
Reproductive toxicity studies have not shown any embryotoxic or teratogenic effect in rat, mice and rabbit.
Fertility was not impaired either in male or female rats.
Amlodipine: Reproductive toxicology: Reproductive studies in rats and mice have shown delayed date of delivery, prolonged duration of labour and decreased pup survival at dosages approximately 50 times greater than the maximum recommended dosage for humans based on mg/kg.
Impairment of fertility: There was no effect on the fertility of rats treated with amlodipine (males for 64 days and females 14 days prior to mating) at doses up to 10 mg/kg/day (8 times* the maximum recommended human dose of 10 mg on a mg/m2 basis). In another rat study in which male rats were treated with amlodipine besilate for 30 days at a dose comparable with the human dose based on mg/kg, decreased plasma follicle-stimulating hormone and testosterone were found as well as decreases in sperm density and in the number of mature spermatids and Sertoli cells.
Carcinogenesis, mutagenesis: Rats and mice treated with amlodipine in the diet for two years, at concentrations calculated to provide daily dosage levels of 0.5, 1.25, and 2.5 mg/kg/day showed no evidence of carcinogenicity. The highest dose (for mice, similar to, and for rats twice* the maximum recommended clinical dose of 10 mg on a mg/m2 basis) was close to the maximum tolerated dose for mice but not for rats.
Mutagenicity studies revealed no drug related effects at either the gene or chromosome levels.
*Based on patient weight of 50 kg.
Natrixam is indicated as substitution therapy for treatment of essential hypertension in patients already controlled with indapamide and amlodipine given concurrently at the same dose level.
Posology: One tablet per day as single dose, preferably to be taken in the morning, to be swallowed whole with water and not chewed.
The fixed dose combination is not suitable for initiation therapy.
If a change of the posology is required, titration should be done with the individual components.
Special populations: Paediatric population: The safety and efficacy of Natrixam in children and adolescents have not been established.
No data are available.
Patients with renal impairment (see Contraindications and Precautions): In severe renal impairment (creatinine clearance below 30 ml/min), treatment is contraindicated.
In patients with mild to moderate renal impairment, no dose adjustment is needed.
Older people (see Precautions and Pharmacology: Pharmacokinetics under Actions): Older people can be treated with Natrixam according to renal function.
Patients with hepatic impairment (see Contraindications and Precautions): In severe hepatic impairment, treatment is contraindicated.
Dosage recommendations of amlodipine have not been established in patients with mild to moderate hepatic impairment; therefore dose selection should be cautious and should start at the lower end of the dosing range (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Method of administration: Oral administration.
There is no information on overdose with Natrixam in humans.
For indapamide: Symptoms: Indapamide has been found free of toxicity at up to 40 mg, i.e. 27 times the therapeutic dose.
Signs of acute poisoning take the form above all of water/electrolyte disturbances (hyponatraemia, hypokalaemia). Clinically, possibility of nausea, vomiting, hypotension, cramps, vertigo, drowsiness, confusion, polyuria or oliguria possibly to the point of anuria (by hypovolaemia).
Treatment: Initial measures involve the rapid elimination of the ingested substance(s) by gastric wash-out and/or administration of activated charcoal, followed by restoration of water/electrolyte balance to normal in a specialised centre.
For amlodipine: In humans experience with intentional overdose is limited.
Symptoms: Available data suggest that gross overdose could result in excessive peripheral vasodilatation and possibly reflex tachycardia. Marked and probably prolonged systemic hypotension up to and including shock with fatal outcome have been reported.
Non-cardiogenic pulmonary oedema has rarely been reported as a consequence of amlodipine overdose that may manifest with a delayed onset (24-48 hours post-ingestion) and require ventilatory support. Early resuscitative measures (including fluid overload) to maintain perfusion and cardiac output may be precipitating factors.
Treatment: Clinically significant hypotension due to amlodipine overdose calls for active cardiovascular support including frequent monitoring of cardiac and respiratory function, elevation of extremities and attention to circulating fluid volume and urine output.
A vasoconstrictor may be helpful in restoring vascular tone and blood pressure, provided that there is no contraindication to its use. Intravenous calcium gluconate may be beneficial in reversing the effects of calcium channel blockade.
Gastric lavage may be worthwhile in some cases. In healthy volunteers the use of charcoal up to 2 hours after administration of amlodipine 10 mg has been shown to reduce the absorption rate of amlodipine.
Since amlodipine is highly protein-bound, dialysis is not likely to be of benefit.
Hypersensitivity to the active substances, to other sulfonamides, to dihydropyridine derivatives or to any of the excipients listed in Description.
Severe renal failure (creatinine clearance below 30 ml/min).
Hepatic encephalopathy or severe impairment of liver function.
Hypokalaemia.
Severe hypotension.
Shock (including cardiogenic shock).
Obstruction of the outflow tract of the left ventricle (e.g., high grade aortic stenosis).
Haemodynamically unstable heart failure after acute myocardial infarction.
Special warnings: Hepatic encephalopathy: When liver function is impaired, thiazide-related diuretics may cause, particularly in case of electrolyte imbalance, hepatic encephalopathy which can progress to hepatic coma. Due to the presence of indapamide, administration of Natrixam must be stopped immediately if this occurs.
Photosensitivity: Cases of photosensitivity reactions have been reported with thiazides and thiazide-related diuretics (see Adverse Reactions). If photosensitivity reaction occurs during treatment, it is recommended to stop the treatment. If a re-administration of the diuretic is deemed necessary, it is recommended to protect exposed areas to the sun or to artificial UVA.
Precautions for use: Hypertensive crisis: The safety and efficacy of amlodipine in hypertensive crisis have not been established.
Water and electrolyte balance: Plasma sodium: This must be measured before starting treatment, then at regular intervals subsequently. The fall in plasma sodium may be asymptomatic initially and regular monitoring is therefore essential, and should be even more frequent in the elderly and cirrhotic patients (see Adverse Reactions and Overdosage).
Any diuretic treatment may cause hyponatraemia, sometimes with very serious consequences. Hyponatraemia with hypovolaemia may be responsible of dehydration and orthostatic hypotension. Concomitant loss of chloride ions may lead to secondary compensatory metabolic alkalosis: the incidence and degree of this effect are slight.
Plasma potassium: Potassium depletion with hypokalaemia is the major risk of thiazide and related diuretics. Hypokalaemia may cause muscle disorders. Cases of Rhabdomyolysis have been reported, mainly in the context of severe hypokalaemia. The risk of onset of hypokalaemia (< 3.4 mmol/l) must be prevented in certain high risk populations, i.e. the elderly, malnourished and/or polymedicated, cirrhotic patients with oedema and ascites, coronary artery disease and cardiac failure patients. In this situation, hypokalaemia increases the cardiac toxicity of digitalis preparations and the risks of arrhythmias.
Individuals with a long QT interval are also at risk, whether the origin is congenital or iatrogenic. Hypokalaemia, as well as bradycardia, is then a predisposing factor to the onset of severe arrhythmias, in particular, potentially fatal torsades de pointes.
More frequent monitoring of plasma potassium is required in all the situations indicated as previously mentioned. The first measurement of plasma potassium should be obtained during the first week following the start of treatment.
Detection of hypokalaemia requires its correction. Hypokalaemia found in association with low serum magnesium concentration can be refractory to treatment unless serum magnesium is corrected.
Plasma magnesium: Thiazides and related diuretics including indapamide have been shown to increase the urinary excretion of magnesium, which may result in hypomagnesaemia (see Interactions and Adverse Reactions).
Plasma calcium: Thiazide and related diuretics may decrease urinary calcium excretion and cause a slight and transitory rise in plasma calcium. Frank hypercalcaemia may be due to previously unrecognised hyperparathyroidism.
Treatment should be withdrawn before the investigation of parathyroid function.
Blood glucose: Due to the presence of indapamide, monitoring of blood glucose is important in diabetics, in particular in the presence of hypokalaemia.
Cardiac failure: Patients with heart failure should be treated with caution. In a long-term, placebo controlled study in patients with severe heart failure (NYHA class III and IV) the reported incidence of pulmonary oedema was higher in the amlodipine treated group than in the placebo group. Calcium channel blockers, including amlodipine, should be used with caution in patients with congestive heart failure, as they may increase the risk of future cardiovascular events and mortality.
Uric acid: Due to the presence of indapamide, tendency to gout attacks may be increased in hyperuricaemic patients.
Choroidal effusion, acute myopia and secondary angle-closure glaucoma: Sulfonamide or sulfonamide derivative drugs can cause an idiosyncratic reaction resulting in choroidal effusion with visual field defect, transient myopia and acute angle-closure glaucoma. Symptoms include acute onset of decreased visual acuity or ocular pain and typically occur within hours to weeks of drug initiation. Untreated acute angle-closure glaucoma can lead to permanent vision loss. The primary treatment is to discontinue drug intake as rapidly as possible. Prompt medical or surgical treatments may need to be considered if the intraocular pressure remains uncontrolled. Risk factors for developing acute angle-closure glaucoma may include a history of sulfonamide or penicillin allergy.
Athletes: Athletes should note that this product contains an active substance which may cause a positive reaction in doping tests.
Excipients: Natrixam should not be administered to patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption.
Level of sodium: Natrixam contains less than 1 mmol sodium (23 mg) per tablet, i.e. essentially 'sodium-free'.
Effects on ability to drive and use machines: Natrixam has minor or moderate influence on the ability to drive and use machines: Indapamide does not affect vigilance but different reactions in relation with the decrease in blood pressure may occur in individual cases, especially at the start of the treatment or when another antihypertensive agent is added.
As a result the ability to drive vehicles or to operate machinery may be impaired.
Amlodipine can have minor or moderate influence on the ability to drive and use machines. If patients taking amlodipine suffer from dizziness, headache, fatigue or nausea the ability to react may be impaired. Caution is recommended especially at the start of treatment.
Renal function: Thiazide and related diuretics are fully effective only when renal function is normal or only minimally impaired (plasma creatinine below levels of the order of 25 mg/l, i.e. 220 μmol/l in an adult). In the elderly, this plasma creatinine must be adjusted in relation to age, weight and gender.
Hypovolaemia, secondary to the loss of water and sodium induced by the diuretic at the start of treatment causes a reduction in glomerular filtration. This may lead to an increase in blood urea and plasma creatinine. This transitory functional renal insufficiency is of no consequence in individuals with normal renal function but may worsen preexisting renal insufficiency.
Amlodipine may be used in patients with renal failure at normal doses. Changes in amlodipine plasma concentrations are not correlated with degree of renal impairment. Amlodipine is not dialysable.
The effect of the combination Natrixam has not been tested in renal dysfunction. In renal impairment, Natrixam doses should respect those of the individual components taken individually.
Hepatic function: The half-life of amlodipine is prolonged and AUC values are higher in patients with impaired liver function; dosage recommendations have not been established. Amlodipine should therefore be initiated at the lower end of the dosing range and caution should be used, both on initial treatment and when increasing the dose.
The effect of the combination Natrixam has not been tested in hepatic dysfunction. Taking into account the effect of indapamide and amlodipine, Natrixam is contra-indicated in patients with severe hepatic impairment, and caution should be exercised in patients with mild to moderate hepatic impairment.
Use in the Elderly: Older patients can be treated with Natrixam according to renal function (see Dosage & Administration and Pharmacology: Pharmacokinetics under Actions).
Given the effects of the individual components in this combination product on pregnancy and lactation: Natrixam is not recommended during pregnancy.
Natrixam is not recommended during lactation.
Pregnancy: Linked to indapamide: There are no or limited amount of data (less than 300 pregnancy outcomes) from the use of indapamide in pregnant women. Prolonged exposure to thiazide during the third trimester of pregnancy can reduce maternal plasma volume as well as uteroplacental blood flow, which may cause a foeto-placental ischaemia and growth retardation. Moreover, rare cases of hypoglycemia and thrombocytopenia in neonates have been reported following exposure near term.
Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Linked to amlodipine: The safety of amlodipine in human pregnancy has not been established.
In animal studies, reproductive toxicity was observed at high doses (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Breastfeeding: Linked to indapamide: There is insufficient information on the excretion of indapamide/metabolites in human milk. Hypersensitivity to sulfonamide-derived medicines and hypokalaemia might occur. A risk to the newborns/infants cannot be excluded.
Indapamide is closely related to thiazide diuretics which have been associated, during breast-feeding, with a decrease or even suppression of milk lactation.
Linked to amlodipine: Amlodipine is excreted in human milk. The proportion of the maternal dose received by the infant has been estimated with an interquartile range of 3 - 7%, with a maximum of 15%. The effect of amlodipine on infants is unknown.
Fertility: Linked to indapamide: Reproductive toxicity studies showed no effect on fertility in female and male rats (see Pharmacology: Toxicology: Preclinical safety data under Actions). No effects on human fertility are anticipated.
Linked to amlodipine: Reversible biochemical changes in the head of spermatozoa have been reported in some patients treated by calcium channel blockers. Clinical data are insufficient regarding the potential effect of amlodipine on fertility. In one rat study, adverse reactions were found on male fertility (see Pharmacology: Toxicology: Preclinical safety data under Actions).
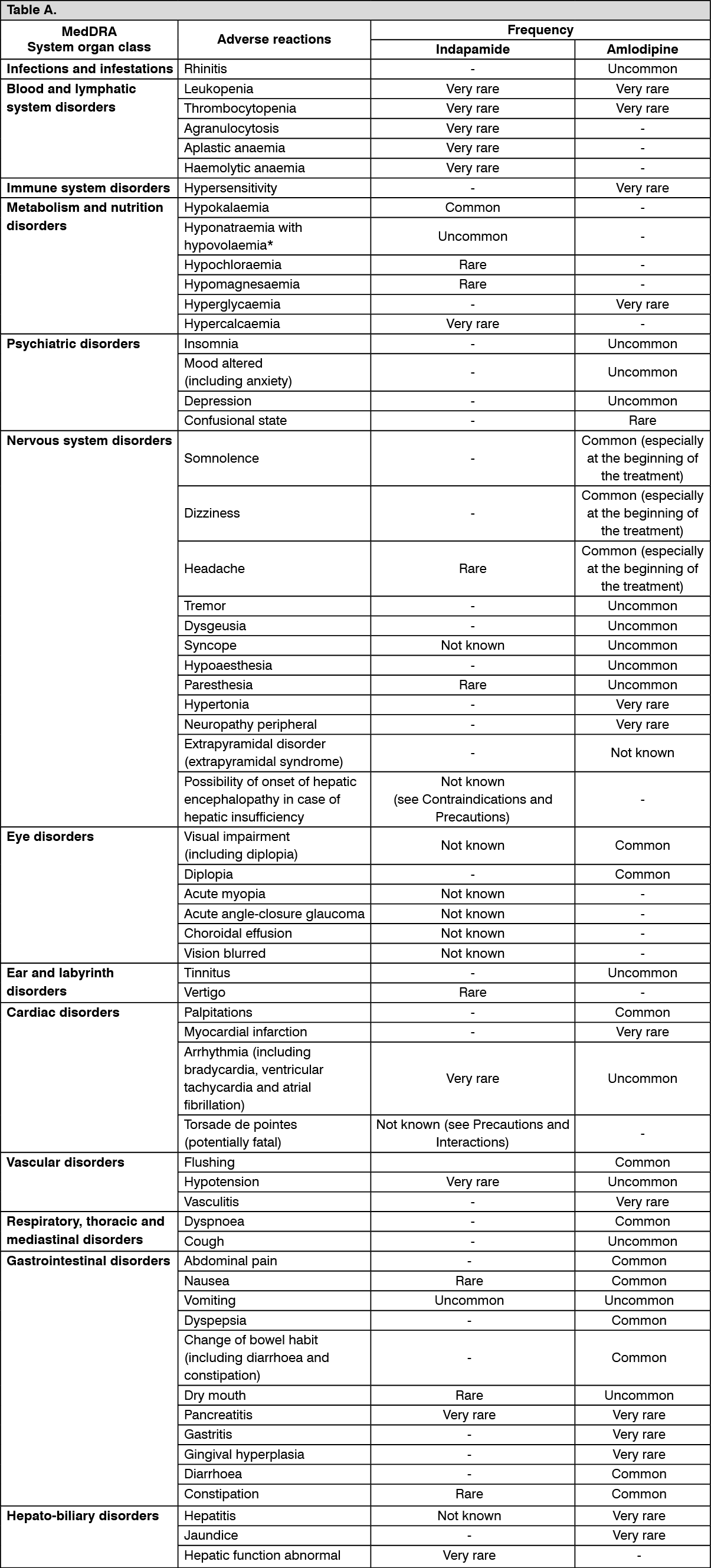
Summary of the safety profile: The most commonly reported adverse reactions with indapamide and amlodipine given separately are hypokalaemia, somnolence, dizziness, headache, visual impairment, diplopia, palpitations, flushing, dyspnoea, abdominal pain, nausea, dyspepsia, change of bowel habit, diarrhoea, constipation, rash maculo-papular, ankle swelling, muscle spasms, oedema, fatigue and asthenia.
Tabulated list of adverse reactions: The following adverse reactions have been observed and reported during treatment with indapamide and amlodipine with the following frequencies: Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to ≤1/100); rare (≥1/10,000 to ≤1/1,000); very rare (≤1/10,000); not known (cannot be estimated from the available data). (
See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Description of selected adverse reactions: During phase II and III studies comparing indapamide 1.5mg and 2.5mg, plasma potassium analysis showed a dose-dependent effect of indapamide: Indapamide 1.5mg: Plasma potassium <3.4 mmol/l was seen in 10 % of patients and < 3.2 mmol/l in 4 % of patients after 4 to 6 weeks treatment. After 12 weeks treatment, the mean fall in plasma potassium was 0.23 mmol/l.
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Description of selected adverse reactions: During phase II and III studies comparing indapamide 1.5mg and 2.5mg, plasma potassium analysis showed a dose-dependent effect of indapamide: Indapamide 1.5mg: Plasma potassium <3.4 mmol/l was seen in 10 % of patients and < 3.2 mmol/l in 4 % of patients after 4 to 6 weeks treatment. After 12 weeks treatment, the mean fall in plasma potassium was 0.23 mmol/l.
Indapamide 2.5 mg: Plasma potassium <3.4 mmol/l was seen in 25 % of patients and < 3.2 mmol/l in 10 % of patients after 4 to 6 weeks treatment. After 12 weeks treatment, the mean fall in plasma potassium was 0.41 mmol/l.
Linked to indapamide: Combinations that are not recommended: Lithium: Increased plasma lithium with signs of overdose, as with a salt-free diet (decreased urinary lithium excretion). However, if the use of diuretics is necessary, careful monitoring of plasma lithium and dose adjustment are required.
Combinations requiring precautions for use: Torsades de pointes-inducing medicines such as but not limited to: class Ia antiarrhythmic agents (e.g quinidine, hydroquinidine, disopyramide); class III antiarrhythmic agents (e.g amiodarone, sotalol, dofetilide, ibutilide, bretylium); some antipsychotics: phenothiazines (e.g chlorpromazine, cyamemazine, levomepromazine, thioridazine, trifluoperazine); benzamides (e.g amisulpride, sulpiride, sultopride, tiapride); butyrophenones (e.g droperidol, haloperidol); other antipsychotic (e.g pimozide); other substances (e.g bepridil, cisapride, diphemanil, erythromycin IV, halofantrine, mizolastine, pentamidine, sparfloxacin, moxifloxacin, vincamine IV, methadone, astemizole, terfenadine).
Increased risk of ventricular arrhythmias, particularly torsades de pointes (hypokalaemia is a risk factor).
Monitor for hypokalaemia and correct, if required, before introducing this combination. Clinical, plasma electrolytes and ECG monitoring.
Use substances which do not have the disadvantage of causing torsades de pointes in the presence of hypokalaemia.
N.S.A.I.Ds. (systemic route) including COX-2 selective inhibitors, high dose acetylsalicylic acid (≥ 3 g/day): Possible reduction in the antihypertensive effect of indapamide.
Risk of acute renal failure in dehydrated patients (decreased glomerular filtration). Hydrate the patient; monitor renal function at the start of treatment.
Angiotensin converting enzyme (A.C.E.) inhibitors: Risk of sudden hypotension and/or acute renal failure when treatment with an A.C.E. inhibitor is initiated in the presence of preexisting sodium depletion (particularly in patients with renal artery stenosis).
In hypertension, when prior diuretic treatment may have caused sodium depletion, it is necessary: either to stop the diuretic 3 days before starting treatment with the A.C.E. inhibitor, and restart a hypokalaemic diuretic if necessary; or give low initial doses of the A.C.E. inhibitor and increase the dose gradually.
In congestive heart failure, start with a very low dose of A.C.E. inhibitor, possibly after a reduction in the dose of the concomitant hypokalaemic diuretic.
In all cases, monitor renal function (plasma creatinine) during the first weeks of treatment with an A.C.E. inhibitor.
Other compounds causing hypokalaemia: amphotericin B (IV), gluco- and mineralo-corticoids (systemic route), tetracosactide, stimulant laxatives: Increased risk of hypokalaemia (additive effect).
Monitoring of plasma potassium and correction if required. Must be particularly borne in mind in case of concomitant digitalis treatment. Use non-stimulant laxatives.
Digitalis preparations: Hypokalaemia and/or hypomagnesaemia predispose to the toxic effects of digitalis.
Monitoring of plasma potassium, magnesium and ECG and, if necessary, adjust the treatment.
Baclofen: Increased antihypertensive effect.
Hydrate the patient; monitor renal function at the start of treatment.
Allopurinol: Concomitant treatment with indapamide may increase the incidence of hypersensitivity reactions to allopurinol.
Combinations to be taken into consideration: Potassium-sparing diuretics (amiloride, spironolactone, triamterene): Whilst rational combinations are useful in some patients, hypokalaemia or hyperkalaemia (particularly in patients with renal failure or diabetes) may still occur. Plasma potassium and ECG should be monitored and, if necessary, treatment reviewed.
Metformin: Increased risk of metformin induced lactic acidosis due to the possibility of functional renal failure associated with diuretics and more particularly with loop diuretics. Do not use metformin when plasma creatinine exceeds 15 mg/l (135 μmol/l) in men and 12 mg/l (110 μmol/l) in women.
Iodinated contrast media: In the presence of dehydration caused by diuretics, increased risk of acute renal failure, in particular when large doses of iodinated contrast media are used.
Rehydration before administration of the iodinated compound.
Imipramine-like antidepressants, neuroleptics: Antihypertensive effect and increased risk of orthostatic hypotension-(additive effect).
Calcium (salts): Risk of hypercalcaemia resulting from decreased urinary elimination of calcium.
Ciclosporin, tacrolimus: Risk of increased plasma creatinine without any change in circulating ciclosporin levels, even in the absence of water/sodium depletion.
Corticosteroids, tetracosactide (systemic route): Decreased antihypertensive effect (water/sodium retention due to corticosteroids).
Linked to amlodipine: Dantrolene (infusion): In animals, lethal ventricular fibrillation and cardiovascular collapse are observed in association with hyperkalaemia after administration of verapamil and intravenous dantrolene. Due to risk of hyperkalaemia, it is recommended that the co-administration of calcium channel blockers such as amlodipine be avoided in patients susceptible to malignant hyperthermia and in the management of malignant hyperthermia.
Administration of amlodipine with grapefruit or grapefruit juice is not recommended as bioavailability may be increased in some patients resulting in increased blood pressure lowering effects.
CYP3A4 inhibitors: Concomitant use of amlodipine with strong or moderate CYP3A4 inhibitors (protease inhibitors, azole antifungals, macrolides like erythromycin or clarithromycin, verapamil or diltiazem) may give rise to significant increase in amlodipine exposure. The clinical translation of these pharmacokinetic variations may be more pronounced in the elderly. Clinical monitoring and dose adjustment may thus be required.
There is an increased risk of hypotension in patients receiving clarithromycin with amlodipine. Close observation of patients is recommended when amlodipine is co administered with clarithromycin.
CYP3A4 inducers: Upon co-administration of known inducers of the CYP3A4, the plasma concentration of amlodipine may vary. Therefore, blood pressure should be monitored and dose regulation considered both during and after concomitant medication particularly with strong CYP3A4 inducers (e.g. rifampicin, Hypericum perforatum).
Effects of amlodipine on other medicinal products: The blood pressure lowering effects of amlodipine adds to the blood pressure-lowering effects of other medicinal products with antihypertensive properties.
In clinical interaction studies, amlodipine did not affect the pharmacokinetics of atorvastatin, digoxin, warfarin.
Tacrolimus: There is a risk of increased tacrolimus blood levels when co administered with amlodipine. In order to avoid toxicity of tacrolimus, administration of amlodipine in a patient treated with tacrolimus requires monitoring of tacrolimus blood levels and dose adjustment of tacrolimus when appropriate.
Mechanistic Target of Rapamycin (mTOR) Inhibitors: mTOR inhibitors such as sirolimus, temsirolimus, and everolimus are CYP3A substrates. Amlodipine is a weak CYP3A inhibitor. With concomitant use of mTOR inhibitors, amlodipine may increase exposure of mTOR inhibitors.
Ciclosporin: No drug interaction studies have been conducted with ciclosporin and amlodipine in healthy volunteers or other populations with the exception of renal transplant patients, where variable trough concentration increases (average 0% - 40%) of ciclosporin were observed. Consideration should be given to monitoring ciclosporin levels in renal transplant patients on amlodipine, and ciclosporin dose reductions should be made as necessary.
Simvastatin: Co-administration of multiple doses of 10 mg of amlodipine with 80 mg simvastatin resulted in a 77% increase in exposure to simvastatin compared to simvastatin alone. Limit the dose of simvastatin to 20 mg daily in patients on amlodipine.
Incompatibilities: Not applicable.
Special precautions for disposal: Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Store below 30°C.
Shelf life: 2 years.
C08GA02 - amlodipine and diuretics ; Belongs to the class of calcium-channel blockers in combination with diuretics. Used in the treatment of cardiovascular diseases.
Natrixam 1.5/10 mg MR-FC tab
30's
Natrixam 1.5/5 mg MR-FC tab
30's





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
