


 Sign Out
Sign Out




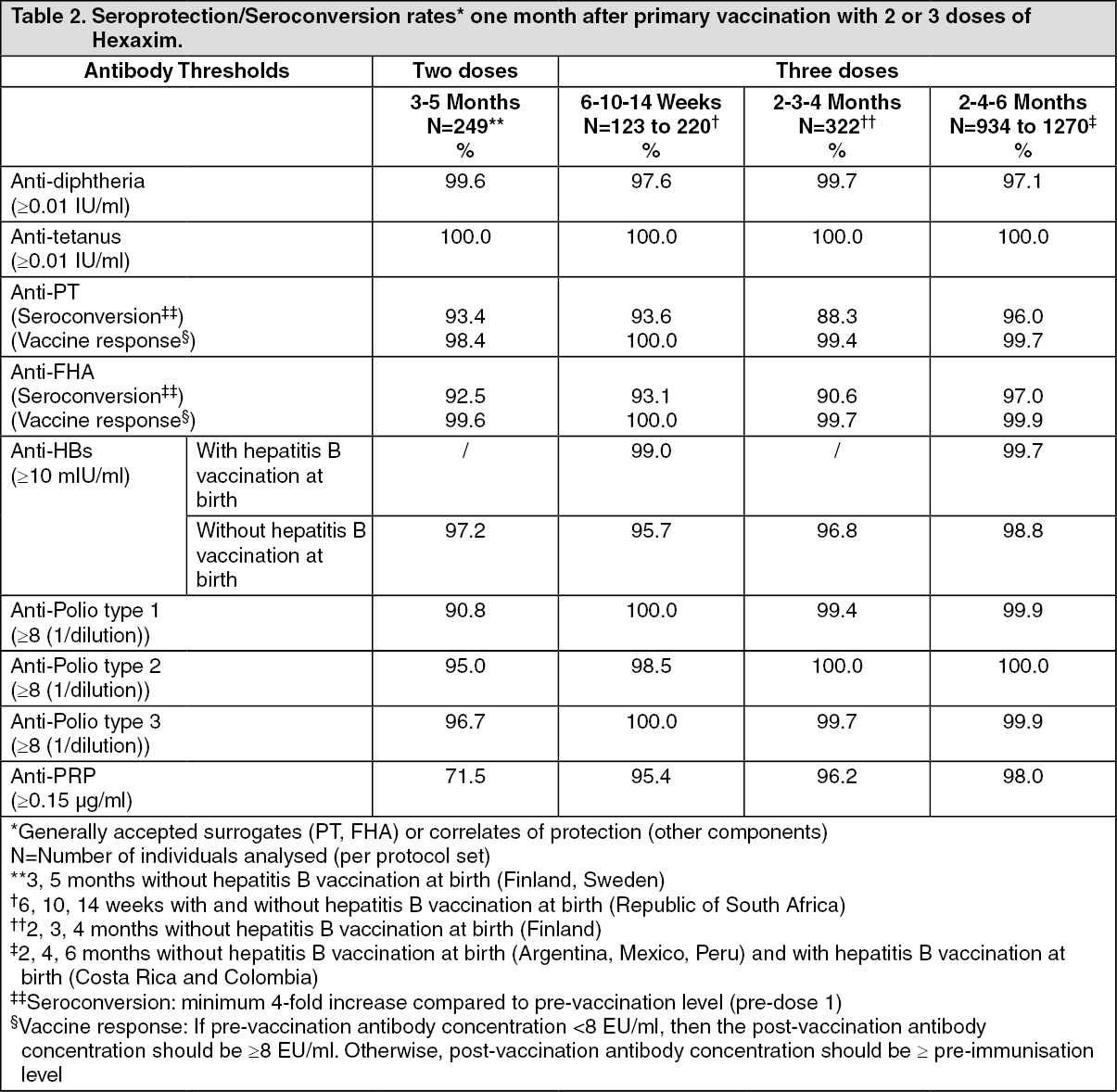
Pharmacology: Pharmacodynamics: Results obtained for each of the components are summarised in the tables as follows: (See Tables 2 and 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image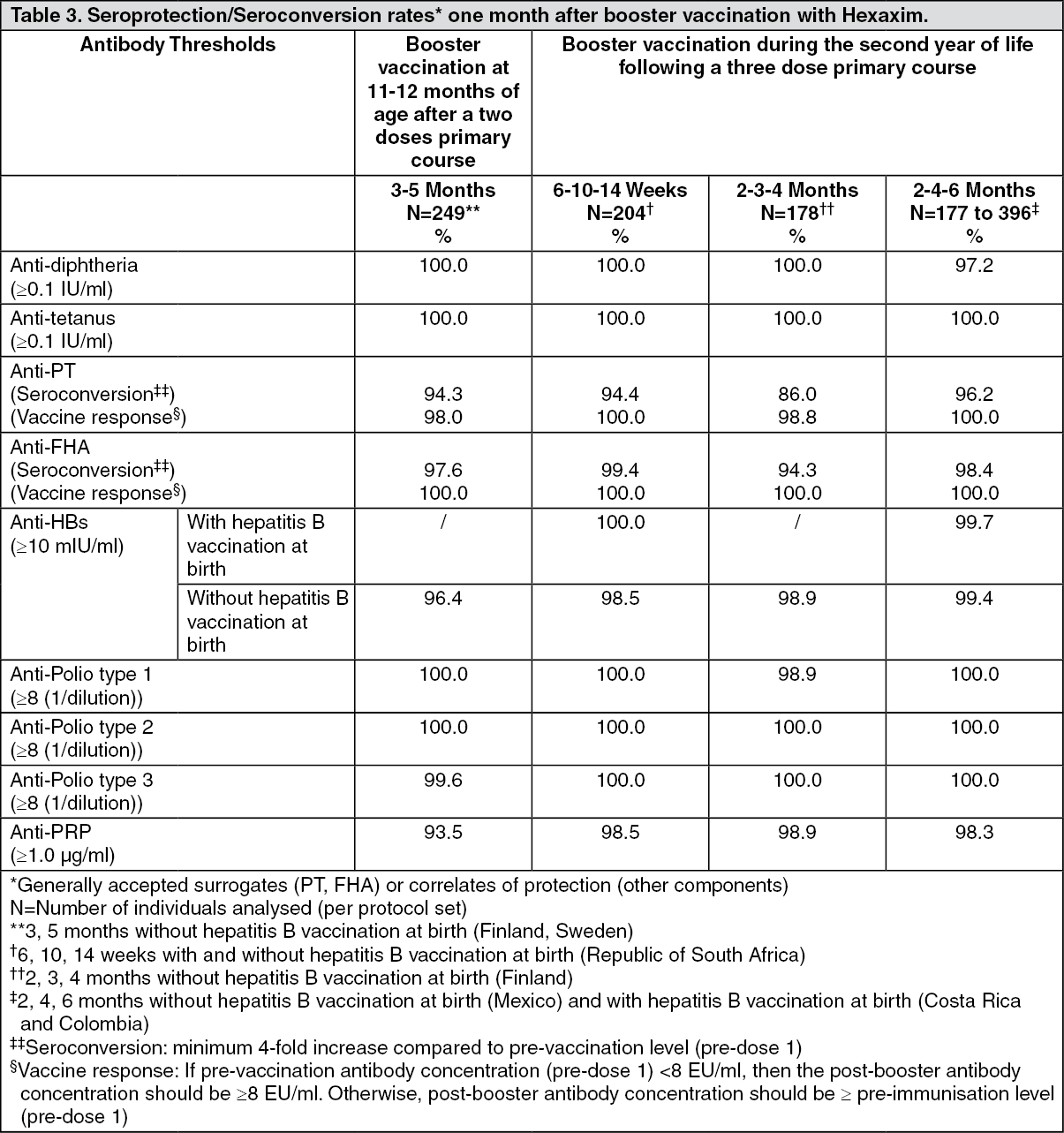 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageImmune responses to Hib and pertussis antigens after 2 doses at 2 and 4 months of age: The immune responses to Hib (PRP) and pertussis antigens (PT and FHA) were evaluated after 2 doses in a subset of subjects receiving Hexaxim (N=148) at 2, 4, 6 months of age. The immune responses to PRP, PT and FHA antigens one month after a 2 doses given at 2 and 4 months of age were similar to those observed one month after a 2-dose priming given at 3 and 5 months of age: anti-PRP titers ≥ 0.15 μg/ml were observed in 73.0% of individuals, anti-PT vaccine response in 97.9% of individuals, anti-FHA vaccine response in 98.6% of individuals.
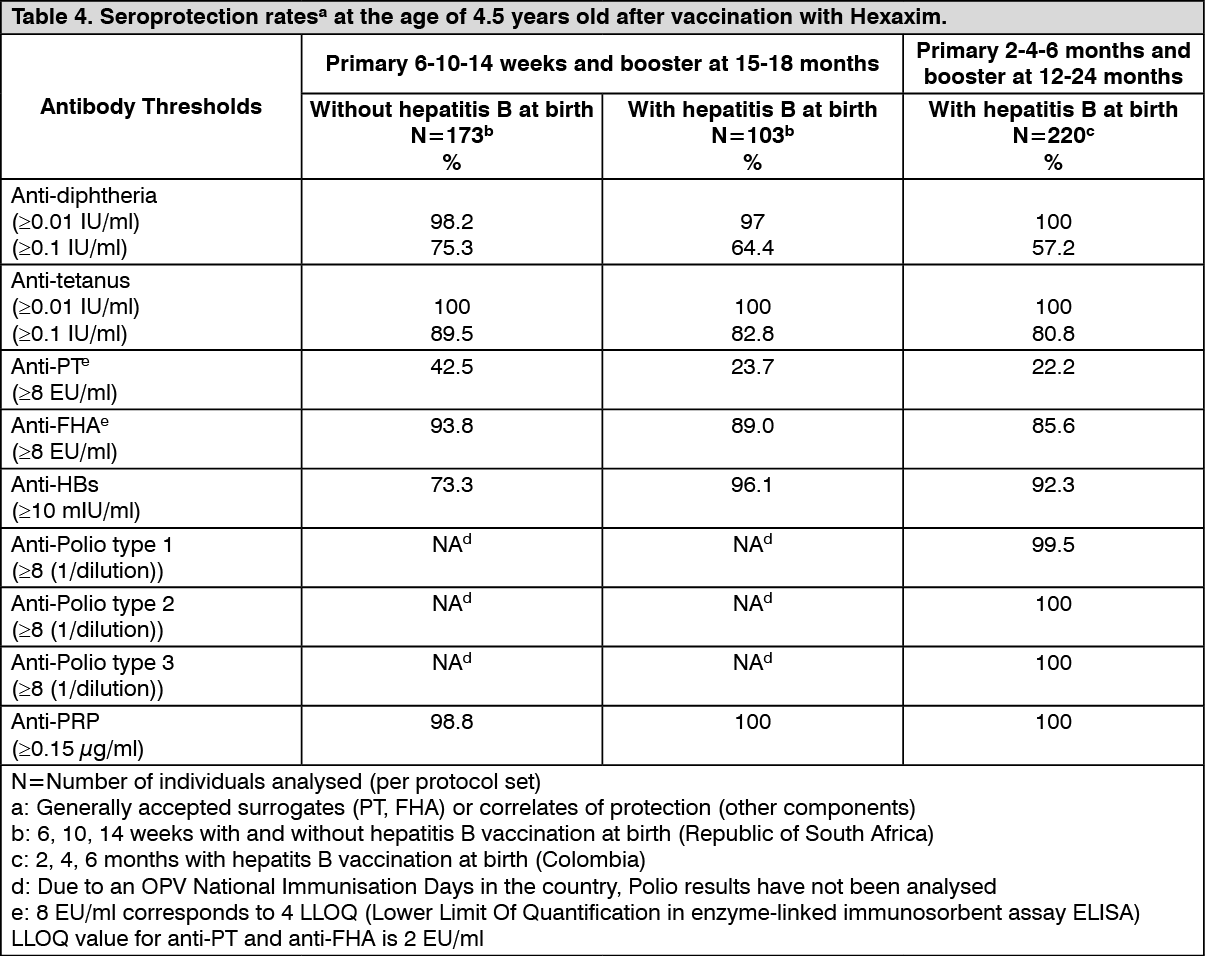
Persistence of immune response: Studies on long-term persistence of vaccine induced antibodies following varying infant/toddler primary series and following Hepatitis B vaccine given at birth or not have shown maintenance of levels above the recognized protective levels or antibody thresholds for the vaccine antigens (see Table 4).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe persistence of the immune responses against the hepatitis B component of Hexaxim was evaluated in infants primed with different schedules.
For a primary series consisting of one dose of hepatitis B vaccine given at birth followed by a 3-dose infant series at 2, 4, and 6 months of age without a toddler booster, 49.3% of children were seroprotected (anti-HBsAg ≥ 10 mIU/mL) at 9 years of age, and 92.8% presented an anamnestic response after a challenge dose with a standalone Hepatitis B vaccine.
These data support persisting immune memory induced in infants primed with Hexaxim.
Immune responses to Hexaxim in preterm infants: Immune responses to Hexaxim antigens in preterm (105) infants (born after a gestation period of 28 to 36 weeks), including 90 infants born to women vaccinated with Tdap vaccine during pregnancy and 15 to women not vaccinated during pregnancy, were evaluated following a 3-dose primary vaccination course at 2, 3, and 4 months of age, and a booster dose at 13 months of age.
One month after primary vaccination, all subjects were seroprotected against diphtheria (≥ 0.01 IU/mL), tetanus (≥ 0.01 IU/mL), and poliovirus types 1, 2 and 3 (≥ 8 (1/dilution)); 89.8% of subjects were seroprotected against hepatitis B (≥ 10 IU/mL) and 79.4% were seroprotected against Hib invasive diseases (≥ 0.15 μg/mL).
One month after the booster dose, all subjects were seroprotected against diphtheria (≥ 0.1 IU/mL), tetanus (≥ 0.1 IU/mL), and poliovirus types 1, 2 and 3 (≥ 8 (1/dilution)); 94.6% of subjects were seroprotected against hepatitis B (≥ 10 IU/mL) and 90.6% were seroprotected against Hib invasive diseases (≥ 1 μg/mL).
Regarding pertussis, one month after primary vaccination 98.7% and 100% of subjects developed antibodies ≥ 8 EU/mL against PT and FHA antigens, respectively. One month after the booster dose, 98.8% of subjects developed antibodies ≥ 8 EU/mL against both PT and FHA antigens. Pertussis antibody concentrations increased by 13-fold after primary vaccination and by 6- to 14-fold after the booster dose.
Immune responses to Hexaxim in infants born to women vaccinated with Tdap during pregnancy: Immune responses to Hexaxim antigens in term (109) and preterm (90) infants born to women vaccinated with Tdap vaccine during pregnancy (between 24 and 36 weeks of gestation) were evaluated following a 3-dose primary vaccination course at 2, 3, and 4 months of age, and a booster dose at 13 (preterm infants) or 15 (term infants) months of age.
One month after primary vaccination, all subjects were seroprotected against diphtheria (≥ 0.01 IU/mL), tetanus (≥ 0.01 IU/mL) and poliovirus types 1 and 3 (≥ 8 (1/dilution)); 97.3% of subjects were seroprotected against poliovirus type 2 (≥ 8 (1/dilution)); 94.6% of subjects were seroprotected against hepatitis B (≥ 10 IU/mL) and 88.0% were seroprotected against Hib invasive diseases (≥ 0.15 μg/mL).
One month after the booster dose, all subjects were seroprotected against diphtheria (≥ 0.1 IU/mL), tetanus (≥ 0.1 IU/mL) and poliovirus types 1, 2 and 3 (≥ 8 (1/dilution)); 93.9% of subjects were seroprotected against hepatitis B (≥ 10 IU/mL) and 94.0% were seroprotected against Hib invasive diseases (≥ 1 μg/mL).
Regarding pertussis, one month after primary vaccination 99.4% and 100% of subjects developed antibodies ≥ 8 EU/mL against PT and FHA antigens, respectively. One month after the booster dose, 99.4% of subjects developed antibodies ≥ 8 EU/mL against both PT and FHA antigens. Pertussis antibody concentrations were increased by 5- to 9-fold after primary vaccination and by 8- to 19-fold after the booster dose.
Immune responses to Hexaxim in HIV-exposed infants: Immune responses to Hexaxim antigens in 51 HIV-exposed infants (9 infected and 42 uninfected) were evaluated following a 3-dose primary vaccination course at 6, 10, and 14 weeks of age, and a booster dose at 15 to 18 months of age.
One month after primary vaccination, all infants were seroprotected against diphtheria (≥ 0.01 IU/mL), tetanus (≥ 0.01 IU/mL), poliovirus types 1, 2, and 3 (≥ 8 (1/dilution), hepatitis B (≥ 10 IU/mL), and more than 97.6% for Hib invasive diseases (≥ 0.15 μg/mL).
One month after the booster dose, all subjects were seroprotected against diphtheria (≥ 0.1 IU/mL), tetanus (≥ 0.1 IU/mL), poliovirus types 1, 2 and 3 (≥ 8 (1/dilution), hepatitis B (≥ 10 IU/mL) and more than 96.6% for Hib invasive diseases (≥ 1 μg/mL).
Regarding pertussis, one month after primary vaccination, 100% of subjects developed antibodies ≥ 8 EU/mL against both PT and FHA antigens. One month after the booster dose, 100% of subjects developed antibodies ≥ 8 EU/mL against both PT and FHA antigens. Seroconversion rates defined as minimum 4-fold increase compared to pre-vaccination level (pre-dose 1) were 100% in the HIV-exposed and infected group for anti-PT and anti-FHA; and 96.6% for anti-PT and 89.7% for anti-FHA in the HIV-exposed and uninfected group.
Efficacy and effectiveness in protecting against pertussis: Vaccine efficacy of the acellular pertussis (aP) antigens contained in Hexaxim against the most severe WHO-defined typical pertussis (≥ 21 days of paroxysmal cough) is documented in a randomised double-blind study among infants with a 3 dose primary series using a DTaP vaccine in a highly endemic country (Senegal). The need for a toddler booster dose was seen in this study. The long term capability of the acellular pertussis (aP) antigens contained in Hexaxim to reduce pertussis incidence and control pertussis disease in the childhood has been demonstrated in a 10-year national pertussis surveillance on pertussis disease in Sweden with the pentavalent DTaP-IPV/Hib vaccine using a 3, 5, 12 months schedule. Results of long term follow-up demonstrated a dramatic reduction of the pertussis incidence following the second dose regardless of the vaccine used.
Effectiveness in protecting against Hib invasive disease: The vaccine effectiveness against Hib invasive disease of DTaP and Hib combination vaccines (pentavalent and hexavalent including vaccines containing the Hib antigen from Hexaxim) has been demonstrated in Germany via an extensive (over five years follow-up period) post-marketing surveillance study. The vaccine effectiveness was of 96.7% for the full primary series, and 98.5% for the booster dose (irrespective of priming).
Pharmacokinetics: No pharmacokinetic studies have been performed.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional repeat dose toxicity and local tolerance studies.
At the injection sites, chronic histological inflammatory changes were observed that are expected to have a slow recovery.