Summary of the safety profile: For azathioprine, there is no modern clinical documentation which can be used as support for determining the frequency of undesirable effects. Undesirable effects may vary in their incidence depending on the indication.
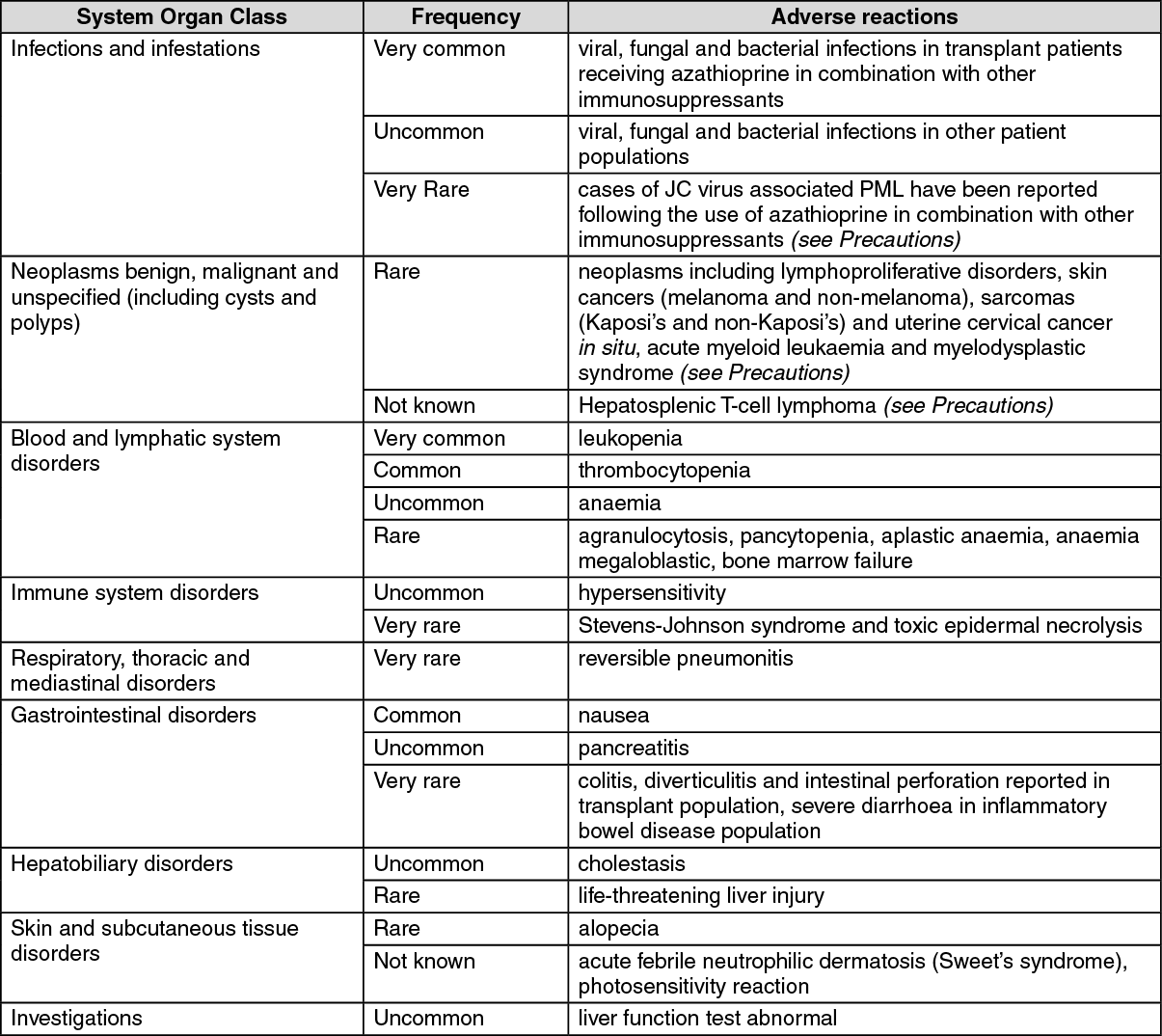
Tabulated summary of adverse reactions: The following convention has been utilised for the classification of frequency: Very common ≥1/10; common ≥1/100 and <1/10; uncommon ≥1/1000 and <1/100; rare ≥1/10,000 and <1/1000; very rare <1/10,000 and not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Description of selected adverse reactions: Infections and infestations:
Click on icon to see table/diagram/image
Description of selected adverse reactions: Infections and infestations: Patients receiving azathioprine alone or in combination with other immunosuppressants, particularly corticosteroids, have shown increased susceptibility to viral, fungal and bacterial infections, including severe or atypical infection, and reactivation with VZV, hepatitis B and other infectious agents.
Neoplasms benign, malignant and unspecified (including cysts and polyps): Patients receiving immunosuppressive therapy, including azathioprine are at an increased risk of developing lymphoproliferative disorders and other malignancies, notably skin cancers (melanoma and non-melanoma), sarcomas (Kaposi's and non-Kaposi's) and uterine cervical cancer
in situ. The increased risk appears to be related to the degree and duration of immunosuppression. It has been reported that discontinuation of immunosuppression may provide partial regression of the lymphoproliferative disorder.
There have been rare reports of acute myeloid leukaemia and myelodysplasia (some in association with chromosomal abnormalities).
Blood and lymphatic system disorders: Azathioprine may be associated with a dose-related, generally reversible, depression of bone marrow function, most frequently expressed as leukopenia, but also sometimes as anaemia and thrombocytopenia and rarely as agranulocytosis, pancytopenia and aplastic anaemia. These occur particularly in patients predisposed to myelotoxicity, such as those with TPMT deficiency and renal or hepatic insufficiency and in patients failing to reduce the dose of azathioprine when receiving concurrent allopurinol therapy.
Reversible, dose-related increases in mean corpuscular volume and red cell haemoglobin content have occurred in association with azathioprine therapy. Megaloblastic bone marrow changes have also been observed but severe megaloblastic anaemia and erythroid hypoplasia are rare.
Immune system disorders: Several different clinical syndromes, which appear to be idiosyncratic manifestations of hypersensitivity, have been described occasionally following administration of azathioprine. Clinical features include general malaise, dizziness, nausea, vomiting, diarrhoea, fever, rigors, exanthema, rash, vasculitis, erythema nodosum, myalgia, arthralgia, hypotension, renal dysfunction, hepatic dysfunction and cholestasis (see Hepatobiliary disorders as follows).
In many cases, rechallenge has confirmed an association with azathioprine.
Immediate withdrawal of azathioprine and institution of circulatory support where appropriate have led to recovery in the majority of cases.
Other marked underlying pathology has contributed to the very rare deaths reported.
Following a hypersensitivity reaction to azathioprine, the necessity for continued administration of azathioprine should be carefully considered on an individual basis.
Gastrointestinal disorders: Some patients experience nausea when first given oral azathioprine. This appears to be relieved by administering the tablets after meals. However, administration of azathioprine tablets after meals may reduce oral absorption, therefore monitoring for therapeutic efficacy should be considered after administration in this way (see Pharmacology: Pharmacokinetics under Actions).
Serious complications, including colitis, diverticulitis and bowel perforation, have been described in transplant recipients receiving immunosuppressive therapy. However, the aetiology is not clearly established and high-dose corticosteroids may be implicated. Severe diarrhoea, recurring on rechallenge, has been reported in patients treated with azathioprine for inflammatory bowel disease. The possibility that exacerbation of symptoms might be drug-related should be borne in mind when treating such patients.
Pancreatitis has been reported in a small percentage of patients on azathioprine therapy, particularly in renal transplant patients and those diagnosed as having inflammatory bowel disease. There are difficulties in relating the pancreatitis to the administration of one particular drug, although rechallenge has confirmed an association with azathioprine on occasions.
Hepatobiliary disorders: Cholestasis and deterioration of liver function have occasionally been reported in association with azathioprine therapy and are usually reversible on withdrawal of therapy. This may be associated with symptoms of a hypersensitivity reaction (see Immune system disorders as previously mentioned).
Rare, but life-threatening hepatic damage associated with chronic administration of azathioprine has been described primarily in transplant patients. Histological findings include sinusoidal dilatation, peliosis hepatis, venoocclusive disease and nodular regenerative hyperplasia. In some cases withdrawal of azathioprine has resulted in either a temporary or permanent improvement in liver histology and symptoms.
Skin and subcutaneous tissue disorders: Hair loss has been described on a number of occasions in patients receiving azathioprine and other immunosuppressive agents. In many instances the condition resolved spontaneously despite continuing therapy. The relationship between alopecia and azathioprine treatment is uncertain.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
