Pharmacotherapeutic group: Other alimentary tract and metabolism products, enzymes.
ATC code: A16AB07.
Pharmacology: Pharmacodynamics: Pompe disease: Pompe disease Pompe disease is a rare, progressive and fatal metabolic myopathy with an estimated global incidence of 1 in 40,000 births. Other names for Pompe disease include glycogen storage disease type II (GSD-II), acid maltase deficiency (AMD) and glycogenosis type II. Pompe disease belongs to the lysosomal storage disorders as it is caused by a deficiency of a naturally-occurring lysosomal hydrolase, acid α-glucosidase (GAA) that degrades lysosomal glycogen to glucose. Deficiency of this enzyme leads to glycogen accumulation in various tissues, particularly cardiac, respiratory and skeletal muscle, leading to the development of hypertrophic cardiomyopathy and progressive muscle weakness, including impairment of respiratory function. The clinical presentation of Pompe disease can be described as a spectrum of disease which ranges from a rapidly-progressing infantile-onset form (onset of symptoms of Pompe disease typically within the first year of life and a very short expected life-span) to a less rapidly-progressing late-onset form.
The infantile-onset form of Pompe disease is characterised by massive deposition of glycogen in the heart, and skeletal muscle always resulting in rapidly progressive cardiomyopathy, generalised muscle weakness and hypotonia. Motor development is often completely arrested, or if motor milestones are achieved, they are subsequently lost. Death typically occurs due to cardiac and/or respiratory failure before the age of one year.
In a retrospective natural history study in patients with infantile-onset Pompe disease (n=168), the median age at onset of symptoms was 2.0 months and the median age of death was 9.0 months. Kaplan-Meier survival rates at 12, 24 and 36 months of age were 26%, 9% and 7%, respectively.
A non-typical, more slowly progressive form of infantile-onset Pompe disease has been described which is characterised by a less severe cardiomyopathy and consequently a more prolonged survival.
The late-onset form of Pompe disease manifests during infancy, childhood, adolescence or even adulthood and is much less rapidly progressive than the infantile-onset form. Usually, it is characterised by the presence of sufficient residual GAA activity to preclude the development of cardiomyopathy, however some cardiac involvement has been reported in up to approximately 4% of patients with late-onset Pompe disease.
Patients with late-onset Pompe disease typically present with progressive myopathy, predominantly of the proximal muscles in the pelvic and shoulder girdles, and varying degrees of respiratory involvement, ultimately progressing to profound disability and/or the need for ventilatory support. The time course of disease progression is extremely variable and not predictable, with some patients experiencing a rapid deterioration in skeletal and respiratory muscle function leading to loss of ambulation and respiratory failure, others progressing less rapidly, and yet others presenting with a dissociation in the progression of skeletal and respiratory muscle involvement.
Mechanism of action: It is postulated that Myozyme will restore lysosomal GAA activity resulting in stabilisation or restoration of cardiac and skeletal muscle function (including respiratory muscles). Due to the blood-brain barrier effect and the enzyme's size, uptake of alglucosidase alfa in the central nervous system is unlikely.
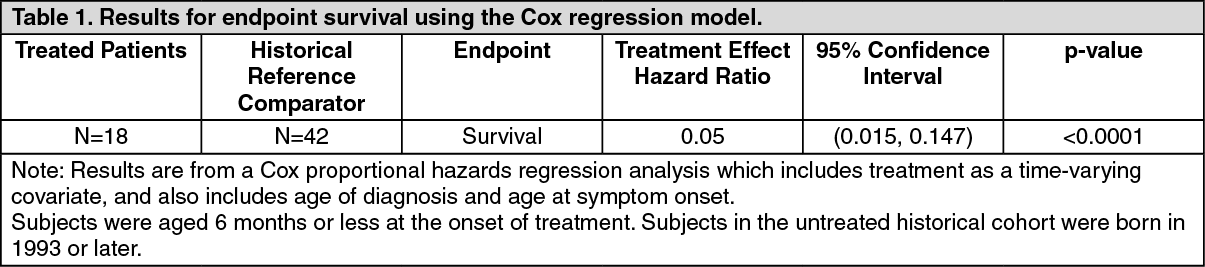
Clinical efficacy and safety: Infantile-onset Pompe disease; clinical trial in patients aged 6 months or less: The safety and efficacy of Myozyme was assessed in a pivotal, randomised, open-label, historically controlled clinical trial of 18 non-ventilated infantile-onset patients aged 6 months or less at the onset of treatment. The untreated historical cohort was matched to the pivotal study population and was derived from a retrospective natural history study (n = 42) in patients with infantile-onset Pompe disease. Patients were randomized to receive either 20 mg/kg or 40 mg/kg once every two weeks for a period of 52 weeks. After a minimum of 52 weeks, 16 of these 18 patients were enrolled in an extension study to receive continued treatment at the same dose for a total duration of up to three years (150 weeks).
The primary endpoint was the proportion of patients who were alive and free of invasive ventilator support. However, the invasive ventilator-free survival was not recorded in the untreated historical cohort and a comparison of this endpoint is not possible. After 52 weeks of treatment, all 18 patients treated with Myozyme were alive and 15 of these 18 patients were alive and free of invasive ventilatory support whereas 1 of 42 patients in the untreated historical cohort was alive at 18 months of age. Two patients died and did not enter into the extension study. After 104 weeks of treatment, all 16 patients who enrolled in the extension study were alive and 10 of these 16 patients were free of invasive ventilatory support. At the end of the study (with individual patient treatment durations ranging from 60 to 150 weeks; mean follow-up period of 119 weeks) 14 of 16 patients were alive and 9 of 16 patients were alive and free of invasive ventilatory support. One additional patient died after study end and another one after withdrawal from the study.
Comparison of survival curves from time of diagnosis versus the untreated historical cohort was made using a Cox proportional hazards regression analysis. Patients treated with Myozyme demonstrated prolonged survival as compared to survival in an untreated historical cohort (see Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Echocardiographic indices of cardiomyopathy improved as measured by a decrease in left ventricular mass (LVM). After 52 weeks of treatment, LVM decreased from baseline in all 14 patients with available data and was within normal limits in 3 of 14 patients. After the first year (64 up to 130 weeks) of treatment LVM further decreased in 8 patients. At 104 weeks of treatment LVM assessments were available for 8 patients, of which 5 decreased to within normal limits.
As measured by motor performance age-equivalent scores of the Alberta Infant Motor Scale (AIMS), seven of the 18 patients made motor development gains during the study and were walking independently by the last study assessment (with individual patient treatment durations ranging from 52 to 130 weeks; mean follow-up period of 94 weeks). An additional 4 patients made motor development gains during the study and were sitting independently by the last study assessment (with individual patient treatment durations ranging from 78 to 130 weeks; mean follow-up period of 110 weeks), although they did not have functional use of the legs. The remaining 7 patients made no clinically significant motor gains or were unable to sustain the motor gains made and had very limited motor movement by the last study assessment (with individual patient treatment durations ranging from 52 to 142 weeks; mean follow-up period of 103 weeks).
After 52 weeks of treatment 14 of 18 patients (77.8%) had maintained or improved weight-for-age percentiles (above the 3rd percentile), 14 of 15 patients (93.3%) were above the 3rd percentile for length and 12 of 15 patients (80.0%) were above the 3rd percentile for head circumference. In the second year of treatment, 15 out of 17 patients had further improved weight-for-age percentiles (with individual patient treatment durations ranging from 78 to 142 weeks; mean follow-up period of 111 weeks), 10 out of 16 patients had further improved length-for-age percentiles (with individual patient treatment durations ranging from 90 to 130 weeks; mean follow-up period of 113 weeks) and 11 out of 15 patients had further improved head circumference-for-age percentiles (with individual patient treatment durations ranging from 90 to 130 weeks; mean follow-up period of 110 weeks). At 104 weeks of treatment, all 13 patients with available data had maintained or improved weight-for-age percentiles (above the 3rd percentile), all 12 patients with available data were above the 3rd percentile for length and all 12 patients with available data were above the 3rd percentile for head circumference.
Analyses of efficacy did not reveal meaningful differences between the 2 dose groups with respect to survival, invasive ventilator-free survival, any ventilator-free survival, decrease in LVM, gains in growth parameters and acquisition of motor milestones. Based on these results the 20 mg/kg qow dose is recommended.
Infantile-onset Pompe disease; clinical trial in patients aged 6 months to 3.5 years: A second open-label clinical trial also assessed the safety and efficacy of Myozyme in 21 patients with predominantly a non-typical form of infantile-onset Pompe disease who ranged in age from 6 months to 3.5 years at initiation of treatment. Patients received 20 mg/kg Myozyme once every two weeks for 52 weeks except for 8 patients who received 40 mg/kg after at least 26 weeks of treatment. After 52 weeks all patients continued treatment for a total duration of more than 3 years (168 weeks with a median of 121 weeks).
The primary endpoint of the pivotal trial was the proportion of patients who were alive. After 52 weeks of treatment, 16 of 21 patients (76.2%) treated with Myozyme were alive. After 104 weeks of treatment, 14 of 21 patients (66.7%) were alive and 1 patient was alive but had discontinued from the study. These proportions were maintained up to the end of the study (with individual patient treatment durations ranging from 1 to 168 weeks; mean follow-up period of 109 weeks). In the untreated historical cohort 5 of 47 patients (10.6%) for whom data were available, were alive at age 30 months (2.5 years).
Survival in the treated patients was compared to survival in a similar historical cohort of untreated subjects using a Cox proportional hazards regression analysis (see Table 2).
Click on icon to see table/diagram/image
Additional efficacy data showed that of 16 patients who were free of invasive-ventilator support at baseline, 7 remained so after 104 weeks of treatment. The 9 remaining patients either died (5 patients) or became invasive-ventilator dependent (4 patients). All 5 patients who were receiving invasive ventilation at baseline continued to require ventilation throughout the study (4 patients survived beyond week 104 and one patient died).
After 52 weeks of treatment, LVM decreased from baseline in all 12 patients with available data and was within normal limits in 6 of 12 patients. After the first year (58 up to 168 weeks) of treatment LVM further decreased in 9 out of 12 patients with available data. At 104 weeks of treatment LVM assessments were available for 10 patients, of which 9 decreased to within normal limits.
After 52 weeks of treatment, 3 out of 8 patients with available data made gains in motor function over baseline as measured by raw scores and age-equivalent scores from baseline in the AIMS. Six of the 11 patients with available data continued to make motor development gains beyond Week 52 (with individual patient treatment durations ranging from 58 to 168 weeks; mean follow-up period of 121 weeks), including 3 patients ambulatory and 3 patients with only functional sitting skills by the last study visit. The remaining 5 patients showed no significant change in motor development beyond Week 52 (with individual patient treatment durations ranging from 104 to 168 weeks; mean follow-up period of 140 weeks), including 4 patients with no significant motor skills in any of the positions evaluated and 1 patient with only functional sitting skills by the last study visit.
The vast majority of patients with infantile-onset Pompe disease treated with Myozyme demonstrate improvement in cardiac function as well as stabilisation or improvements in growth parameters. However, motor and respiratory responses to treatment have been more variable.
Patients with infantile-onset Pompe disease who demonstrated motor gains, had greater preservation of motor function and lower glycogen content in the quadriceps muscle at baseline. It is noteworthy that a higher proportion of patients with better motor outcomes show stability or improvement in growth parameters (weight), while the large majority of patients, regardless of their motor outcomes or baseline features, show reversal of cardiomyopathy as measured by changes in LVM Z-score.
The totality of the data suggests that early diagnosis and treatment at an early stage of disease may be critical to achieve the best outcomes in these infantile onset patients.
IOPD Immune Tolerance Induction: Use of ITI and alglucosidase alfa has been evaluated in 1 clinical trial and a retrospective chart review of patients naïve to ERT at the initiation of treatment and 1 clinical trial of patients already receiving alglucosidase alfa at time of initiating ITI.
A retrospective chart review at Duke Center identified 21 CRIM-negative IOPD patients of which 19 patients were ERT naïve at the time of ITI initiation. Of the 21 patients, 16 survived through the end of this study, with a median time from ERT initiation to last assessment of 44.6 months (range: 5.7 to 105.47); 5 patients died due to respiratory failure and disease progression, all of whom were ERT-naive at the start of ERT+ITI treatment. Younger patients diagnosed and treated early and who received ITI concomitantly to ERT initiation had a trend towards better survival rate than patients treated with similar regimen at a later age. The study data demonstrated that prophylactic ITI prevents or reduces the occurrence of antibodies against alglucosidase alfa over time, which may maintain clinical benefit of ERT and improve survival in CRIM-negative IOPD patients.
Late-onset Pompe disease; pivotal clinical trial: The safety and efficacy of Myozyme was assessed in a randomized, double-blind, placebo-controlled study in 90 patients with late-onset Pompe disease who ranged in age from 10 to 70 years at initiation of treatment and were all naive to enzyme replacement therapy. Patients were randomized in a 2:1 ratio and received 20 mg/kg Myozyme (n=60) or placebo (n=30) once every two weeks for 78 weeks (18 months).
The co-primary efficacy outcome assessments were distance walked (meters) in 6 minutes (6-Minute Walk Test, 6MWT) and FVC (Forced Vital Capacity) % predicted in the sitting position. After 78 weeks, patients treated with Myozyme showed improvement in distance walked as measured by 6MWT and stabilization of pulmonary function as measured by FVC % predicted as compared to placebo-treated patients. The distance walked in 6 minutes increased by a median of 15.0 meters for Myozyme-treated patients and decreased by a median of 7.5 meters for placebo-treated patients, indicating a statistically significant Myozyme treatment effect compared to placebo (p=0.0283). The % predicted FVC changed by a median of 0.0 for Myozyme-treated patients and decreased by a median of 3% for placebo-treated patients, indicating a statistically significant treatment effect (p=0.0026). The results are shown in Table 3. (See Table 3.)
Click on icon to see table/diagram/image
Late-onset Pompe disease; other clinical trials and analyses: Three independent, open-label, single arm, investigator-initiated studies with Myozyme were conducted: One study in Italy enrolled 74 late-onset patients with up to 48 months follow up.
One study in Germany enrolled 38 late-onset patients with 36 months follow up.
One study in the Netherlands enrolled 69 late-onset patients with a median follow-up of 23 months.
These three studies with Myozyme (with a follow up of at least 3 years in two studies and a median of 23 months in the other study) suggested stabilisation or improvement of motor function and stabilisation of pulmonary function.
In the previously described study in 69 late-onset patients in the Netherlands, Myozyme showed an improvement in muscle strength. However, muscle function only improved in wheelchair independent patients and in those with less pronounced muscle weakness.
In two additional open-label clinical trials with Myozyme with a follow-up of 24 months, ten patients with severe late-onset Pompe disease (moderate to severe motor impairment and assisted ventilation) showed a variable response on measures of motor and respiratory functions, mostly in the form of a modest improvement (AGLU03105, AGLU04107).
An open-label clinical trial assessed the safety and efficacy of Myozyme in 5 patients with late-onset Pompe disease who ranged in age from 5 to 15 years at initiation of treatment (AGLU02804). Patients received 20 mg/kg Myozyme once every two weeks for 26 weeks. All patients were freely ambulatory and all but one patient did not require any form of ventilator support (1 patient required nocturnal non-invasive ventilation). Of the 3 patients with significant pulmonary involvement at screening/baseline (percentage predicted forced vital capacity in the sitting position ranging from 58-67%), two demonstrated clinically meaningful improvements in FVC (+11.5% and +16.0%) in the sitting position by Week 26. Evaluation of motor function gave disparate results.
Ten patients with advanced late-onset Pompe disease (i.e. wheelchair-bound for 10/10 and ventilator-dependent for 9/10) aged 9-54 years were treated in expanded access programs with alglucosidase alfa 20-40 mg/kg once every two weeks for various periods of time between 6 months and 2.5 years. The pulmonary benefits observed in patients included a clinically meaningful improvement in FVC of 35% in one patient, and significant reductions in the number of hours of ventilator support needed in 2 patients. Benefits of treatment on motor function including the regaining of lost motor skills were observed in some patients. Only one patient became wheelchair-free. In this group of patients a variable response has also been seen with respect to motor function.
Pompe Registry: Medical or healthcare professionals are encouraged to register patients who are diagnosed with Pompe disease at www.PompeRegistry.com. Patient data will be anonymously collected in this Registry. The objectives of the "Pompe Registry" are to enhance the understanding of Pompe disease and to monitor patients and their response to enzyme replacement therapy over time, with the ultimate goal of improving clinical outcomes for these patients.
Pharmacokinetics: Infantile-onset Pompe disease: In a pivotal trial including 18 patients, the pharmacokinetics of alglucosidase alfa were evaluated in 15 patients with infantile-onset Pompe disease (all less than 6 months of age at treatment-onset) who received doses of 20 mg/kg or 40 mg/kg alglucosidase alfa as an approximate 4 to 6.5-hour infusion, respectively.
Distribution and elimination: After the first and sixth infusion of Myozyme, mean maximum plasma concentrations (C
max) ranged from 178.2 to 263.7 μg/ml for the 20 mg/kg and 40 mg/kg dose groups respectively. The mean area under the plasma concentration-time curve (AUC
∞) ranged from 977.5 to 1,872.5 μg·hr/ml for the 20 mg/kg and 40 mg/kg dose groups. Mean plasma clearance (CL) was 21.4 ml/hr/kg and mean volume of distribution at steady state (V
ss) was 66.2 ml/kg for both dose groups with small between-subject variability of 15% and 11%, respectively. Mean plasma elimination half-life (t
½) was 2.75 hours for the two dose groups.
Linearity/non linearity: Pharmacokinetics were dose proportional and did not change over time.
The pharmacokinetics of alglucosidase alfa were also evaluated in a separate trial in 21 patients with infantile-onset Pompe disease (all aged between 6 months and 3.5 years at treatment-onset) who received doses of 20 mg/kg of alglucosidase alfa. In 12 patients with available data the AUC
∞ and C
max were approximately equivalent to those observed for the 20 mg/kg dose group in the pivotal trial. The t
½ of approximately 2 - 3 hours was also similar in this group of patients.
Late-onset Pompe disease: The pharmacokinetics of alglucosidase alfa were evaluated in a trial in 5 patients with late-onset Pompe disease aged 6-15 years who received 20 mg/kg alglucosidase alfa once every two weeks. There was no difference in the pharmacokinetic profile of alglucosidase alfa in these juvenile late-onset patients compared to infantile-onset patients.
The pharmacokinetics of alglucosidase alfa were studied in a population analysis of 32 late-onset Pompe disease patients from the randomized, double-blind, placebo-controlled study ranging in age from 21 to 70 years who received Myozyme 20 mg/kg once every two weeks. AUC
∞ and C
max were similar at week 0, 12 and 52 visits indicating alglucosidase alfa pharmacokinetics were not time-dependent (Table 4).
Distribution and elimination: (See Table 4.)
Click on icon to see table/diagram/image
There was no evidence that IgG antibodies to alglucosidase alfa affected pharmacokinetics. Higher mean clearance, lower mean AUC
∞, and lower mean C
max were observed in 5 patients who tested positive for inhibition of cellular uptake of enzyme. However, there was no apparent association between inhibition of uptake and the co-primary efficacy endpoints (see Precautions).
Toxicology: Preclinical Safety Data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, single and repeated dose toxicity. No significant adverse findings on embryofoetal development were observed in a mouse and a rabbit embryofoetal study and no significant adverse findings were observed in a mouse fertility and early embryonic development study. In the rabbit embryofoetal development study, following administration of Myozyme (10-40 mg/kg/day) with coadministration of diphenhydramine, a treatment-related increase in the incidence of abortions and early delivery was observed. This effect was partly attributable to maternal toxicity, as a significant decrease in feed consumption and body weight gain was observed.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image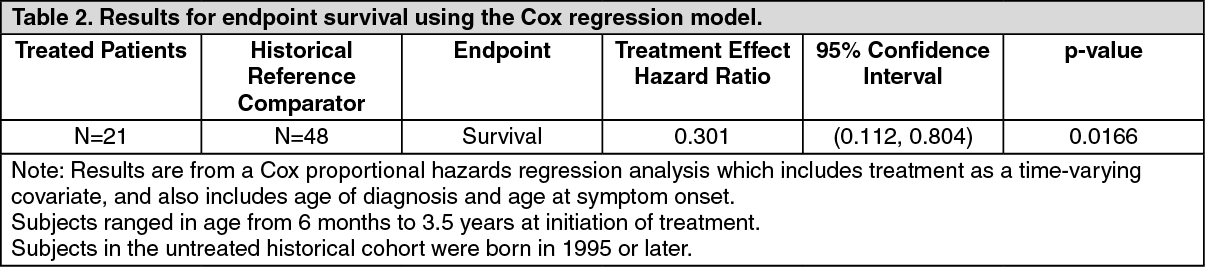 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
