Circulatory Disorders: Epidemiological studies have shown an association between the use of CHCs and an increased risk of arterial and venous thrombotic and thromboembolic diseases such as myocardial infarction, stroke, deep venous thrombosis, and pulmonary embolism. These events occur rarely.
The use of CHCs is associated with an increased risk of venous thromboembolism (VTE) manifesting as deep venous thrombosis and/or pulmonary embolism. The risk is highest during the first year a woman ever uses a CHC. The risk is also increased after initially starting a CHC or restarting the same or different CHC after a break in use of 4 weeks or more.
Some epidemiological studies have suggested that women using low-dose COCs with third generation progestogens, including desogestrel, have an increased risk of VTE compared with those using low-dose COCs with the progestogen levonorgestrel. These studies indicate an approximate 2-fold increase in risk, which would correspond to an additional 1-2 cases of VTE per 10 000 women years of use. However, data from other studies have not shown this 2-fold increase in risk.
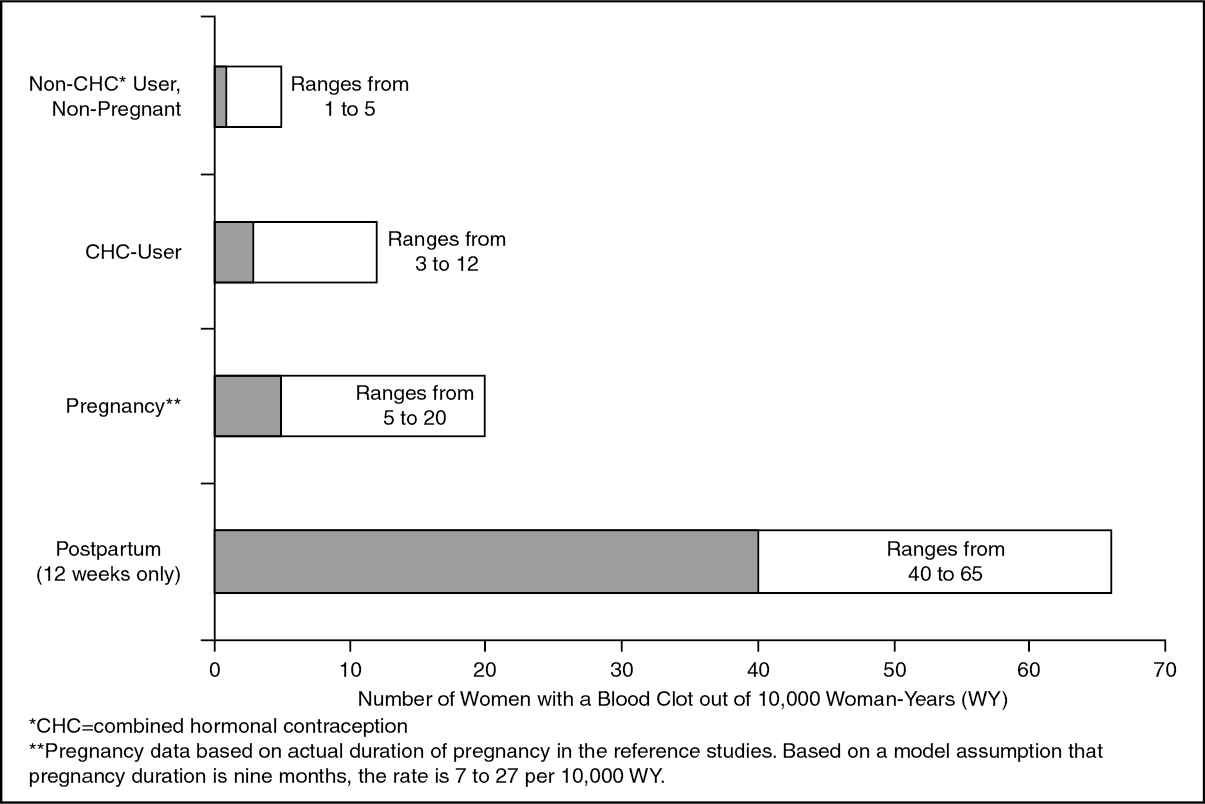
Overall, the incidence of VTE in users of low estrogen dose (< 0.05 mg ethinylestradiol) CHCs ranges from about 3 to 12 cases per 10 000 women years compared to 1 to 5 cases per 10 000 women years in non-CHC users. The incidence of VTE occurring during CHC use is less than the incidence associated with pregnancy (i.e. 5 to 20 cases per 10 000 women years). VTE is fatal in 1-2% of cases.
The figure as follows shows the risk of developing a VTE for women who are not pregnant and do not use CHCs, for women who use CHCs, for pregnant women, and for women in the postpartum period. To put risk of developing a VTE into perspective: If 10,000 women who are not pregnant and do not use CHCs are followed for one year, between 1 and 5 of these women will develop VTE.
Likelihood of Developing a VTE: (See figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Extremely rarely, thrombosis has been reported to occur in other blood vessels, e.g., hepatic, mesenteric, renal, cerebral or retinal veins and arteries, in CHC users.
Symptoms of venous or arterial thrombotic/thromboembolic events or of a cerebrovascular accident can include: unilateral leg pain and/or swelling; sudden severe pain in the chest, whether or not it radiates to the left arm; sudden breathlessness; sudden onset of coughing; any unusual, severe, prolonged headache; sudden partial or complete loss of vision; diplopia; slurred speech or aphasia; vertigo; collapse with or without focal seizure; weakness or very marked numbness suddenly affecting one side or one part of the body; motor disturbances; 'acute' abdomen.
The risk of venous thromboembolism increases with: increasing age; a positive family history (i.e. venous thromboembolism ever in a sibling or parent at a relatively early age). If a hereditary predisposition is suspected, the woman should be referred to a specialist for advice before deciding about any hormonal contraceptive use; obesity (body mass index over 30 kg/m
2); prolonged immobilisation, major surgery, any surgery to the legs, or major trauma. In these situations it is advisable to discontinue COC use (in the case of elective surgery at least four weeks in advance) and not to resume until two weeks after complete remobilisation. See also 'Contraindications' and possibly also with superficial thrombophlebitis and varicose veins. There is no consensus about the possible role of these conditions in the etiology of venous thromboembolism.
The risk of arterial thromboembolic complications increases with: increasing age; smoking (with heavier smoking and increasing age the risk further increases, especially in women over 35 years of age); dyslipoproteinaemia; obesity (body mass index over 30 kg/m
2); hypertension; migraine; valvular heart disease; atrial fibrillation; a positive family history (i.e. arterial thrombosis ever in a sibling or parent at a relatively early age). If a hereditary predisposition is suspected, the woman should be referred to a specialist for advice before deciding about any hormonal contraceptive use.
The increased risk of thromboembolism in the puerperium must be considered (for information on "Pregnancy and Lactation" see Use in Pregnancy & Lactation).
Other medical conditions which have been associated with adverse circulatory events include diabetes mellitus, systemic lupus erythematosus, haemolytic uraemic syndrome, chronic inflammatory bowel disease (Crohn's disease or ulcerative colitis) and sickle cell disease.
An increase in frequency or severity of migraine during COC use (which may be prodromal of a cerebrovascular event) may be a reason for immediate discontinuation of the COC.
Biochemical factors that may be indicative of hereditary or acquired predisposition for venous or arterial thrombosis include Activated Protein C (APC) resistance, hyperhomocysteinaemia, antithrombin-III deficiency, protein C deficiency, protein S deficiency, antiphospholipid antibodies (anticardiolipin antibodies, lupus anticoagulant).
When considering risk/benefit, the physician should take into account that adequate treatment of a condition may reduce the associated risk of thrombosis.
Tumours: The most important risk factor for cervical cancer is persistent human papilloma virus (HPV) infection. Epidemiological studies have indicated that long-term use of COCs contributes to this increased risk, but there continues to be uncertainty about the extent to which this finding is attributable to confounding effects, like increased cervical screening and difference in sexual behavior including use of barrier contraceptives, or a causal association.
A meta-analysis from 54 epidemiological studies reported that there is a slightly increased relative risk (RR = 1.24) of having breast cancer diagnosed in women who are currently using COCs. The excess risk gradually disappears during the course of the 10 years after cessation of COC use. Because breast cancer is rare in women under 40 years of age, the excess number of breast cancer diagnoses in current and recent COC users is small in relation to the overall risk of breast cancer. The breast cancers diagnosed in ever-users tend to be less advanced clinically than the cancers diagnosed in never-users.
In another epidemiological study of 1.8 million Danish women followed an average of 10.9 years, the reported RR of breast cancer among COC users increased with longer duration of use compared with women who never used COCs (overall RR = 1.19; RR ranged from 1.17 for 1 to less than 5 years of use to 1.46 after more than 10 years of use). The reported absolute risk difference (number of breast cancer cases between never-users compared with current and recent COC users) was small: 13 per 100,000 woman-years.
Epidemiological studies do not provide evidence for causation. The observed pattern of increased risk may be due to an earlier diagnosis of breast cancer in COC users, the biological effects of COCs or a combination of both.
In rare cases, benign liver tumours, and even more rarely, malignant liver tumours have been reported in users of COCs. In isolated cases, these tumours have led to life-threatening intra-abdominal haemorrhages. A hepatic tumour should be considered in the differential diagnosis when severe upper abdominal pain, liver enlargement or signs of intra-abdominal haemorrhage occur in women taking COCs.
Hepatitis C: During clinical trials with the HCV combination drug regimen ombitasvir/paritaprevir/ritonavir with and without dasabuvir, ALT elevations greater than 5 times the upper limit of normal (ULN) were significantly more frequent in women using ethinylestradiol-containing medications such as CHCs. Marvelon must be discontinued prior to starting therapy with the combination drug regimen ombitasvir/paritaprevir/ritonavir with or without dasabuvir (see Contraindications and Interactions). Marvelon can be restarted approximately 2 weeks following completion of treatment with the combination drug regimen.
Other conditions: Women with hypertriglyceridaemia, or a family history thereof, may be at an increased risk of pancreatitis when using COCs.
Although small increases in blood pressure have been reported in many women taking COCs, clinically relevant increases are rare. A relationship between COC use and clinical hypertension has not been established. However, if a sustained clinically significant hypertension develops during the use of a COC then it is prudent for the physician to withdraw the COC and treat the hypertension. Where considered appropriate, COC use may be resumed if normotensive values can be achieved with antihypertensive therapy.
The following conditions have been reported to occur or deteriorate with both pregnancy and COC use, but the evidence of an association with COC use is inconclusive: jaundice and/or pruritus related to cholestasis; gallstone formation; porphyria; systemic lupus erythematosus; haemolytic uraemic syndrome; Sydenham's chorea; herpes gestationis; otosclerosis-related hearing loss; (hereditary) angioedema.
Acute or chronic disturbances of liver function may necessitate the discontinuation of COC use until markers of liver function return to normal. Recurrence of cholestatic jaundice which occurred first during pregnancy or previous use of sex steroids necessitates the discontinuation of COCs.
Although COCs may have an effect on peripheral insulin resistance and glucose tolerance, there is no evidence for a need to alter the therapeutic regimen in diabetics using low-dose COCs (containing < 0.05 mg ethinylestradiol). However, diabetic women should be carefully observed while taking COCs.
Crohn's disease and ulcerative colitis have been associated with COC use.
Chloasma may occasionally occur, especially in women with a history of chloasma gravidarum. Women with a tendency to chloasma should avoid exposure to the sun or ultraviolet radiation whilst taking COCs.
Marvelon contains < 80 mg lactose per tablet. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption who are on lactose-free diet should take this amount into consideration.
When counselling the choice of contraceptive method(s), all the previously mentioned information should be taken into account.
Medical Examination/Consultation: Prior to the initiation or reinstitution of Marvelon a complete medical history (including family history) should be taken and pregnancy must be ruled out. Blood pressure should be measured and if clinically indicated a physical examination should be performed, guided by the contra-indications (Contraindications) and warnings as previously mentioned. The woman should also be instructed to carefully read the user leaflet and to adhere to the advice given. The frequency and nature of further periodic checks should be based on established practice guidelines and be adapted to the individual woman.
Women should be advised that oral contraceptives do not protect against HIV infections (AIDS) and other sexually transmissible diseases.
Reduced efficacy: The efficacy of Marvelon may be reduced in the event of e.g., missed tablets (Management of missed tablets under Dosage & Administration), gastro-intestinal disturbances (Advice in case of gastro-intestinal disturbances under Dosage & Administration) or concomitant medications that decrease the plasma concentration of etonogestrel, the active metabolite of desogestrel (Interactions).
Reduced cycle control: With all COCs, irregular bleeding (spotting or breakthrough bleeding) may occur, especially during the first months of use. Therefore, the evaluation of any irregular bleeding is only meaningful after an adaptation interval of about three cycles.
If bleeding irregularities persist or occur after previously regular cycles, then non-hormonal causes should be considered and adequate diagnostic measures are indicated to exclude malignancy or pregnancy. These may include curettage.
In some women withdrawal bleeding may not occur during the tablet-free interval. If the COC has been taken according to the directions described in Dosage & Administration, it is unlikely that the woman is pregnant. However, if the COC has not been taken according to these directions prior to the first missed withdrawal bleed or if two withdrawal bleeds are missed, pregnancy must be ruled out before COC use is continued.
Effects on ability to drive and use machines: No effects on ability to drive and use machines have been observed.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
