


 Sign Out
Sign Out

For intravenous infusion the initially prepared solution may be diluted with 5% dextrose in water, isotonic saline solution, or 5% dextrose in isotonic saline solution. To avoid compatibility problems with other drugs Methylprednisolone powder for injection/infusion should be administered separately, only in the solutions mentioned.
Undesirable effects may be minimised by using the lowest effective dose for the minimum period.
Parenteral drug products should wherever possible be visually inspected for particulate matter and discoloration prior to administration.
Adults: Dosage should be varied according to the severity of the condition, initial dosage will vary from 10 to 500 mg. In the treatment of graft rejection reactions following transplantation, a dose of up to 1 gram/day may be required. Although doses and protocols have varied in studies using methylprednisolone sodium succinate in the treatment of graft rejection reactions, the published literature supports the use of doses of this level, with 500 mg to 1 g most commonly used for acute rejection.
Treatment at these doses should be limited to a 48-2 hour period until the patient's condition has stabilised, as prolonged high dose corticosteroid therapy can cause serious corticosteroid induced side effects.
Children: In the treatment of high dose indications, such as haematological, rheumatic, renal and dermatological conditions, a dosage of 30 mg/kg/day to a maximum of 1 g/day is recommended.
This dosage may be repeated for three pulses either daily or on alternate days. In the treatment of graft rejection reactions following transplantation, a dosage of 10 to 20 mg/kg/day for up to 3 days, to a maximum of 1 g/day, is recommended. In the treatment of status asthmaticus, a dosage of 1 to 4 mg/kg/day for 1-3 days is recommended.
Elderly patients: Methylprednisolone sodium succinate powder for injection/infusion is primarily used in acute short term conditions. There is no information to suggest that a change in dosage is warranted in the elderly. However, treatment of elderly patients should be planned bearing in mind the more serious consequences of the common side-effects of corticosteroids in old age and close clinical supervision is required (see Precautions).
Detailed recommendations for adult dosage are as follows: In anaphylactic reactions adrenaline or noradrenaline should be administered first for an immediate haemodynamic effect, followed by intravenous injection of methylprednisolone sodium succinate with other accepted procedures. There is evidence that corticosteroids through their prolonged haemodynamic effect are of value in preventing recurrent attacks of acute anaphylactic reactions.
In sensitivity reactions, Methylprednisolone sodium succinate is capable of providing relief within one half to two hours. In patients with status asthmaticus Methylprednisolone sodium succinate may be given at a dose of 40 mg intravenously, repeated as dictated by patient response. In some asthmatic patients it may be advantageous to administer by slow intravenous drip over a period of hours.
In graft rejection reactions following transplantation doses of up to 1 g per day have been used to suppress rejection crises, with doses of 500 mg to 1 g most commonly used for acute rejection. Treatment should be continued only until the patient's condition has stabilised usually not beyond 48-72 hours.
In cerebral oedema corticosteroids are used to reduce or prevent the cerebral oedema associated with brain tumours (primary or metastatic).
In patients with oedema due to tumour, tapering the dose of corticosteroid appears to be important in order to avoid a rebound increase in intracranial pressure. If brain swelling does occur as the dose is reduced (intracranial bleeding having been ruled out), restart larger and more frequent doses parenterally. Patients with certain malignancies may need to remain on oral corticosteroid therapy for months or even life. Similar or higher doses may be helpful to control oedema during radiation therapy.
The following are suggested dosage schedules for oedemas due to brain tumour: (See Table 1.)
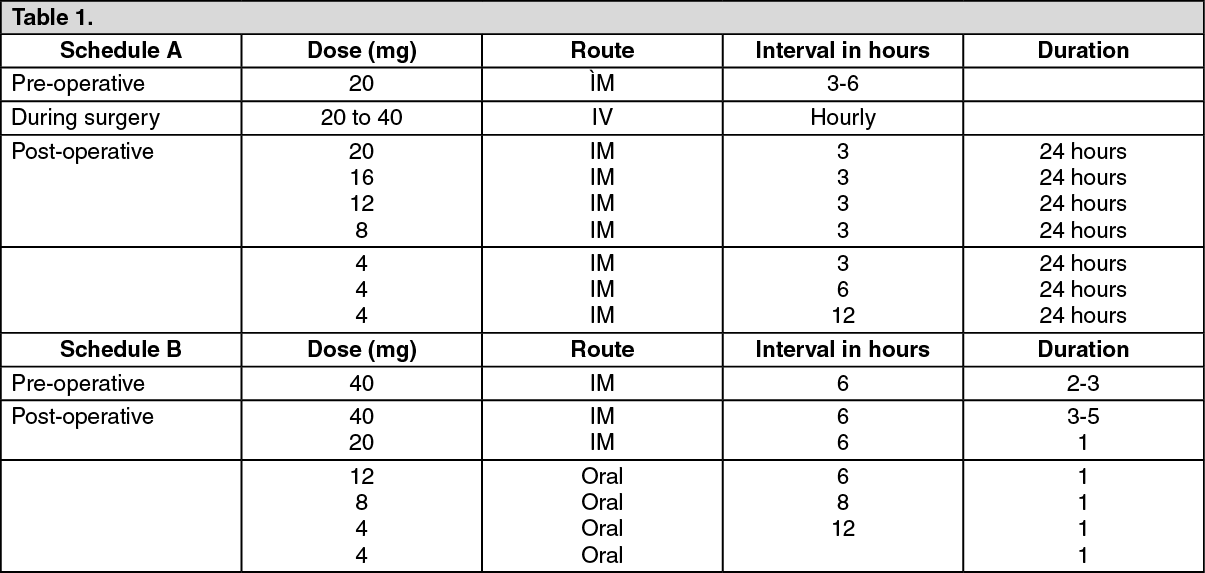 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAim to discontinue therapy after a total of 10 days.
In the treatment of acute exacerbations of multiple sclerosis in adults, the recommended dose is 1000 mg daily for 3 days.
Methylprednisolone powder for injection/infusion should be given as an intravenous infusion over at least 30 minutes.
In other indications, initial dosage will vary from 10 to 500 mg depending on the clinical problem being treated. Larger doses may be required for short term management of severe, acute conditions. The initial dose, up to 250 mg, should be given intravenously over a period of at least 5 minutes, doses exceeding 250 mg should be given intravenously over a period of at least 30 minutes.
Subsequent doses may be given intravenously or intramuscularly at intervals dictated by the patient's response and clinical condition. Corticosteroid therapy is an adjunct to, and not replacement for, conventional therapy.