


 Sign Out
Sign Out

For all indications described as follows: Dose is modified based upon clinical and laboratory findings (see Precautions).
Dose adjustments, during treatment and restart of treatment, are recommended to manage grade 3 or 4 thrombocytopenia, neutropenia, or other grade 3 or 4 toxicity judged to be related to lenalidomide.
In case of neutropenia, the use of growth factors in patient management should be considered.
If less than 12 hours has elapsed since missing a dose, the patient can take the dose. If more than 12 hours has elapsed since missing a dose at the normal time, the patient should not take the dose, but take the next dose at the normal time on the following day.
Posology: Newly diagnosed multiple myeloma (NDMM): Lenalidomide maintenance in patients who have undergone autologous stem cell transplantation (ASCT): Lenalidomide maintenance should be initiated after adequate haematologic recovery following ASCT in patients without evidence of progression. Lenalidomide must not be started if the Absolute Neutrophil Count (ANC) is < 1.0 x 109/L, and/or platelet counts are < 75 x 109/L.
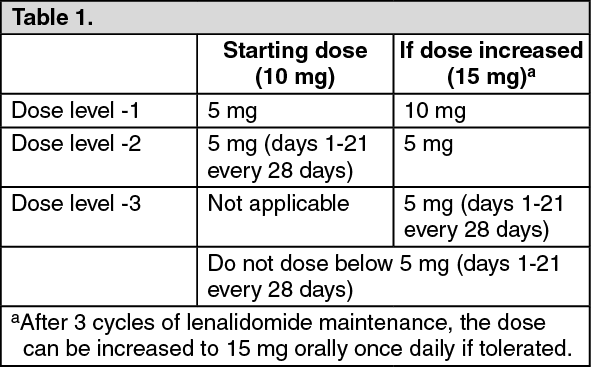
Recommended dose: The recommended starting dose is lenalidomide 10 mg orally once daily continuously (on days 1 to 28 of repeated 28-day cycles) given until disease progression or intolerance. After 3 cycles of lenalidomide maintenance, the dose can be increased to 15 mg orally once daily if tolerated.
Dose reduction steps: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThrombocytopenia: See Table 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNeutropenia: See Table 3.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLenalidomide in combination with dexamethasone until disease progression in patients who are not eligible for transplant: Lenalidomide treatment must not be started if the ANC is < 1.0 x 109/L, and/or platelet counts are < 50 x 109/L.
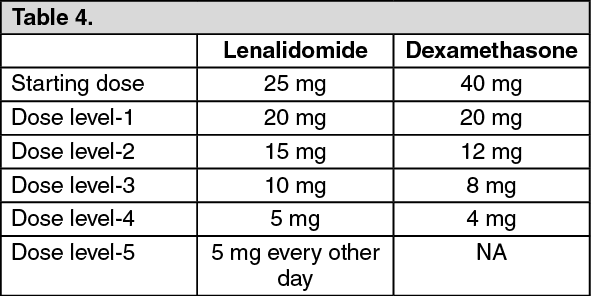
Recommended dose: The recommended starting dose of lenalidomide is 25 mg orally once daily on days 1 to 21 of repeated 28-day cycles.
The recommended dose of dexamethasone is 40 mg orally once daily on days 1, 8, 15 and 22 of repeated 28-day cycles. Patients may continue lenalidomide and dexamethasone therapy until disease progression or intolerance.
Dose reduction steps: See Table 4.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThrombocytopenia: See Table 5.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNeutropenia: See Table 6.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIf the dose of lenalidomide was reduced for a hematologic DLT, the dose of lenalidomide may be re-introduced to the next higher dose level (up to the starting dose) at the discretion of the treating physician if continued lenalidomide / dexamethasone therapy resulted in improved bone marrow function (no DLT for at least 2 consecutive cycles and an ANC ≥1,500/μL with a platelet count ≥ 100,000/μL at the beginning of a new cycle at the current dose level).
Multiple myeloma with at least one prior therapy: Lenalidomide treatment must not be started if the ANC < 1.0 x 109/L, and/or platelet counts < 75 x 109/L or, dependent on bone marrow infiltration by plasma cells, platelet counts < 30 x 109/L.
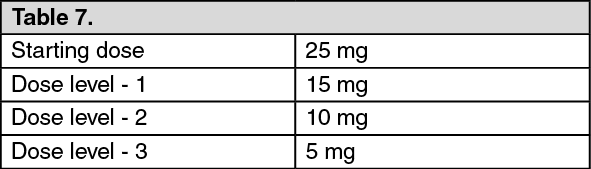
Recommended dose: The recommended starting dose of lenalidomide is 25 mg orally once daily on days 1 to 21 of repeated 28-day cycles. The recommended dose of dexamethasone is 40 mg orally once daily on days 1 to 4, 9 to 12, and 17 to 20 of each 28-day cycle for the first 4 cycles of therapy and then 40 mg once daily on days 1 to 4 every 28 days. Prescribing physicians should carefully evaluate which dose of dexamethasone to use, taking into account the condition and disease status of the patient.
Dose reduction steps: See Table 7.
 Click on icon to see table/diagram/image
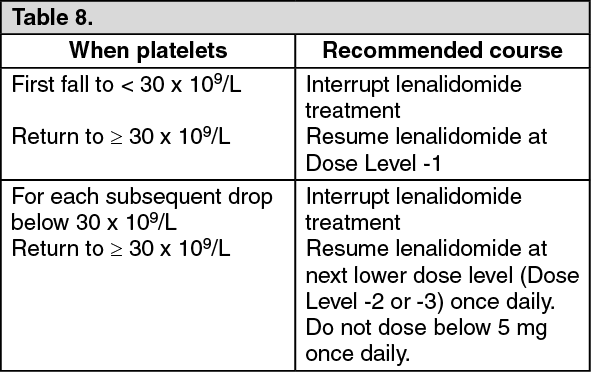
Click on icon to see table/diagram/imageThrombocytopenia: See Table 8.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNeutropenia: See Table 9.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAll indications: For other grade 3 or 4 toxicities judged to be related to lenalidomide, treatment should be stopped and only restarted at next lower dose level when toxicity has resolved to ≤ grade 2 depending on the physician's discretion.
Lenalidomide interruption or discontinuation should be considered for grade 2 or 3 skin rash. Lenalidomide must be discontinued for angioedema, grade 4 rash, exfoliative or bullous rash, or if Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN) or Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) is suspected and should not be resumed following discontinuation from these reactions.
Special populations: Paediatric population: Lenangio should not be used in children and adolescents from birth to less than 18 years because of safety concerns.
Older people: Currently available pharmacokinetic data are described in Pharmacology: Pharmacokinetics under Actions. Lenalidomide has been used in multiple myeloma patients up to 91 years of age.
In patients with newly diagnosed multiple myeloma aged 75 years and older who received lenalidomide, there was a higher incidence of serious adverse reactions and adverse reactions that led to treatment discontinuation (see Precautions). Patients with newly diagnosed multiple myeloma aged 75 years and older should be carefully assessed before treatment is considered (see Precautions). Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection and it would be prudent to monitor renal function.
Newly diagnosed multiple myeloma: For patients older than 75 years of age treated with lenalidomide in combination with dexamethasone, the starting dose of dexamethasone is 20 mg once daily on days 1, 8, 15 and 22 of each 28-day treatment cycle.
Lenalidomide combined therapy was less tolerated in newly diagnosed multiple myeloma patients older than 75 years of age compared to the younger population. These patients discontinued at a higher rate due to intolerance (Grade 3 or 4 adverse events and serious adverse events), when compared to patients < 75years.
Multiple myeloma: patients with at least one prior therapy: The percentage of multiple myeloma patients aged 65 or over was not significantly different between the lenalidomide/dexamethasone and placebo/dexamethasone groups. No overall difference in safety or efficacy was observed between these patients and younger patients, but greater pre-disposition of older individuals cannot be ruled out.
Patients with renal impairment: Lenalidomide is substantially excreted by the kidney; patients with greater degrees of renal impairment can have impaired treatment tolerance. Care should be taken in dose selection and monitoring of renal function is advised.
No dose adjustments are required for patients with mild renal impairment.
The following dose adjustments are recommended at the start of therapy and throughout treatment for patients with moderate or severe impaired renal function or end stage renal disease. There are no data available for patients with End Stage Renal Disease (ESRD) (CLcr < 30 mL/min, requiring dialysis).
Multiple myeloma: See Table 10.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAfter initiation of lenalidomide therapy, subsequent lenalidomide dose modification in renally impaired patients should be based on individual patient treatment tolerance, as described previously.
Patients with hepatic impairment: Lenalidomide has not formally been studied in patients with impaired hepatic function and there are no specific dose recommendations.
Method of administration: Oral use.
Lenangio capsules should be taken at about the same time on the scheduled days. The capsules should not be opened, broken or chewed. The capsules should be swallowed whole, preferably with water, either with or without food.
It is recommended to press only on one end of the capsule to remove it from the blister thereby reducing the risk of capsule deformation or breakage.