General Dosing Guidelines: The recommended starting dose of bortezomib is 1.3 mg/m
2.
Bortezomib may be administered intravenously at a concentration of 1 mg/ml, or subcutaneously at a concentration of 2.5 mg/ml. When administered intravenously, Bortezomib is administered as a 3 to 5 second bolus intravenous injection. Bortezomib is for intravenous or subcutaneous use only. Bortezomib should not be administered by any other route. Because each route of administration has a different reconstituted concentration, caution should be used when calculating the volume to be administered.
BORTEZOMIB IS FOR INTRAVENOUS OR SUBCUTANEOUS USE ONLY. Intrathecal administration has resulted in death.
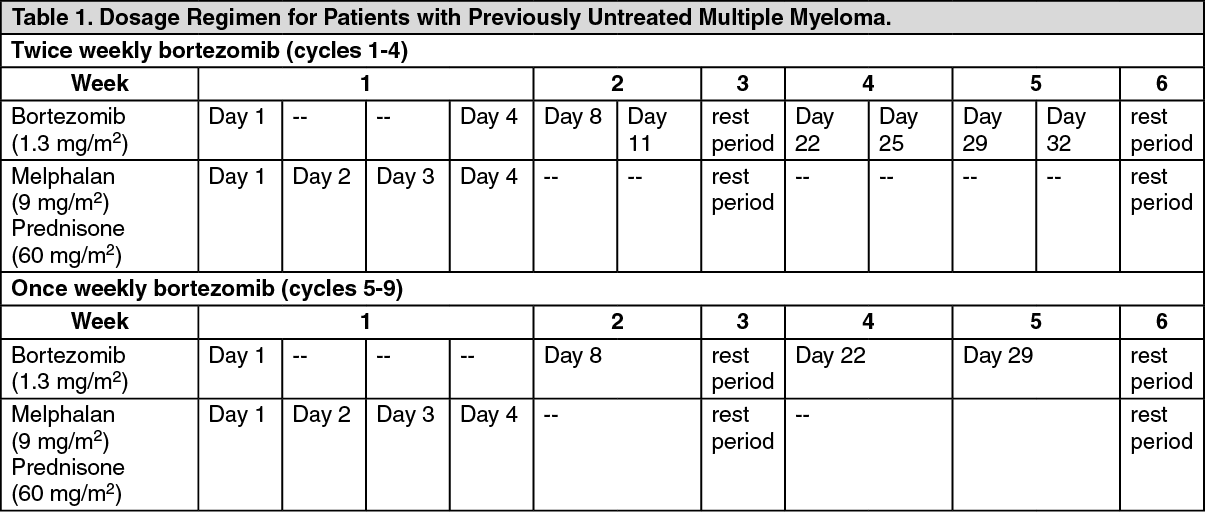
Dosage in Previously Untreated Multiple Myeloma: Bortezomib is administered in combination with oral melphalan and oral prednisone for nine 6-week treatment cycles as shown in Table 1.
In Cycles 1-4, bortezomib is administered twice weekly (days 1, 4, 8, 11, 22, 25, 29 and 32).
In Cycles 5-9, bortezomib is administered once weekly (days 1, 8, 22 and 29). At least 72 hours should elapse between consecutive doses of bortezomib. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Dose Modification Guidelines for Combination Therapy with bortezomib, Melphalan and Prednisone: Prior to initiating any cycle of therapy with bortezomib in combination with melphalan and prednisone: Platelet count should be ≥ 70 x 10
9/L and the ANC should be ≥ 1 x 10
9/L; nonhematological toxicities should have resolved to Grade 1 or baseline. (See Table 2.)
Click on icon to see table/diagram/image
For information concerning melphalan and prednisone, see manufacturer's prescribing information.
Dose modifications guidelines for peripheral neuropathy are provided.
Dosage and Dose Modifications for Relapsed Multiple Myeloma and Relapsed Mantle Cell Lymphoma: Bortezomib (1.3 mg/m
2/dose) is administered twice weekly for 2 weeks (Days 1, 4, 8, and 11) followed by a 10-day rest period (Days 12 - 21). For extended therapy of more than 8 cycles, bortezomib may be administered on the standard schedule or, for relapsed multiple myeloma, on a maintenance schedule of once weekly for 4 weeks (Days 1, 8, 15, and 22) followed by a 13-day rest period (Days 23 to 35). At least 72 hours should elapse between consecutive doses of bortezomib.
Bortezomib therapy should be withheld at the onset of any Grade 3 non hematological or Grade 4 hematological toxicities excluding neuropathy as discussed as follows. Once the symptoms of the toxicity have resolved, bortezomib therapy may be reinitiated at a 25% reduced dose (1.3 mg/m
2/dose reduced to 1.0 mg/m
2/dose; 1.0 mg/m
2/dose reduced to 0.7 mg/m
2/dose).
For dose modifications guidelines for peripheral neuropathy, see Dose Modifications for Peripheral Neuropathy as follows.
Dose Modifications for Peripheral Neuropathy: Starting bortezomib subcutaneously may be considered for patients with pre-existing or at high risk of peripheral neuropathy. Patients with pre-existing severe neuropathy should be treated with bortezomib only after careful risk-benefit assessment. Patients experiencing new or worsening peripheral neuropathy during bortezomib therapy may require a decrease in the dose and/or a less dose-intense schedule. For dose or schedule modification guidelines for patients who experience bortezomib-related neuropathic pain and/or peripheral neuropathy see Table 3. (See Table 3.)
Click on icon to see table/diagram/image
Special populations:
Elderly: There is no evidence to suggest that dose adjustments are necessary in patients over 65 years of age.
There are no studies on the use of bortezomib in elderly patients with previously untreated multiple myeloma who are eligible for high-dose chemotherapy with haematopoietic stem cell transplantation. Therefore no dose recommendations can be made in this population.
Previously untreated mantle cell lymphoma patients, who exposed to bortezomib were in the range 65-74 years and ≥ 75 years of age, respectively. In patients aged ≥ 75 years, both regimens, Bortezomib-R-CAP as well as R-CHOP, were less tolerated.
Hepatic impairment: Patients with mild hepatic impairment do not require a dose adjustment and should be treated per the recommended dose. Patients with moderate or severe hepatic impairment should be started on bortezomib at a reduced dose of 0.7 mg/m
2 per injection during the first treatment cycle, and a subsequent dose escalation to 1.0 mg/m
2 or further dose reduction to 0.5 mg/m
2 may be considered based on patient tolerability (see Table 4).
Click on icon to see table/diagram/image
Renal impairment: The pharmacokinetics of bortezomib are not influenced in patients with mild to moderate renal impairment (Creatinine Clearance [Cr
CL] > 20 ml/min/1.73 m
2); therefore, dose adjustments are not necessary for these patients. It is unknown if the pharmacokinetics of bortezomib are influenced in patients with severe renal impairment not undergoing dialysis (Cr
CL < 20 ml/min/1.73 m
2). Since dialysis may reduce bortezomib concentrations, bortezomib should be administered after the dialysis procedure.
Paediatric population: The safety and efficacy of bortezomib in children below 18 years of age have not been established.
Method of administration: Bortezomib 3.5 mg powder for solution for injection is available for intravenous or subcutaneous administration.
Bortezomib 1 mg powder for solution for injection is available for intravenous administration only.
Bortezomib should not be given by other routes. Intrathecal administration has resulted in death.
Intravenous injection: Bortezomib 3.5 mg reconstituted solution is administered as a 3-5 second bolus intravenous injection through a peripheral or central intravenous catheter followed by a flush with sodium chloride 9 mg/ml (0.9%) solution for injection. At least 72 hours should elapse between consecutive doses of bortezomib.
Subcutaneous injection: Bortezomib 3.5 mg reconstituted solution is administered subcutaneously through the thighs (right or left) or abdomen (right or left). The solution should be injected subcutaneously, at a 45-90° angle. Injection sites should be rotated for successive injections.
If local injection site reactions occur following bortezomib subcutaneous injection, either a less concentrated bortezomib solution (bortezomib 3.5 mg to be reconstituted to 1 mg/ml instead of 2.5 mg/ml) may be administered subcutaneously or a switch to intravenous injection is recommended.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image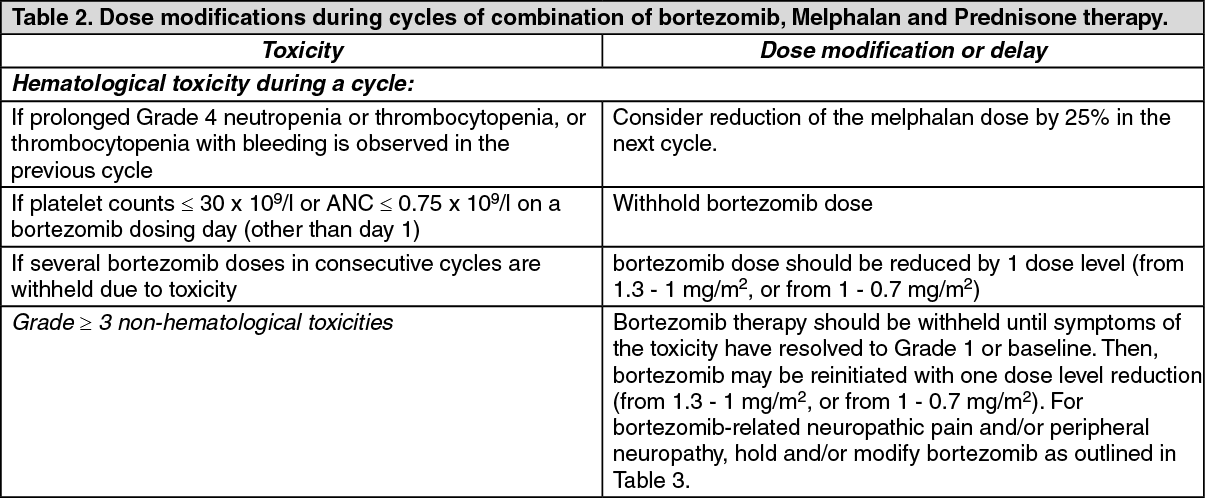 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image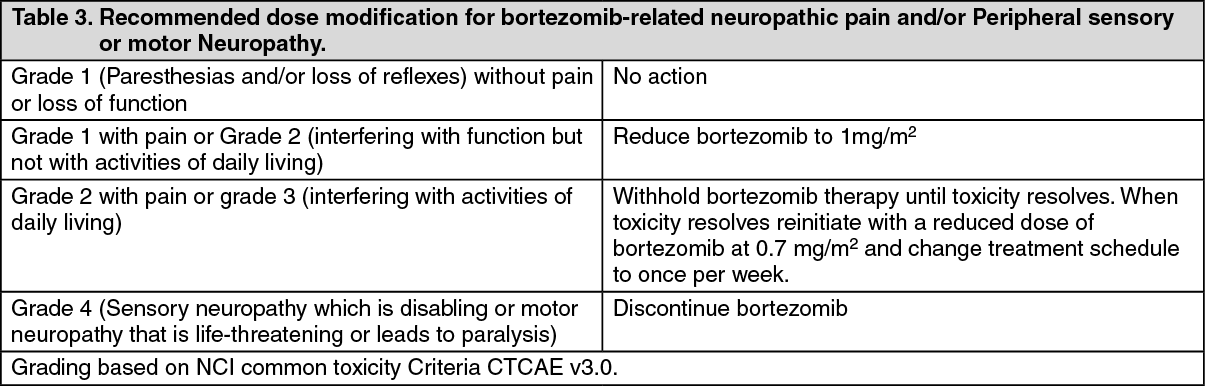 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image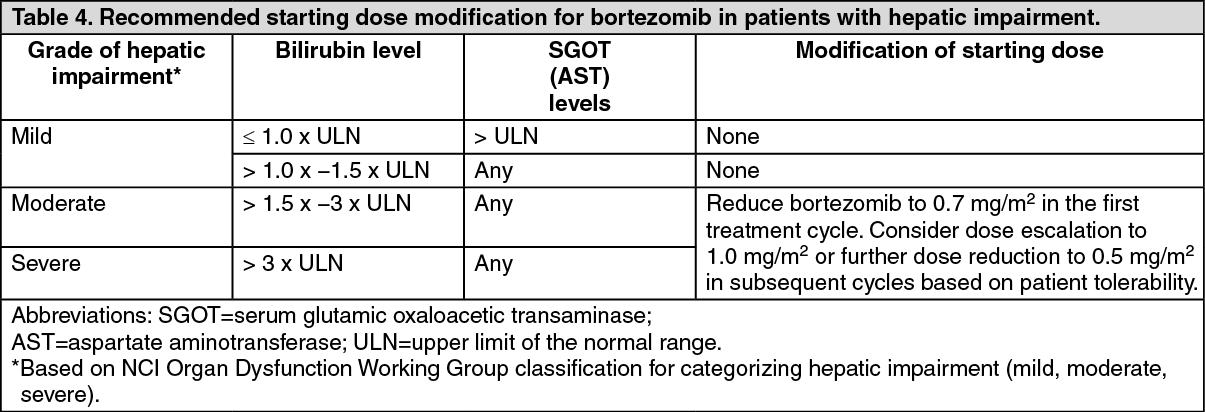 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image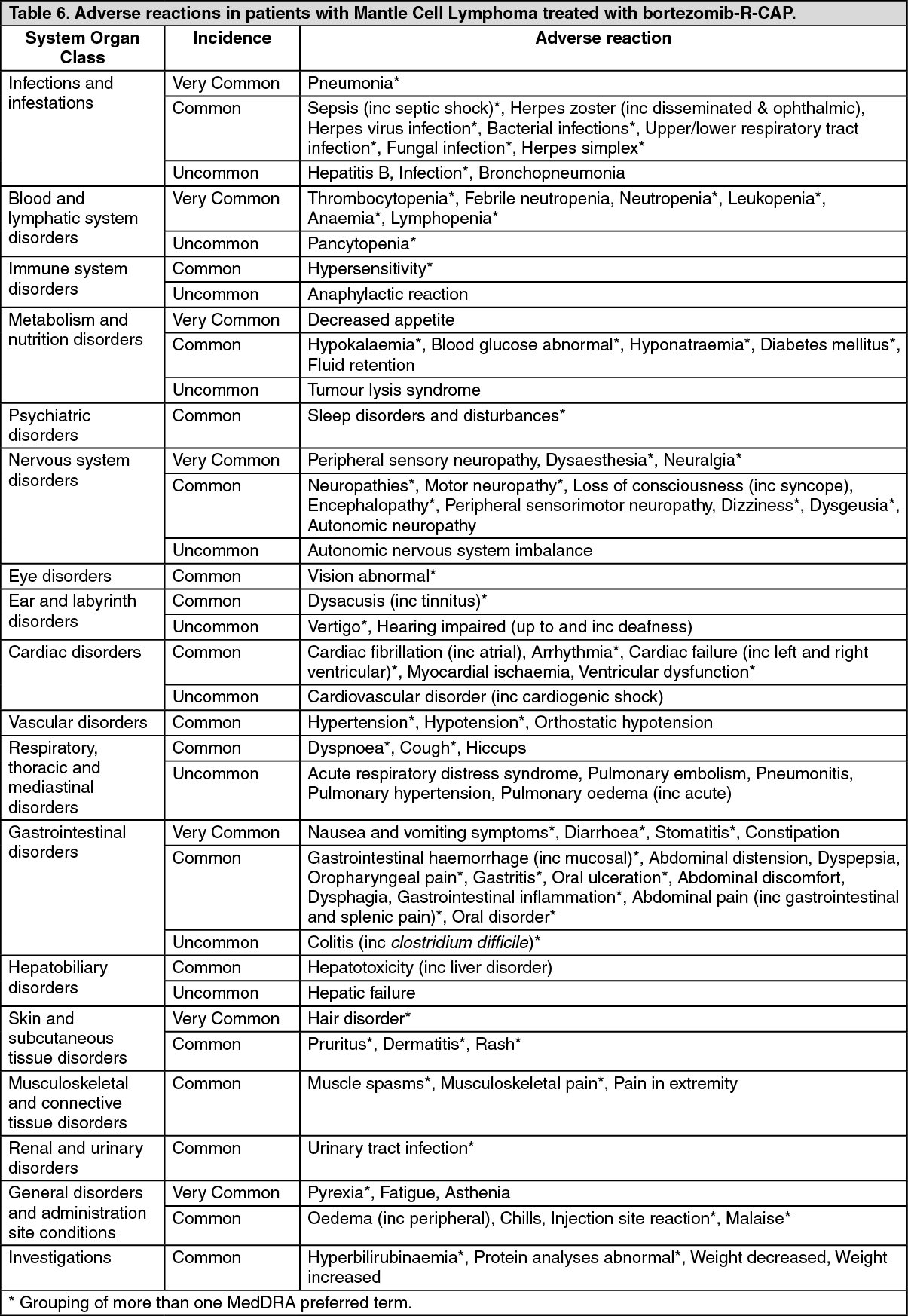 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
