The tablets for oral administration contain either 25 mg or 50 mg of eplerenone.
Eplerenone is chemically described as Pregn-4-ene-7,21-dicarboxylic acid, 9,11-epoxy-17-hydroxy-3-oxo-, γ-lactone, methyl ester, (7α,11α,17α)-. Its empirical formula is C24H30O6 and it has a molecular weight of 414.50.
Excipients/Inactive Ingredients: Tablet core: Lactose monohydrate, Microcrystalline cellulose (E460), Croscarmellose sodium (E468), Hypromellose (E464), Sodium laurilsulfate, Talc (E553b), Magnesium stearate (E470b).
Tablet coating: Opadry yellow: Hypromellose (E464), Titanium dioxide (E171), Macrogol 400, Polysorbate 80 (E433), Iron oxide yellow (E172), Iron oxide red (E172).
Pharmacology: Pharmacodynamics: Mechanism of Action of Eplerenone: Eplerenone has relative selectivity in binding to recombinant human mineralocorticoid receptors compared to its binding to recombinant human glucocorticoid, progesterone and androgen receptors. Eplerenone prevents the binding of aldosterone, a key hormone in the renin-angiotensin-aldosterone-system (RAAS), which is involved in the regulation of blood pressure and the pathophysiology of cardiovascular disease.
Eplerenone has been shown to produce sustained increases in plasma renin and serum aldosterone, consistent with inhibition of the negative regulatory feedback of aldosterone on renin secretion. The resulting increased plasma renin activity and circulating aldosterone levels do not overcome the effects of eplerenone.
Heart Failure Post MI: In dose-ranging studies of chronic heart failure (NYHA classification II-IV), the addition of eplerenone to standard therapy resulted in expected dose-dependent increases in aldosterone.
Eplerenone was studied in EPHESUS, a double-blind, placebo-controlled study in 6632 subjects with acute MI, left ventricular dysfunction (as measured by LVEF ≤40%), and clinical signs of heart failure. Within 3 to 14 days (median 7 days) after an acute MI, patients received eplerenone or placebo in addition to standard therapies at an initial dose of 25 mg once daily and titrated to the target dose of 50 mg once daily after 4 weeks if serum potassium was <5.0 mmol/L. During the study, patients received standard care including acetylsalicylic acid (92%), ACE inhibitors (90%), beta blockers (83%), nitrates (72%), loop diuretics (66%), or HMG CoA reductase inhibitors (60%).
In EPHESUS, the co-primary endpoints were all-cause mortality and the combined endpoint of cardiovascular (CV) death or CV hospitalization; 14.4% of patients assigned to eplerenone and 16.7% of subjects assigned to placebo died (all causes), while 26.7% of patients assigned to eplerenone and 30.0% assigned to placebo met the combined endpoint of CV death or hospitalization. Thus, in EPHESUS, eplerenone reduced the risk of death from any cause by 15% (RR 0.85; 95% CI, 0.75-0.96; p = 0.008) compared to placebo, primarily by reducing CV mortality. The combined risk of CV death or CV hospitalization was reduced by 13% with eplerenone (RR 0.87; 95% CI, 0.79-0.95; p = 0.002). The absolute risk reductions for the endpoints all-cause mortality and combined CV mortality/hospitalization were 2.3% and 3.3%, respectively. Clinical efficacy was primarily demonstrated when eplerenone therapy was initiated in patients aged <75 years old. The benefits of therapy in those patients over the age of 75 are unclear. NYHA functional classification improved or remained stable for a statistically significant greater proportion of patients receiving eplerenone compared to placebo. The incidence of hyperkalemia was 3.4% in the eplerenone group vs. 2.0% in the placebo group (p < 0.001). The incidence of hypokalemia was 0.5% in the eplerenone group vs. 1.5% in the placebo group (p < 0.001).
Electrocardiography: No consistent effects of eplerenone on heart rate, QRS duration, or PR or QT interval were observed in 147 normal subjects evaluated for electrocardiographic changes during pharmacokinetic studies.
Pharmacokinetics: Absorption and Distribution: The absolute bioavailability of eplerenone is 69% following administration of a 100 mg oral tablet. Maximum plasma concentrations are reached after approximately 1.5 to 2 hours. Both peak plasma levels (Cmax) and area under the curve (AUC) are dose proportional for doses of 10 mg to 100 mg and less than proportional at doses above 100 mg. Steady-state is reached within 2 days. Absorption is not affected by food.
The plasma protein binding of eplerenone is about 50% and is primarily bound to alpha 1-acid glycoproteins. The apparent volume of distribution at steady-state is estimated to be 42-90 L. Eplerenone does not preferentially bind to red blood cells.
Metabolism and Excretion: Eplerenone metabolism is primarily mediated via CYP3A4. No active metabolites of eplerenone have been identified in human plasma.
Less than 5% of an eplerenone dose is recovered as unchanged drug in the urine and feces. Following a single oral dose of radiolabeled drug, approximately 32% of the dose was excreted in the feces and approximately 67% was excreted in the urine. The elimination half-life of eplerenone is approximately 3 to 6 hours. The apparent plasma clearance is approximately 10 L/hr.
Special Populations: Age, Gender, and Race: The pharmacokinetics of eplerenone at a dose of 100 mg once daily have been investigated in the elderly (≥65 years), in males and females, and in blacks. The pharmacokinetics of eplerenone did not differ significantly between males and females. At steady-state, elderly subjects had increases in Cmax (22%) and AUC (45%) compared with younger subjects (18 to 45 years). At steady-state, Cmax was 19% lower and AUC was 26% lower in blacks (see Dosage & Administration).
Renal Insufficiency: The pharmacokinetics of eplerenone were evaluated in patients with varying degrees of renal insufficiency and in patients undergoing hemodialysis. Compared with control subjects, steady-state AUC and Cmax were increased by 38% and 24%, respectively, in patients with severe renal impairment and were decreased by 26% and 3%, respectively, in patients undergoing hemodialysis. No correlation was observed between plasma clearance of eplerenone and creatinine clearance. Eplerenone is not removed by hemodialysis (see Overdosage).
Hepatic Insufficiency: The pharmacokinetics of eplerenone 400 mg have been investigated in patients with moderate (Child-Pugh Class B) hepatic impairment and compared with normal subjects. Steady-state Cmax and AUC of eplerenone were increased by 3.6% and 42%, respectively (see Dosage & Administration). Since the use of eplerenone has not been investigated in patients with severe hepatic impairment, eplerenone is contraindicated in this patient group (see Contraindications).
Heart Failure: The pharmacokinetics of eplerenone 50 mg were evaluated in patients with heart failure (NYHA classification II-IV). Compared with healthy subjects matched according to age, weight and gender, steady-state AUC and Cmax in heart failure patients were 38% and 30% higher, respectively. Consistent with these results, a population pharmacokinetic analysis of eplerenone based on a subset of patients from EPHESUS indicates that apparent clearance of eplerenone in patients with heart failure was similar to that in healthy elderly subjects.
Toxicology: Preclinical Safety Data: Carcinogenesis, Mutagenesis, Impairment of Fertility: Preclinical studies of safety pharmacology, genotoxicity, carcinogenic potential and reproductive toxicity revealed no special hazard for humans.
In repeated dose toxicity studies, prostate atrophy was observed in rats and dogs at exposure levels several-fold above clinical exposure levels. The prostatic changes were not associated with adverse functional consequences. The clinical relevance of these findings is unknown.
Studies in rats and rabbits showed no teratogenic effects, although decreased body weight in maternal rabbits and increased rabbit fetal resorptions and post-implantation loss were observed at the highest administered dosage.
Heart Failure - Post Myocardial Infarction (MI): Eplerenone is indicated, in addition to standard therapy, to reduce the risk of cardiovascular (CV) mortality and morbidity in stable patients with left ventricular dysfunction (left ventricular ejection fraction [LVEF] ≤40%) and clinical evidence of heart failure after recent myocardial infarction (MI).
Posology: For the individual adjustment of dose, the strengths of 25 mg and 50 mg are available. The maximum dose regimen is 50 mg daily.
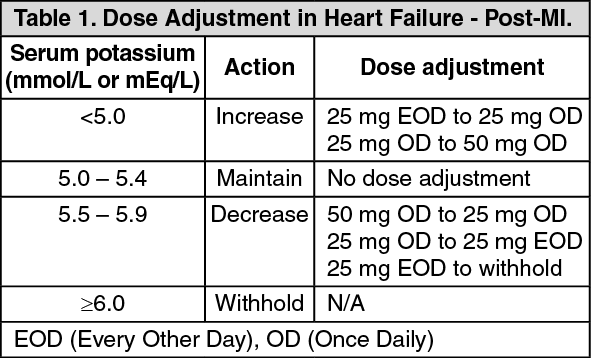
For post-MI heart failure patients: The recommended maintenance dose of eplerenone is 50 mg once daily (OD). Treatment should be initiated at 25 mg once daily and titrated to the target dose of 50 mg once daily preferably within 4 weeks, taking into account the serum potassium level (see Table 1).
Eplerenone therapy should usually be started within 3-14 days after an acute MI.
Patients with a serum potassium of >5.0 mmol/L should not be started on eplerenone (see Contraindications).
Serum potassium should be measured before initiating eplerenone therapy, within the first week and at one month after the start of treatment or dose adjustment. Serum potassium should be assessed as needed periodically thereafter.
After initiation, the dose should be adjusted based on the serum potassium level as shown in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Following withholding eplerenone due to serum potassium ≥6.0 mmol/L (or ≥6.0 mEq/L), eplerenone can be re-started at a dose of 25 mg every other day when potassium levels have fallen below 5.0 mmol/L (or 5.0 mEq/L).
General Considerations: Potassium: Serum potassium should be measured before initiating eplerenone therapy, within the first week and at one month after the start of treatment or dose adjustment. Serum potassium should be assessed periodically thereafter.
Food: Eplerenone may be administered with or without food.
Concomitant CYP3A4 Medications: Patients receiving mild to moderate CYP3A4 inhibitors, such as erythromycin, saquinavir, verapamil, and fluconazole should receive the dose of 25 mg once daily (see Interactions).
Special Populations and Special Considerations for Dosing: Use in children: Safety and efficacy of eplerenone has not been studied in pediatric patients with heart failure.
Elderly: No initial dose adjustment is required in the elderly. Due to an age-related decline in renal function, the risk of hyperkalemia is increased in elderly patients. This risk may be further increased when co-morbidity associated with increased systemic exposure is also present, in particular mild-to-moderate hepatic impairment. Periodic monitoring of serum potassium is recommended (see Precautions).
Use in renal impairment: No initial dose adjustment is required in patients with mild renal impairment. Periodic monitoring of serum potassium with dose adjustment according to Table 1 is recommended (see Precautions).
Patients with moderate renal impairment (CrCl 30-60 mL/min) should be started at 25 mg every other day, and dose should be adjusted based on the potassium level (see Table 1).
Periodic monitoring of serum potassium is recommended (see Precautions).
In patients with post-MI heart failure, there is no experience in patients with CrCl <50 mL/min.
Use in patients with severe renal impairment (CrCl <30 mL/min) is contraindicated (see Contraindications). Eplerenone is not dialysable.
Use in hepatic impairment: Mild-to-Moderate Hepatic Impairment: No initial dose adjustment is necessary (see Contraindications and Precautions).
No cases of adverse events associated with overdose of eplerenone in humans have been reported. The most likely manifestation of human overdose would be hypotension and/or hyperkalemia, consequently patients should be treated symptomatically and supportive measures instituted, as required. Eplerenone cannot be removed by hemodialysis. Eplerenone has been shown to bind extensively to charcoal.
Eplerenone is contraindicated in all patients with the following: Hypersensitivity to eplerenone or any component of this medication.
Clinically significant hyperkalemia or with conditions associated with hyperkalemia.
Serum potassium level >5.0 mmol/L (mEq/L) at initiation.
Moderate to severe renal impairment (creatinine clearance <50 mL/min) in post-MI heart failure (Eplerenone Post-acute Myocardial Infarction Heart failure Efficacy and Survival Study [EPHESUS]).
Severe hepatic impairment (Child-Pugh Class C).
Concomitant use with potassium-sparing diuretics, or potent inhibitors of CYP450 3A4 such as ketoconazole, itraconazole, and ritonavir (see Interactions).
Hyperkalemia: Eplerenone is associated with an increased risk of hyperkalemia. This risk can be minimized by patient selection, avoidance of certain concomitant treatments, and monitoring. Eplerenone should generally not be administered to patients who are receiving potassium supplements (see Contraindications). Potassium levels should be monitored regularly in patients with impaired renal function, including diabetic microalbuminuria (see as follows). Dose reduction of eplerenone has been shown to decrease serum potassium levels (see Dosage & Administration).
The risk of hyperkalemia may increase when eplerenone is used in combination with an Angiotensin-converting enzyme (ACE) inhibitor and/or an angiotensin receptor blocker (ARB).
CYP3A4 Inducers: Co-administration of eplerenone with potent CYP3A4 inducers is not recommended (see Interactions).
Information for Patients: Patients receiving eplerenone should be informed not to use potassium supplements, salt substitutes containing potassium, or contraindicated medications without consulting the prescribing healthcare professional.
Effects on Ability to Drive and Use Machines: No studies on the effect of eplerenone on the ability to drive or use machines have been performed. Eplerenone does not cause drowsiness or impairment of cognitive function but when driving vehicles or operating machines it should be taken into account that dizziness may occur during treatment.
Impaired Hepatic Function: Due to an increased systemic exposure to eplerenone in patients with mild-to-moderate hepatic impairment, frequent and regular monitoring of serum potassium is recommended in these patients, especially when elderly. The use of eplerenone in patients with severe hepatic impairment (Child-Pugh Class C) has not been evaluated and is therefore contraindicated (see Dosage & Administration and Contraindications).
Impaired Renal Function: See Hyperkalemia as previously mentioned and also Contraindications.
Use in the Elderly: Due to age-related decline in renal function, the risk of hyperkalemia is increased in elderly patients. Periodic monitoring of serum potassium is recommended.
Fertility/Pregnancy: Eplerenone has not been studied in pregnant women. Animal studies did not indicate direct or indirect adverse effects with respect to pregnancy, embryofetal development, parturition or post-natal development (see Pharmacology: Toxicology: Preclinical Safety Data under Actions). Caution should be exercised when prescribing eplerenone to pregnant women.
Lactation: It is unknown if eplerenone is excreted in human breast milk after oral administration. However, preclinical data show that eplerenone and/or metabolites are present in rat breast milk and that rat pups exposed by this route developed normally. Because many drugs are excreted in human milk and because of the unknown potential for adverse effects on the nursing infant, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother.
Heart Failure Post MI: In the (EPHESUS) study, the overall incidence of adverse events and the discontinuation rate due to adverse events reported with eplerenone was similar to placebo.
The most frequent adverse event reported in the EPHESUS study was hyperkalemia with an incidence rate of 3.4% for eplerenone, respectively.
Adverse events reported as follows are those with suspected relationship to treatment. Adverse events are listed by body system and absolute frequency. (See Table 2.)
Click on icon to see table/diagram/image
Pharmacodynamic interactions: Potassium-sparing diuretics and potassium supplements: Due to increased risk of hyperkalaemia, eplerenone should not be administered to patients receiving other potassium-sparing diuretics and potassium supplements (see Contraindications). Potassium-sparing diuretics may also potentiate the effect of antihypertensive agents and other diuretics.
ACE inhibitors, ARBs: The risk of hyperkalemia may increase when eplerenone is used in combination with an ACE inhibitor and/or an ARB. A close monitoring of serum potassium and renal function is recommended, especially in patients at risk for impaired renal function, e.g., the elderly. The triple combination of an ACE inhibitor and an ARB with eplerenone should not be used (see Contraindications and Precautions).
Lithium: Drug interaction studies of eplerenone have not been conducted with lithium. However, lithium toxicity has been reported in patients receiving lithium concomitantly with diuretics and ACE inhibitors (see Precautions). Co-administration of eplerenone and lithium should be avoided. If this combination appears necessary, lithium plasma concentrations should be monitored (see Precautions).
Cyclosporin, tacrolimus: Cyclosporin and tacrolimus may lead to impaired renal function and increase the risk of hyperkalaemia. The concomitant use of eplerenone and cyclosporin or tacrolimus should be avoided. If needed, close monitoring of serum potassium and renal function are recommended when cyclosporin and tacrolimus are to be administered during treatment with eplerenone (see Precautions).
Non-steroidal anti-inflammatory drugs (NSAIDs): Acute renal failure may occur in at risk patients (elderly, dehydrated subjects, using diuretics, with impaired renal function) due to decreased glomerular filtration (inhibition of vasodilatory prostaglandins due to non-steroidal anti-inflammatory drugs). These effects are generally reversible. Furthermore, there may be a reduction of the antihypertensive effect. Hydrate the patient and monitor renal function at the beginning of treatment and regularly during the combination (see Dosage & Administration and Precautions).
Trimethoprim: The concomitant administration of trimethoprim with eplerenone increases the risk of hyperkalaemia. Monitoring of serum potassium and renal function should be made, particularly in patients with renal impairment and in the elderly.
Alpha 1 blockers (e.g. prazosin, alfuzosin): When alpha-1-blockers are combined with eplerenone, there is the potential for increased hypotensive effect and/or postural hypotension. Clinical monitoring for postural hypotension is recommended during alpha-1-blocker co-administration.
Tricyclic anti-depressants, neuroleptics, amifostine, baclofen: Co-administration of these drugs with eplerenone may potentially increase antihypertensive effects and risk of postural hypotension.
Glucocorticoids, tetracosactide: Co-administration of these drugs with eplerenone may potentially decrease antihypertensive effects (sodium and fluid retention).
Pharmacokinetic interactions: In vitro studies indicate that eplerenone is not an inhibitor of CYP1A2, CYP2C19, CYP2C9, CYP2D6 or CYP3A4 isozymes. Eplerenone is not a substrate or an inhibitor of P-Glycoprotein.
Digoxin: Systemic exposure (AUC) to digoxin increases by 16% (90% CI: 4% - 30%) when co-administered with eplerenone. Caution is warranted when digoxin is dosed near the upper limit of therapeutic range.
Warfarin: No clinically significant pharmacokinetic interactions have been observed with warfarin. Caution is warranted when warfarin is dosed near the upper limit of therapeutic range.
CYP3A4 substrates: Results of pharmacokinetic studies with CYP3A4 probe-substrates, i.e., midazolam and cisapride, showed no significant pharmacokinetic interactions when these drugs were co-administered with eplerenone.
CYP3A4 inhibitors: Strong CYP3A4 inhibitors: Significant pharmacokinetic interactions may occur when eplerenone is co-administered with drugs that inhibit the CYP3A4 enzyme. A strong inhibitor of CYP3A4 (ketoconazole 200 mg BID) led to a 441% increase in AUC of eplerenone (see Contraindications). The concomitant use of eplerenone with strong CYP3A4 inhibitors such as ketoconazole, itraconazole, ritonavir, nelfinavir, clarithromycin, telithromycin and nefazodone, is contraindicated (see Contraindications).
Mild to moderate CYP3A4 inhibitors: Co-administration with erythromycin, saquinavir, amiodarone, diltiazem, verapamil, or fluconazole has led to significant pharmacokinetic interactions with rank order increases in AUC ranging from 98% to 187%. Eplerenone dosing should therefore not exceed 25 mg daily when mild to moderate inhibitors of CYP3A4 are co-administered with eplerenone (see Dosage & Administration).
CYP3A4 inducers: Co-administration of St. John's wort (a strong CYP3A4 inducer) with eplerenone caused a 30% decrease in eplerenone AUC. A more pronounced decrease in eplerenone AUC may occur with stronger CYP3A4 inducers, such as rifampicin. Due to the risk of decreased eplerenone efficacy, the concomitant use of strong CYP3A4 inducers (rifampicin, carbamazepine, phenytoin, phenobarbital, St. John's wort) with eplerenone is not recommended (see Precautions).
Antacids: Based on the results of a pharmacokinetic clinical study, no significant interaction is expected when antacids are co-administered with eplerenone.
Incompatibilities: Not applicable.
Instructions for Use and Handling: No special requirements.
No special precautions for storage.
Shelf-life: 36 months.
C03DA04 - eplerenone ; Belongs to the class of aldosterone antagonists. Used as potassium-sparing diuretics.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image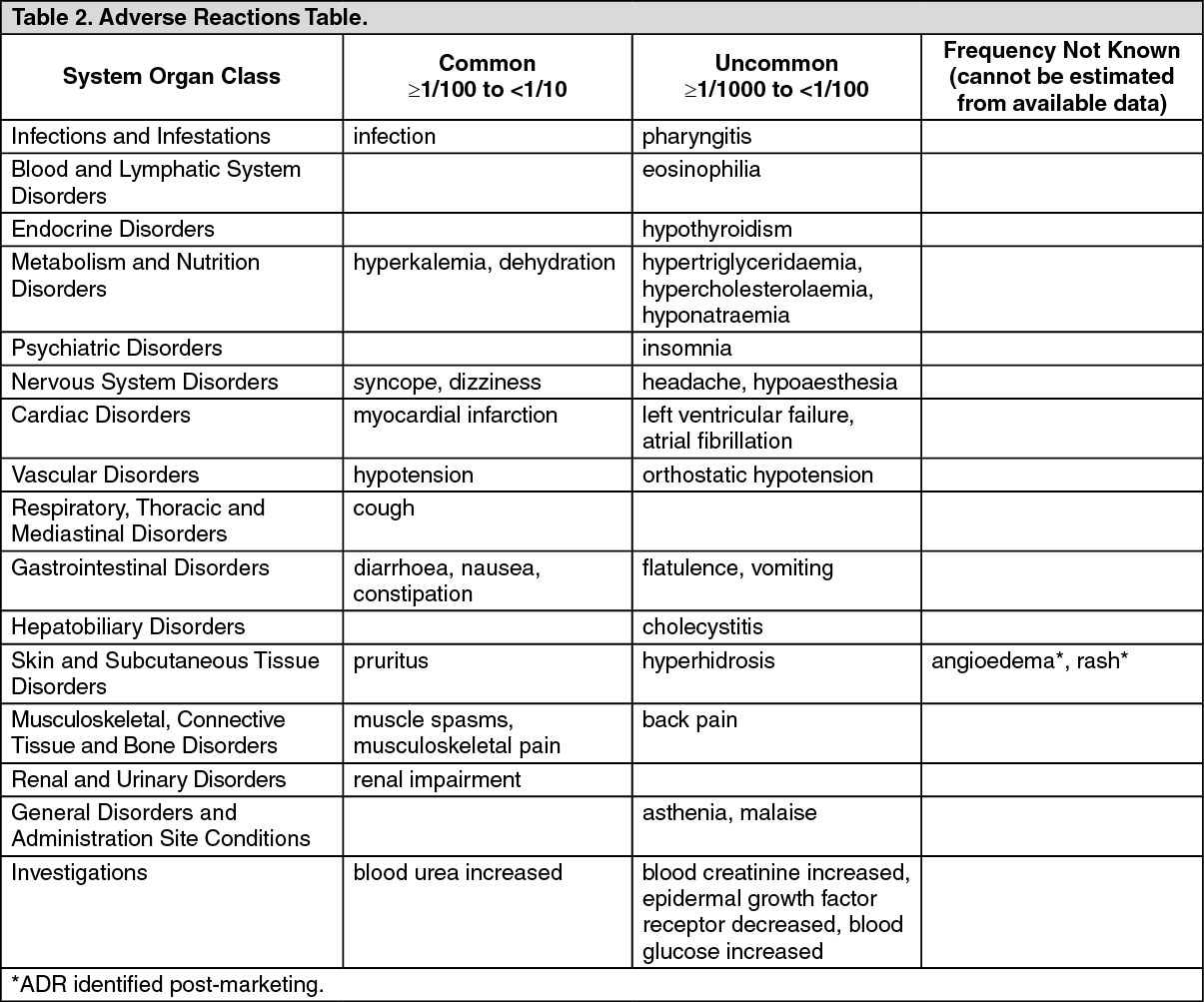 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
