Each ml of infusion contains Levofloxacin Hemihydrate equivalent to 5.0 mg of Levofloxacin Base.
Pharmacotherapeutic Group: quinolone antibacterials, fluoroquinolones. ATC Code: J01MA12.
Pharmacology: Pharmacodynamics: Levofloxacin is a synthetic antibacterial agent of the fluoroquinolone class and is the S (-) enantiomer of the racemic active substance ofloxacin.
Mechanism of action: As a fluoroquinolone antibacterial agent, levofloxacin acts on the DNA-DNA-gyrase complex and topoisomerase IV.
PK/PD relationship: The degree of the bactericidal activity of levofloxacin depends on the ratio of the maximum concentration in serum (Cmax) or the area under the curve (AUC) and the minimal inhibitory concentration (MIC).
Mechanism of resistance: Resistance to levofloxacin is acquired through a stepwise process by target site mutations in both type II topoisomerases, DNA gyrase and topoisomerase IV. Other resistance mechanisms such as permeation barriers (common in Pseudomonas aeruginosa) and efflux mechanisms may also affect susceptibility to levofloxacin. Cross-resistance between levofloxacin and other fluoroquinolones is observed. Due to the mechanism of action, there is generally no cross-resistance between levofloxacin and other classes of antibacterial agents.
Pharmacokinetics: Levofloxacin is rapidly and almost completely absorbed after oral use with peak plasma concentrations achieved within 1 hour of a dose. It is distributed into body tissues including the bronchial mucosa and lungs, but penetration into CSF is relatively poor. Levofloxacin is about 30 to 40% bound to plasma proteins. It is only metabolised to a small degree to inactive metabolites. The elimination half-life of Levofloxacin is 6 to 8 hours, although this may be prolonged in patients with renal impairment. Levofloxacin is excreted largely unchanged, primarily in the urine. It is not removed by haemodialysis or peritoneal dialysis.
Treatment of the following infections caused by Staphylococcus sp, Streptococcus pneumoniae, Streptococcus pyogenes, Streptococcus hemolyticus, Enterococcus sp and Peptostreptococcus sp, Neisseria gonorrhoeae, Moraxella catarrhalis, Propionibacterium acnes, Escherichia coli, Citrobacter, Salmonella sp (excluding S. typhi or S. paratyphi), Shigella sp, Klebsiella sp, Enterobacter sp, Serratia sp and Proteus sp, Vibrio cholerae, Pseudomonas aeruginosa, Haemophilus influenzae, Acinetobacter sp and Campylobacter sp or Chlamydia trachomatis susceptible to levofloxacin: Pneumonia, chronic bronchitis, diffuse panbronchiolitis, bronchiectasis with infection and secondary infections in chronic respiratory tract diseases. Laryngopharyngitis, tonsillitis (peritonsillitis, peritonsillar abscess) and acute bronchitis. Pyelonephritis, cystitis, prostatitis, epididymitis, gonococcal urethritis and nongonococcal urethritis.
Intrauterine infection, cervicitis, uterine adnexitis and bartholinitis. Folliculitis (including acne pustulosa), furuncle, furunculosis, carbuncle, impetigo contagiosa, erysipelas, phlegmon, lymphangitis/lymphadenitis, suppurative paronychia (including felon), subcutaneous abscess, hydradenitis, acne conglobata, infectious atheroma and periproctic abscess.
Mastitis, (superficial) secondary infections in traumatic wounds, burns, operative wound, etc.
Cholecystitis and cholangitis.
Otitis externa, otitis media, sinusitis and suppurative sialadenitis. Blepharitis, hordeolum, dacryocystitis, conjunctivitis and tarsadenitis. Bacterial dysentery, infectious enteritis, salmonella enteritis and cholera. Periodontitis, pericoronitis and gnathitis.
Treatment of adults (more than or equal to 18 years) with mild, moderate and severe infections caused by susceptible strains of the designated microorganisms in the conditions listed as follows. Levores 5mg/ml Solution for Infusion is indicated when IV administration offers a route of administration advantageous to the patient (eg, patient cannot tolerate an oral dosage form). (See Dosage & Administration.)
Acute maxillary sinusitis due to Streptococcus pneumoniae, Haemophilus influenzae or Moraxella catarrhalis.
Acute bacterial exacerbation of chronic bronchitis due to Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae, Haemophilus parainfluenzae or Moraxella catarrhalis.
Community-acquired pneumonia due to Staphylococcus aureus, Streptococcus pneumoniae, Legionella pneumophila or Mycoplasma pneumoniae.
Uncomplicated skin and skin structure infections (mild to moderate) including abscesses, cellulitis, furuncles, impetigo, pyoderma, wound infections, due to Staphylococcus aureus or Streptococcus pyogenes.
Complicated urinary tract infections (mild to moderate) due to Enterococcus faecalis, Enterobacter cloacae, Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis or Pseudomonas aeruginosa.
Acute pyelonephritis (mild to moderate) caused by Escherichia coli. Appropriate culture and susceptibility tests should be performed before treatment in order to isolate and identify organisms causing the infection and to determine their susceptibility to levofloxacin. Therapy with levofloxacin may be initiated before results of these tests are known; once results become available, appropriate therapy should be selected.
As with other drugs in this class, some strains of Pseudomonas aeruginosa may develop resistance fairly rapidly during treatment with levofloxacin. Culture and susceptibility testing performed periodically during therapy will provide information about the continued susceptibility of the pathogens to the antimicrobial agent and also the possible emergence of bacterial resistance.
Recommended Dosage: Levores 5mg/ml Solution for Infusion should only be administered by IV infusion. It is not for IM, intrathecal, intraperitoneal or SC administration.
Caution: Rapid or bolus IV infusion must be avoided. Levofloxacin injection should be infused IV slowly over a period of not less than 60 or 90 min, depending on the dosage (see Precautions).
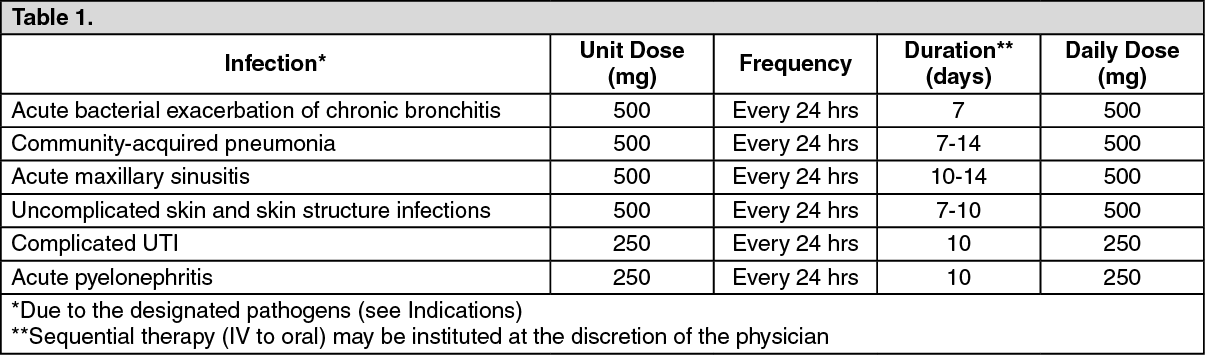
Usual Dose: 250 or 500 mg administered by slow infusion over 60 min every 24 hours or 750 mg administered orally or by slow infusion over 90 min every 24 hours, as indicated by infection and described in the following dosing chart. These recommendations apply to patients with normal renal function (ie, creatinine clearance >80 mL/min). For patients with altered renal function, see Table 2.
Patients with Normal Renal Function: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patients with Impaired Renal Function: See Table 2.
Click on icon to see table/diagram/image
When only the serum creatinine is known, the following formula may be used to estimate creatinine clearance: See equation.
Click on icon to see table/diagram/image
The serum creatinine should represent a steady state of renal function.
Mode of Administration: Intravenous Infusion.
According to toxicity studies in animals or clinical pharmacology studies performed with supra-therapeutic doses, the most important signs to be expected following acute overdosage of levofloxacin are central nervous system symptoms such as confusion, dizziness, impairment of consciousness, and convulsive seizures, increases in QT interval.
In the event of overdose, symptomatic treatment should be implemented. Electrocardiogram (ECG) monitoring should be undertaken, because of the possibility of QT interval prolongation. Haemodialysis, including peritoneal dialysis and CAPD, are not effective in removing levofloxacin from the body. No specific antidote exists.
Levores 5mg/ml Solution for Infusion must not be used: in patients hypersensitive to levofloxacin or any other quinolone and any of the excipients, in patients with epilepsy, in patients with history of tendon disorders related to fluoroquinolone administration, in children or growing adolescents, during pregnancy, in breast-feeding women.
Methicillin-resistant S. aureus are very likely to possess co-resistance to fluoroquinolones, including levofloxacin. Therefore levofloxacin is not recommended for the treatment of known or suspected MRSA infections unless laboratory results have confirmed susceptibility of the organism to levofloxacin (and commonly recommended antibacterial agents for the treatment of MRSA-infections are considered inappropriate).
Resistance to fluoroquinolones of E. coli - the most common pathogen involved in urinary tract infections - varies across the European Union. Prescribers are advised to take into account the local prevalence of resistance in E. coli to fluoroquinolones.
Inhalation Anthrax: Use in humans is based on in vitro Bacillus anthracis susceptibility data and on animal experimental data together with limited human data. Treating physicians should refer to national and/or international consensus documents regarding the treatment of anthrax.
Infusion Time: The recommended infusion time of at least 30 minutes for 250 mg or 60 minutes for 500 mg Tavanic solution for infusion should be observed. It is known for ofloxacin that during infusion tachycardia and a temporary decrease in blood pressure may develop. In rare cases, as a consequence of a profound drop in blood pressure, circulatory collapse may occur. Should a conspicuous drop in blood pressure occur during infusion of levofloxacin, (l-isomer of ofloxacin) the infusion must be halted immediately.
Sodium content: This medicinal product contains 7.8 mmol (181 mg) sodium per 50 ml dose and 15.8 mmol (363 mg) per 100ml dose. To be taken into consideration by patients on a controlled sodium diet.
Tendinitis and tendon rupture: Tendinitis may rarely occur. It most frequently involves the Achilles tendon and may lead to tendon rupture. Tendinitis and tendon rupture, sometimes bilateral, may occur within 48 hours of starting treatment with levofloxacin and have been reported up to several months after discontinuation of treatment. The risk of tendinitis and tendon rupture is increased in patients aged over 60 years, in patients receiving daily doses of 1000 mg and in patients using corticosteroids. The daily dose should be adjusted in elderly patients based on creatinine clearance. Close monitoring of these patients is therefore necessary if they are prescribed levofloxacin. All patients should consult their physician if they experience symptoms of tendinitis. If tendinitis is suspected, treatment with levofloxacin must be halted immediately, and appropriate treatment (e.g. immobilisation) must be initiated for the affected tendon.
Clostridium difficile-associated disease: Diarrhoea, particularly if severe, persistent and/or bloody, during or after treatment with levofloxacin (including several weeks after treatment), may be symptomatic of Clostridium difficile-associated disease (CDAD). CDAD may range in severity from mild to life threatening, the most severe form of which is pseudomembranous colitis. It is therefore important to consider this diagnosis in patients who develop serious diarrhoea during or after treatment with levofloxacin. If CDAD is suspected or confirmed, levofloxacin should be stopped immediately and appropriate treatment initiated without delay. Anti-peristaltic medicinal products are contraindicated in this clinical situation.
Patients predisposed to seizures: Quinolones may lower the seizure threshold and may trigger seizures. Levofloxacin is contraindicated in patients with a history of epilepsy and, as with other quinolones, should be used with extreme caution in patients predisposed to seizures or concomitant treatment with active substances that lower the cerebral seizure threshold, such as theophylline. In case of convulsive seizures, treatment with levofloxacin should be discontinued.
Patients with G-6- phosphate dehydrogenase deficiency: Patients with latent or actual defects in glucose-6-phosphate dehydrogenase activity may be prone to haemolytic reactions when treated with quinolone antibacterial agents. Therefore, if levofloxacin has to be used in these patients, potential occurrence of haemolysis should be monitored.
Hypersensitivity reactions: Levofloxacin can cause serious, potentially fatal hypersensitivity reactions (e.g. angioedema up to anaphylactic shock), occasionally following the initial dose. Patients should discontinue treatment immediately and contact their physician or an emergency physician, who will initiate appropriate emergency measures.
Severe bullous reactions: Cases of severe bullous skin reactions such as Stevens-Johnson syndrome or toxic epidermal necrolysis have been reported with levofloxacin. Patients should be advised to contact their doctor immediately prior to continuing treatment is skin and/or mucosal reactions occur.
Dysglycaemia: As with all quinolones, disturbances in blood glucose, including both hypoglycaemia and hyperglycaemia have been reported, usually in diabetic patients receiving concomitant treatment with an oral hypoglycaemic agent (e.g., glibenclamide) or with insulin. Cases of hypoglycaemic coma have been reported. In diabetic patients, careful monitoring of blood glucose is recommended.
Prevention of photosensitisation: Photosensitisation has been reported with levofloxacin. It is recommended that patients should not expose themselves unnecessarily to strong sunlight or to artificial UV rays (e.g. sunray lamp, solarium), during treatment and for 48 hours following treatment discontinuation in order to prevent photosensitisation.
Patients treated with Vitamin K antagonists: Due to possible increase in coagulation tests (PT/INR) and/or bleeding in patients treated with levofloxacin in combination with a vitamin K antagonist (e.g. warfarin), coagulation tests should be monitored when these drugs are given concomitantly.
Psychotic reactions: Psychotic reactions have been reported in patients receiving quinolones, including levofloxacin. In very rare cases these have progressed to suicidal thoughts and self-endangering behaviour- sometimes after only a single dose of levofloxacin. In the event that the patient develops these reactions, levofloxacin should be discontinued and appropriate measures instituted. Caution is recommended if levofloxacin is to be used in psychotic patients or in patients with history of psychiatric disease.
QT interval prolongation: Caution should be taken when using fluoroquinolones, including levofloxacin, in patients with known risk factors for prolongation of the QT interval such as, for example: congenital long QT syndrome; concomitant use of drugs that are known to prolong the QT interval (e.g. Class IA and III antiarrhythmics, tricyclic antidepressants, macrolides, antipsychotics); uncorrected electrolyte imbalance (e.g. hypokalemia, hypomagnesemia); cardiac disease (e.g. heart failure, myocardial infarction, bradycardia). Elderly patients and women may be more sensitive to QTc-prolonging medications. Therefore, caution should be taken when using fluoroquinolones, including levofloxacin, in these populations.
Peripheral neuropathy: Peripheral sensory neuropathy and peripheral sensory motor neuropathy have been reported in patients receiving fluoroquinolones, including levofloxacin, which can be rapid in its onset. Levofloxacin should be discontinued if the patient experiences symptoms of neuropathy in order to prevent the development of an irreversible condition.
Hepatobiliary disorders: Cases of hepatic necrosis up to fatal hepatic failure have been reported with levofloxacin, primarily in patients with severe underlying diseases, e.g. sepsis. Patients should be advised to stop treatment and contact their doctor if signs and symptoms of hepatic disease develop such as anorexia, jaundice, dark urine, pruritus or tender abdomen.
Exacerbation of myasthenia gravis: Fluoroquinolones, including levofloxacin, have neuromuscular blocking activity and may exacerbate muscle weakness in patients with myasthenia gravis. Postmarketing serious adverse reactions, including deaths and the requirements for respiratory support, have been associated with fluoroquinolone use in patients with myasthenia gravis. Levofloxacin is not recommended in patients with a known history of myasthenia gravis.
Vision disorders: If vision becomes impaired or any effects on the eyes are experienced, an eye specialist should be consulted immediately.
Superinfection: The use of levofloxacin, especially if prolonged, may result in overgrowth of non-susceptible organisms. If superinfection occurs during therapy, appropriate measures should be taken.
Interference with laboratory test: In patients treated with levofloxacin, determination of opiates in urine may give false-positive results. It may be necessary to confirm positive opiate screens by more specific method.
Levofloxacin may inhibit the growth of Mycobacterium tuberculosis and, therefore, may give false-negative results in the bacteriological diagnosis of tuberculosis.
Effects on ability to drive and use machines: Some undesirable effects (e.g. dizziness/vertigo, drowsiness, visual disturbances) may impair the patient's ability to concentrate and react, and therefore may constitute a risk in situations where these abilities are of special importance (e.g. driving a car or operating machinery).
Patients with renal impairment: Since levofloxacin is excreted mainly by the kidneys, the dose of Levores should be adjusted in patients with renal impairment.
Pregnancy: There are limited amount of data from the use of levofloxacin in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity. However in the absence of human data and due to that experimental data suggest a risk of damage by fluoroquinolones to the weight-bearing cartilage of the growing organism, levofloxacin must not be used in pregnant women.
Lactation: Levofloxacin is contraindicated in breast-feeding women. There is insufficient information on the excretion of levofloxacin in human milk; however other fluoroquinolones are excreted in breast milk. In the absence of human data and due to that experimental data suggest a risk of damage by fluoroquinolones to the weight-bearing cartilage of the growing organism, levofloxacin must not be used in breast-feeding women.
See Table 3.
Click on icon to see table/diagram/image
Other undesirable effects which have been associated with fluoroquinolone administration include: attacks of porphyria in patients with porphyria.
Effect of other medicinal products on Levofloxacin 5mg/ml Solution for Infusion and Caplet: Iron salts, zinc salts, magnesium- or aluminium-containing antacids, didanosine: Levofloxacin absorption is significantly reduced when iron salts, or magnesium- or aluminium-containing antacids, or didanosine (only didanosine formulations with aluminium or magnesium containing buffering agents) are administered concomitantly with Levores. Concurrent administration of fluoroquinolones with multi-vitamins containing zinc appears to reduce their oral absorption. It is recommended that preparations containing divalent or trivalent cations such as iron salts, zinc salts or magnesium- or aluminium-containing antacids, or didanosine (only didanosine formulations with aluminium or magnesium containing buffering agents) should not be taken 2 hours before or after Levores administration. Calcium salts have a minimal effect on the oral absorption of levofloxacin.
Sucralfate: The bioavailability of Levores is significantly reduced when administered together with sucralfate. If the patient is to receive both sucralfate and Levores, it is best to administer sucralfate 2 hours after the Levores administration.
Theophylline, fenbufen or similar non-steroidal anti-inflammatory drugs: No pharmacokinetic interactions of levofloxacin were found with theophylline in a clinical study. However a pronounced lowering of the cerebral seizure threshold may occur when quinolones are given concurrently with theophylline, non-steroidal anti-inflammatory drugs, or other agents which lower the seizure threshold.
Levofloxacin concentrations were about 13% higher in the presence of fenbufen than when administered alone.
Probenecid and cimetidine: Probenecid and cimetidine had a statistically significant effect on the elimination of levofloxacin. The renal clearance of levofloxacin was reduced by cimetidine (24%) and probenecid (34%). This is because both drugs are capable of blocking the renal tubular secretion of levofloxacin. However, at the tested doses in the study, the statistically significant kinetic differences are unlikely to be of clinical relevance.
Caution should be exercised when levofloxacin is coadministered with drugs that affect the tubular renal secretion such as probenecid and cimetidine, especially in renally impaired patients.
Other relevant information: Clinical pharmacology studies have shown that the pharmacokinetics of levofloxacin were not affected to any clinically relevant extent when levofloxacin was administered together with the following drugs: calcium carbonate, digoxin, glibenclamide, ranitidine.
Effect of Levores 5mg/ml Solution for Infusion and Caplet on other medicinal products: Ciclosporin: The half-life of ciclosporin was increased by 33% when coadministered with levofloxacin.
Vitamin K antagonists: Increased coagulation tests (PT/INR) and/or bleeding, which may be severe, have been reported in patients treated with levofloxacin in combination with a vitamin K antagonist (e.g. warfarin). Coagulation tests, therefore, should be monitored in patients treated with vitamin K antagonists.
Drugs known to prolong QT interval: Levofloxacin, like other fluoroquinolones, should be used with caution in patients receiving drugs known to prolong the QT interval (e.g. Class IA and III antiarrhythmics, tricyclic antidepressants, macrolides, antipsychotics).
Other relevant information: In a pharmacokinetic interaction study, levofloxacin did not affect the pharmacokinetics of theophylline (which is a probe substrate for CYP1A2), indicating that levofloxacin is not a CYP1A2 inhibitor.
Other forms of interactions: Food: There is no clinically relevant interaction with food. Levores caplet may therefore be administered regardless of food intake.
Incompatibilities: In the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products. Levofloxacin 5mg/ml Solution for Infusion should not be mixed with heparin or alkaline solutions (e.g. sodium hydrogen carbonate).
Store below 30°C, protect from light.
The in-use (once rubber stopper perforated) storage condition and shelf life of Levores 5mg/ml Solution for Infusion will remain stable until 12 hours in room temperature (<25°C).
Shelf-Life: 24 months.
J01MA12 - levofloxacin ; Belongs to the class of fluoroquinolones. Used in the systemic treatment of infections.
Levores soln for infusion 5 mg/mL
100 mL x 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image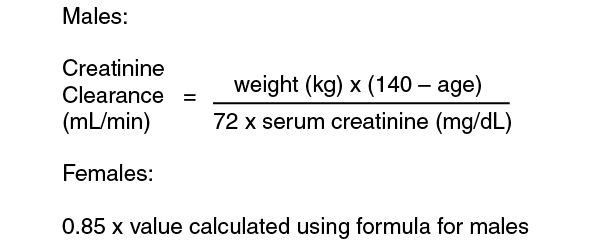 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image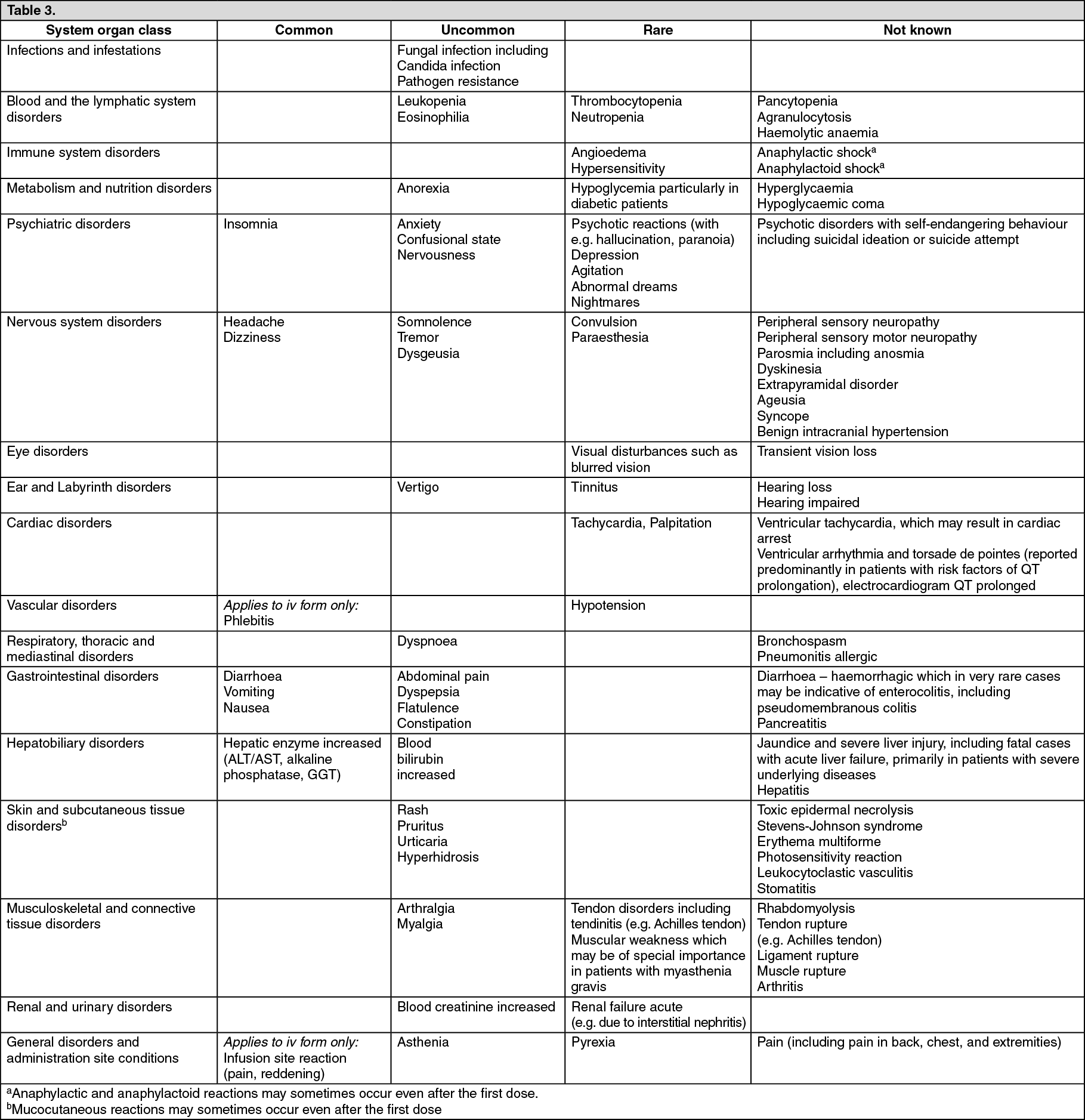 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
