Each film-coated tablet contains 2 or 4 mg perampanel.
Excipients/Inactive Ingredients: Core: Lactose monohydrate, Low-substituted-hydroxypropyl cellulose, Povidone, Magnesium stearate.
Film coating: 2 mg tablet: OPADRY ORANGE (containing): Hypromellose 2910, Talc, Macrogol 8000, Titanium dioxide, Yellow ferric oxide, Red ferric oxide.
4 mg tablet: OPADRY RED (containing): Hypromellose 2910, Talc, Macrogol 8000, Titanium dioxide, Red ferric oxide.
Pharmacotherapeutic group: antiepileptics, other antiepileptics. ATC code: N03AX22.
Pharmacology: Pharmacodynamics: Mechanism of action: Fycompa is a first-in-class selective, non-competitive antagonist of the ionotropic α-amino-3-hydroxy-5-methyl-4-isoxazoleproprionic acid (AMPA) glutamate receptor on post-synaptic neurons. Glutamate is the primary excitatory neurotransmitter in the central nervous system and is implicated in a number of neurological disorders caused by neuronal overexcitation. Activation of AMPA receptors by glutamate is thought to be responsible for most fast excitatory synaptic transmission in the brain. In in vitro studies, Fycompa did not compete with AMPA for binding to the AMPA receptor, but Fycompa binding was displaced by noncompetitive AMPA receptor antagonists, indicating that Fycompa is a noncompetitive AMPA receptor antagonist. In vitro, Fycompa inhibited AMPA-induced (but not NMDA-induced) increase in intracellular calcium. In vivo, Fycompa significantly prolonged seizure latency in an AMPA-induced seizure model.
The precise mechanism by which Fycompa exerts its antiepileptic effects in humans remains to be fully elucidated.
Pharmacodynamic effects: A pharmacokinetic-pharmacodynamic (efficacy) analysis was performed based on the pooled data from the 3 efficacy trials for partial-onset seizures. In addition, a pharmacokinetic-pharmacodynamic (efficacy) analysis was performed in one efficacy trial for primary generalised tonic clonic seizures. In both analyses, Fycompa exposure is correlated with reduction in seizure frequency.
Psychomotor performance: Single and multiple doses of 8 mg and 12 mg impaired psychomotor performance in healthy volunteers in a dose-related manner. The effects of Fycompa on complex tasks such as driving ability were additive or supra-additive to the impairment effects of alcohol.
Psychomotor performance testing returned to baseline within 2 weeks of cessation of Fycompa dosing.
Cognitive function: In a healthy volunteer study to assess the effects of Fycompa on alertness, and memory using a standard battery of assessments, no effects of Fycompa were found following single and multiple doses of Fycompa up to 12 mg/day.
In a placebo controlled study conducted in adolescent patients, no significant changes in cognition relative to placebo as measured by Cognitive Drug Research (CDR) System Global Cognition Score were observed for Fycompa. In the open label extension, no significant changes were observed in global CDR system score after 52 weeks of Fycompa treatment (see Paediatric population as follows).
Alertness and mood: Levels of alertness (arousal) decreased in a dose-related manner in healthy subjects dosed with Fycompa from 4 to 12 mg/day. Mood deteriorated following dosing of 12 mg/day only; the changes in mood were small and reflected a general lowering of alertness. Multiple dosing of Fycompa 12 mg/day also enhanced the effects of alcohol on vigilance and alertness, and increased levels of anger, confusion and depression as assessed using the Profile of Mood State 5-point rating scale.
Cardiac electrophysiology: Fycompa did not prolong the QTc interval when administered in daily doses up to 12 mg/day, and did not have a dose-related or clinically important effect on QRS duration.
Clinical efficacy and safety: Partial Onset Seizures: The efficacy of Fycompa in partial-onset seizures was established in three adjunctive therapy 19 week, randomised, double-blind, placebo-controlled, multicentre trials in adult and adolescent patients. Subjects had partial-onset seizures with or without secondary generalisation and were not adequately controlled with one to three concomitant AEDs. During a 6-week baseline period, subjects were required to have more than five seizures with no seizure-free period exceeding 25 days. In these three trials, subjects had a mean duration of epilepsy of approximately 21.06 years. Between 85.3% and 89.1% of patients were taking two to three concomitant AEDs with or without concurrent vagal nerve stimulation.
Two studies (studies 304 and 305) compared doses of Fycompa 8 and 12 mg/day with placebo and the third study (study 306) compared doses of Fycompa 2, 4 and 8 mg/day with placebo. In all three trials, following a 6-week Baseline Phase to establish baseline seizure frequency prior to randomisation, subjects were randomised and titrated to the randomised dose. During the Titration Phase in all three trials, treatment was initiated at 2 mg/day and increased in weekly increments of 2 mg/day to the target dose. Subjects experiencing intolerable adverse events could remain on the same dose or have their dose decreased to the previously tolerated dose. In all three trials, the Titration Phase was followed by a Maintenance Phase that lasted 13 weeks, during which patients were to remain on a stable dose of Fycompa.
The pooled 50% responder rates were placebo 19%, 4 mg 29%, 8 mg 35% and 12 mg 35%. A statistically significant effect on the reduction in 28-day seizure frequency (Baseline to Treatment Phase) as compared to the placebo group was observed with Fycompa treatment at doses of 4 mg/day (Study 306), 8 mg/day (Studies 304, 305 and 306), and 12 mg/day (Studies 304 and 305). The 50% responder rates in the 4 mg, 8 mg and 12 mg groups were respectively 23.0%, 31.5%, and 30.0% in combination with enzyme inducing anti-epileptic medicinal products and were 33.3%, 46.5% and 50.0% when Fycompa was given in combination with non-enzyme-inducing anti-epileptic medicinal products. These studies show that once-daily administration of Fycompa at doses of 4 mg to 12 mg was significantly more efficacious than placebo as adjunctive treatment in this population.
Data from placebo-controlled studies demonstrate that improvement in seizure control is observed with a once-daily Fycompa dose of 4 mg and this benefit is enhanced as the dose is increased to 8 mg/day. No efficacy benefit was observed at the dose of 12 mg as compared to the dose of 8 mg in the overall population. Benefit at the dose of 12 mg was observed in some patients who tolerate the dose of 8 mg and when the clinical response to that dose was insufficient. A clinically meaningful reduction in seizure frequency relative to placebo was achieved as early as the second week of dosing when patients reached a daily dose of 4 mg.
1.7 to 5.8% of the patients on Fycompa in the clinical studies became seizure free during the 3 month maintenance period compared with 0% - 1.0% on placebo.
Open label extension study: Ninety-seven percent of the patients who completed the randomised trials in patients with partial onset seizures were enrolled in the open label extension study (n=1186). Patients from the randomised trial were converted to Fycompa over 16 weeks followed by a long term maintenance period (≥1 year). The mean average daily dose was 10.05 mg.
Primary Generalised Tonic-Clonic Seizures: Fycompa as adjunctive therapy in patients 12 years of age and older with idiopathic generalised epilepsy experiencing primary generalised tonic-clonic seizures was established in a multicenter, randomized, double-blind, placebo-controlled study (Study 332). Eligible patients on a stable dose of 1 to 3 AEDs experiencing at least 3 primary generalised tonic-clonic seizures during the 8-week baseline period were randomized to either Fycompa or placebo. The population included 164 patients (Fycompa N=82, placebo N=82). Patients were titrated over four weeks to a target dose of 8 mg per day or the highest tolerated dose and treated for an additional 13 weeks on the last dose level achieved at the end of the titration period. The total treatment period was 17 weeks. Study drug was given once per day.
The 50% primary generalised tonic-clonic seizures responder rate during the Maintenance Period was significantly higher in the Fycompa group (58.0%) than in the placebo group (35.8%), P=0.0059. The 50% responder rate was 22.2% in combination with enzyme inducing anti-epileptic medicinal products and was 69.4% when Fycompa was given in combination with non-enzyme-inducing anti-epileptic medicinal products. The number of Fycompa subjects taking enzyme inducing anti-epileptic medicinal products was small (n = 9). The median percent change in primary generalised tonic-clonic seizure frequency per 28 days during the Titration and Maintenance Periods (combined) relative to Prerandomization was greater with Fycompa (-76.5%) than with placebo (-38.4%), P<0.0001. During the 3 months maintenance period, 30.9% (25/81) of the patients on Fycompa in the clinical studies became free of PGTC seizures compared with 12.3% (10/81) on placebo.
Other subtypes of idiopathic generalized seizure: The efficacy and safety of Fycompa in patients with myoclonic seizures have not been established. The available data are insufficient to reach any conclusions.
The efficacy of Fycompa in the treatment of absence seizures has not been demonstrated.
In Study 332, in patients with PGTC seizures who also had concomitant myoclonic seizures, freedom from seizures was achieved in 16.7 % (4/24) on Fycompa compared to 13.0 % (3/23) in those on placebo. In patients with concomitant absence seizures, freedom from seizures was achieved in 22.2% (6/27) on Fycompa compared to 12.1% (4/33) on placebo. Freedom from all seizures was achieved in 23.5% (19/81) of patients on Fycompa compared to 4.9% (4/81) of patients on placebo.
Open label extension phase: Of the 140 subjects who completed the Study 332 114 subjects (81.4%) had entered the Extension phase. Patients from the randomised trial were converted to Fycompa over 6 weeks followed by a long term maintenance period (≥ 1 year). In the Extension Phase, 73.7% of subjects have a modal daily Fycompa dose of greater than 4 to 8 mg/day and 16.7% had a modal daily dose of greater than 8 to 12 mg/day. A decrease in PGTC seizure frequency of at least 50% was seen in 65.9% of subjects after 1 year of treatment during the Extension Phase (relative to their pre-Fycompa baseline seizure frequency). These data were consistent with those for percent change in seizure frequency and showed that the PGTC 50% responder rate was generally stable across time from about week 26 through the end of year 2. Similar results were seen when all seizures and absence vs. myoclonic seizures were evaluated over time.
Conversion to monotherapy: In a retrospective study of clinical practice, 51 patients with epilepsy who received Fycompa as adjunctive treatment converted to Fycompa monotherapy. The majority of these patients had a history of partial onset seizures. Of these, 14 patients (27%) reverted to adjunctive therapy in the following months. Thirty four (34) patients were followed up for at least 6 months and, of these, 24 patients (71%) remained on Fycompa monotherapy for at least 6 months. Ten (10) patients were followed up for at least 18 months and, of these, 3 patients (30%) remained on Fycompa monotherapy for at least 18 months.
Paediatric population: The European Medicines Agency has deferred the obligation to submit the results of studies with Fycompa in one or more subsets of the paediatric population in treatment-resistant epilepsies (localisation-related and age-related epilepsy syndromes) (see Dosage & Administration for information on adolescent use).
The three pivotal double-blind placebo-controlled phase 3 studies included 143 adolescents between the ages of 12 and 18. The results in these adolescents were similar to those seen in the adult population.
Study 332 included 22 adolescents between the ages of 12 and 18. The results in these adolescents were similar to those seen in the adult population.
A 19-week, randomised, double-blind, placebo-controlled study with an open-label extension phase (Study 235) was performed to assess the short-term effects on cognition of Fycompa (target dose range of 8 to 12 mg once daily) as adjunctive therapy in 133 (Fycompa n = 85, placebo n = 48) adolescent patients, ages 12 to less than 18 years old, with inadequately controlled partial-onset seizures. Cognitive function was assessed by the Cognitive Drug Research (CDR) System Global Cognition t-Score, which is a composite score derived from 5 domains testing Power of Attention, Continuity of Attention, Quality of Episodic Secondary Memory, Quality of Working Memory, and Speed of Memory. The mean change (SD) from baseline to end of double-blind treatment (19 weeks) in CDR System Global Cognition t-Score was 1.1 (7.14) in the placebo group and (minus) -1.0 (8.86) in the Fycompa group, with the difference between the treatment groups in LS means (95% CI) = (minus) -2.2 (-5.2, 0.8). There was no statistically significant difference between the treatment groups (p = 0.145). CDR System Global Cognition t-Scores for placebo and Fycompa were 41.2 (10.7) and 40.8 (13.0), respectively at the baseline. For patients with Fycompa in the open label extension (n = 112), the mean change (SD) from baseline to end of open-label treatment (52 weeks) in CDR System Global Cognition t-Score was (minus) -1.0 (9.91). This was not statistically significant (p = 0.96). After up to 52 weeks of treatment with Fycompa (n = 114), no effect on bone growth was observed. No effects on weight, height and sexual development were seen following up to 104 weeks of treatment (n = 114).
Pharmacokinetics: The pharmacokinetics of Fycompa have been studied in healthy adult subjects (age range 18 to 79), adults and adolescents with partial-onset seizures and primary generalised tonic-clonic seizures, adults with Parkinson's disease, adults with diabetic neuropathy, adults with multiple sclerosis, and subjects with hepatic impairment.
Absorption: Fycompa is readily absorbed after oral administration with no evidence of marked first-pass metabolism. Co-administration of Fycompa tablets with a high fat meal had no impact on the peak plasma exposure (Cmax) or total exposure (AUC0-inf) of Fycompa. The tmax was delayed by approximately 1 hour compared to that under fasted conditions.
Distribution: Data from in vitro studies indicate that Fycompa is approximately 95% bound to plasma proteins.
In vitro studies show that Fycompa is not a substrate or significant inhibitor of organic anion transporting polypeptides (OATP) 1B1 and 1B3, organic anion transporters (OAT) 1, 2, 3, and 4, organic cation transporters (OCT) 1, 2, and 3, and the efflux transporters P-glycoprotein and Breast Cancer Resistance Protein (BCRP).
Biotransformation: Fycompa is extensively metabolised via primary oxidation and sequential glucuronidation. The metabolism of Fycompa is mediated primarily by CYP3A based on clinical study results in healthy subjects administered radiolabeled Fycompa and supported by in vitro studies using recombinant human CYPs and human liver microsomes.
Following administration of radiolabeled Fycompa, only trace amounts of Fycompa metabolites were observed in plasma.
Elimination: Following administration of a radiolabeled Fycompa dose to either 8 healthy adults or elderly subjects, approximately 30% of recovered radioactivity was found in the urine and 70% in the faeces. In urine and faeces, recovered radioactivity was primarily composed of a mixture of oxidative and conjugated metabolites. In a population pharmacokinetic analysis of pooled data from 19 Phase 1 studies, the average t1/2 of Fycompa was 105 hours. When dosed in combination with the strong CYP3A inducer carbamazepine, the average t1/2 was 25 hours.
Linearity/non-linearity: In healthy subjects, plasma concentrations of Fycompa increased in direct proportion to administered doses over the range of 2 to 12 mg. In a population pharmacokinetic analysis of patients with partial-onset seizures receiving Fycompa up to 12 mg/day and patients with primary generalised tonic clonic seizures receiving Fycompa up to 8 mg/day in placebo-controlled clinical trials, a linear relationship was found between dose and Fycompa plasma concentrations.
Special populations: Hepatic impairment: The pharmacokinetics of Fycompa following a single 1 mg dose were evaluated in 12 subjects with mild and moderate hepatic impairment (Child-Pugh A and B, respectively) compared with 12 healthy, demographically matched subjects. The mean apparent clearance of unbound Fycompa in mildly impaired subjects was 188 ml/min vs. 338 ml/min in matched controls, and in moderately impaired subjects was 120 ml/min vs. 392 ml/min in matched controls. The t1/2 was longer in mildly impaired (306 h vs. 125 h) and moderately impaired (295 h vs. 139 h) subjects compared to matched healthy subjects.
Renal impairment: The pharmacokinetics of Fycompa have not been formally evaluated in patients with renal impairment. Fycompa is eliminated almost exclusively by metabolism followed by rapid excretion of metabolites; only trace amounts of Fycompa metabolites are observed in plasma. In a population pharmacokinetic analysis of patients with partial-onset seizures having creatinine clearances ranging from 39 to 160 mL/min and receiving Fycompa up to 12 mg/day in placebo-controlled clinical trials, Fycompa clearance was not influenced by creatinine clearance. In a population pharmacokinetic analysis of patients with primary generalised tonic-clonic seizures receiving Fycompa up to 8 mg/day in a placebo-controlled clinical study, Fycompa clearance was not influenced by baseline creatinine clearance.
Gender: In a population pharmacokinetic analysis of patients with partial-onset seizures receiving Fycompa up to 12 mg/day and patients with primary generalised tonic-clonic seizures receiving Fycompa up to 8 mg/day in placebo-controlled clinical trials, Fycompa clearance in females (0.54 l/h) was 18% lower than in males (0.66 l/h).
Elderly (65 years of age and above): In a population pharmacokinetic analysis of patients with partial-onset seizures (age range 12 to 74 years) and primary generalised tonic-clonic seizures (age range 12 to 58 years), and receiving Fycompa up to 8 or 12 mg/day in placebo-controlled clinical trials, no significant effect of age on Fycompa clearance was found. A dose adjustment in the elderly is not considered to be necessary (see Dosage & Administration).
Paediatric population: In a population pharmacokinetic analysis of the adolescent patients in the Phase 2 and 3 clinical studies, there were no notable differences between this population and the overall population.
Drug interaction studies: In vitro assessment of drug interactions: Drug metabolising enzyme inhibition: In human liver microsomes, Fycompa (30 μmol/l) had a weak inhibitory effect on CYP2C8 and UGT1A9 among major hepatic CYPs and UGTs.
Drug metabolising enzyme induction: Compared with positive controls (including phenobarbital, rifampicin), Fycompa was found to weakly induce CYP2B6 (30 μmol/l) and CYP3A4/5 (≥3 μmol/l) among major hepatic CYPs and UGTs in cultured human hepatocytes.
Toxicology: Preclinical safety data: Adverse reactions not observed in clinical studies, but seen in animals at exposure levels similar to clinical exposure levels and with possible relevance to clinical use were as follows: In the fertility study in rats, prolonged and irregular oestrous cycles were observed at the maximum tolerated dose (30 mg/kg) in females; however, these changes did not affect fertility and early embryonic development. There were no effects on male fertility.
The excretion into breast milk was measured in rats at 10 days post-partum. Levels peaked at one hour and were 3.65 times the levels in plasma.
In a pre- and postnatal development toxicity study in rats, abnormal delivery and nursing conditions were observed at maternally toxic doses, and the number of stillbirths was increased in offspring. Behavioural and reproductive development of the offspring was not affected, but some parameters of physical development showed some delay, which is probably secondary to the pharmacology-based CNS effects of Fycompa. The placental transfer was relatively low; 0.09% or less of administered dose was detected in the foetus.
Nonclinical data reveal that Fycompa was not genotoxic and had no carcinogenic potential. The administration of maximum tolerated doses to rats and monkeys resulted in pharmacologically-based CNS clinical signs and decreased terminal body weight. There were no changes directly attributable to Fycompa in clinical pathology or histopathology.
Fycompa is indicated for the adjunctive treatment of partial-onset seizures with or without secondarily generalised seizures in patients with epilepsy aged 12 years and older.
Fycompa is indicated for the adjunctive treatment of primary generalised tonic-clonic seizures in adult and adolescent patients from 12 years of age with idiopathic generalised epilepsy (see Pharmacology: Pharmacodynamics under Actions).
Posology: Adults and adolescents: Fycompa must be titrated, according to individual patient response, in order to optimise the balance between efficacy and tolerability.
Fycompa should be taken orally once daily at bedtime.
Partial-Onset Seizures: Fycompa at doses of 4 mg/day to 12 mg/day has been shown to be effective therapy in partial-onset seizures.
Treatment with Fycompa should be initiated with a dose of 2 mg/day. The dose may be increased based on clinical response and tolerability by increments of 2 mg (either weekly or every 2 weeks as per half-life considerations described as follows) to a maintenance dose of 4 mg/day to 8 mg/day. Depending upon individual clinical response and tolerability at a dose of 8 mg/day, the dose may be increased by increments of 2 mg/day to 12 mg/day. Patients who are taking concomitant medicinal products that do not shorten the half-life of Fycompa (see Interactions) should be titrated no more frequently than at 2-week intervals. Patients who are taking concomitant medicinal products that shorten the half-life of Fycompa (see Interactions) should be titrated no more frequently than at 1-week intervals.
Primary Generalised Tonic-Clonic Seizures: Fycompa at a dose up to 8 mg/day has been shown to be effective in primary generalised tonic-clonic seizures.
Treatment with Fycompa should be initiated at a dose of 2 mg/day. The dose may be increased based on clinical response and tolerability by increments of 2 mg (either weekly or every 2 weeks, as per half-life considerations described as follows) to a maintenance dose of up to 8 mg/day. Depending upon individual clinical response and tolerability at a dose of 8 mg/day, the dose may be increased up to 12 mg/day, which may be effective in some patients (see Precautions). Patients who are taking concomitant medicinal products that do not shorten the half-life of Fycompa (see Interactions) should be titrated no more frequently than at 2-week intervals. Patients who are taking concomitant medicinal products that shorten the half-life of Fycompa (see Interactions) should be titrated no more frequently than at 1-week intervals.
Withdrawal: It is recommended that discontinuation be undertaken gradually to minimise the potential for rebound seizures. However, due to its long half-life and subsequent slow decline in plasma concentrations, Fycompa can be discontinued abruptly if absolutely needed.
Missed doses: Single missed dose: As Fycompa has a long half-life, the patient should wait and take their next dose as scheduled.
If more than 1 dose has been missed, for a continuous period of less than 5 half-lives (3 weeks for patients not taking Fycompa metabolism-inducing anti-epileptic drugs (AED), 1 week for patients taking Fycompa metabolism-inducing AEDs (see Interactions)), consideration should be given to re-start treatment from the last dose level.
If a patient has discontinued Fycompa for a continuous period of more than 5 half-lives, it is recommended that initial dosing recommendations given previously should be followed.
Elderly (65 years of age and above): Clinical studies of Fycompa in epilepsy did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Analysis of safety information in 905 Fycompa-treated elderly subjects (in double-blind studies conducted in non-epilepsy indications) revealed no age-related differences in the safety profile. In combination with the lack of age-related difference in Fycompa exposure, the results indicate that dose-adjustment in the elderly is not required. Fycompa should be used with caution in elderly taking into account the drug interaction potential in polymedicated patients (see Precautions).
Renal impairment: Dose adjustment is not required in patients with mild renal impairment. Use in patients with moderate or severe renal impairment or patients undergoing haemodialysis is not recommended.
Hepatic impairment: Dose increases in patients with mild and moderate hepatic impairment should be based on clinical response and tolerability. For patients with mild or moderate hepatic impairment, dosing can be initiated at 2 mg. Patients should be up-titrated using 2 mg doses no faster than every 2 weeks based on tolerability and effectiveness.
Fycompa dosing for patients with mild and moderate impairment should not exceed 8 mg. Use in patients with severe hepatic impairment is not recommended.
Paediatric population: The safety and efficacy of Fycompa in children below 12 years of age have not been established yet. No data are available.
Method of administration: Fycompa should be taken as single oral dose at bedtime. It may be taken with or without food (see Pharmacology: Pharmacokinetics under Actions). The tablet should be swallowed whole with a glass of water. It should not be chewed, crushed or split. The tablets cannot be split accurately as there is no break line.
There have been post-marketing cases of intentional and accidental overdose in paediatric patients with doses of perampanel up to 36 mg and in adult patients with doses up to 300 mg. The adverse reactions observed included altered mental status, agitation, aggressive behaviour, coma and depressed level of consciousness. The patients recovered without sequelae.
There is no available specific antidote to the effects of Fycompa.
General supportive care of the patient is indicated including monitoring of vital signs and observation of the clinical status of the patient. In view of its long half-life, the effects caused by Fycompa could be prolonged. Because of low renal clearance special interventions such as forced diuresis, dialysis or haemoperfusion are unlikely to be of value.
Hypersensitivity to the active substance or to any of the excipients listed in Description.
Suicidal ideation: Suicidal ideation and behaviour have been reported in patients treated with anti-epileptic medicinal products in several indications. A meta-analysis of randomised placebo-controlled trials of anti-epileptic medicinal products has also shown a small increased risk of suicidal ideation and behaviour. The mechanism of this risk is not known and the available data do not exclude the possibility of an increased risk for Fycompa.
Therefore, patients should be monitored for signs of suicidal ideation and behaviours and appropriate treatment should be considered. Patients (and caregivers of patients) should be advised to seek medical advice should signs of suicidal ideation or behaviour emerge.
Severe cutaneous adverse reactions (SCARs): Severe cutaneous adverse reactions (SCARs) including drug reaction with eosinophilia and systemic symptoms (DRESS) and Stevens-Johnson Syndrome (SJS), which can be life-threatening or fatal, have been reported (frequency unknown; see Adverse Reactions) in association with Fycompa treatment.
At the time of prescription patients should be advised of the signs and symptoms and monitored closely for skin reactions. Symptoms of DRESS include typically, although not exclusively, fever, rash associated with other organ system involvement, lymphadenopathy, liver function tests abnormalities and eosinophilia. It is important to note that early manifestations of hypersensitivity, such as fever or lymphadenopathy, may be present even though rash is not evident.
Symptoms of SJS include typically although not exclusively, skin detachment (epidermal necrosis/blister) < 10%, erythematous skin (confluent), rapid progression, painful atypical target-like lesions and/or purpuric macules in wide dissemination or large erythema (confluent), bullous/erosive involvement of more than 2 mucous membranes.
If signs and symptoms suggestive of these reactions appear, Fycompa should be withdrawn immediately and an alternative treatment considered (as appropriate).
If the patient has developed a serious reaction such as SJS or DRESS with the use of perampanel, treatment with perampanel must not be restarted in this patient at any time.
Nervous system disorders: Fycompa may cause dizziness and somnolence and therefore may influence the ability to drive or use machines (see Effects on ability to drive and use machines as follows).
Hormonal contraceptives: At doses of 12 mg/day Fycompa may decrease the effectiveness of progestative-containing hormonal contraceptives; in this circumstance additional non-hormonal forms of contraception are recommended when using Fycompa (see Interactions and Use in Pregnancy & Lactation).
Falls: There appears to be an increased risk of falls, particularly in the elderly; the underlying reason is unclear.
Aggression: Aggressive and hostile behaviour has been reported in patients receiving Fycompa therapy. In Fycompa-treated patients in clinical trials, aggression, anger and irritability were reported more frequently at higher doses. Most of the reported events were either mild or moderate and patients recovered either spontaneously or with dose adjustment. However, thoughts of harming others, physical assault or threatening behaviour were observed in some patients (< 1% in Fycompa clinical studies). Patients and caregivers should be counselled to alert a healthcare professional immediately if significant changes in mood or patterns of behaviour are noted. The dosage of Fycompa should be reduced if such symptoms occur and should be discontinued immediately if symptoms are severe.
Abuse potential: Caution should be exercised in patients with a history of substance abuse and the patient should be monitored for symptoms of Fycompa abuse.
Concomitant CYP 3A inducing anti-epileptic medicinal products: Response rates after addition of Fycompa at fixed doses were less when patients received concomitant CYP3A enzyme-inducing anti-epileptic medicinal products (carbamazepine, phenytoin, oxcarbazepine) as compared to response rates in patient who received concomitant non-enzyme-inducing anti-epileptic medicinal products. Patients response should be monitored when they are switching from concomitant non-inducer anti-epileptic medicinal products to enzyme inducing medicinal products and vice versa. Depending upon individual clinical response and tolerability, the dose may be increased or decreased 2 mg at a time (see Dosage & Administration).
Other concomitant (non-anti-epileptic) cytochrome P450 inducing or inhibiting medicinal products: Patients should be closely monitored for tolerability and clinical response when adding or removing cytochrome P450 inducers or inhibitors, since Fycompa plasma levels can be decreased or increased; the dose of Fycompa may need to be adjusted accordingly.
Hepatotoxicity: Cases of hepatotoxicity (mainly hepatic enzyme increased) with perampanel in combination with other antiepileptic drugs have been reported. If hepatic enzymes elevation is observed, monitoring of liver function should be considered.
Excipients: Lactose intolerance: Fycompa tablets contain lactose, therefore patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Effects on ability to drive and use machines: Fycompa has moderate influence on the ability to drive and use machines.
Fycompa may cause dizziness and somnolence and, therefore, may influence the ability to drive or use machines. Patients are advised not to drive a vehicle, operate complex machinery or engage in other potentially hazardous activities until it is known whether Fycompa affects their ability to perform these tasks (see Nervous system disorders as previously mentioned and Interactions).
Women of childbearing potential and contraception in males and females: Fycompa is not recommended in women of childbearing potential not using contraception unless clearly necessary. Fycompa may decrease the effectiveness of progestative containing hormonal contraceptives. An additional non-hormonal form of contraception is, therefore recommended (see Precautions and Interactions).
Pregnancy: There are limited amounts of data (less than 300 pregnancy outcomes) from the use of Fycompa in pregnant women. Studies in animals did not indicate any teratogenic effects in rats or rabbits, but embryotoxicity was observed in rats at maternally toxic doses (see Pharmacology: Toxicology: Preclinical safety data under Actions). Fycompa is not recommended during pregnancy.
Breastfeeding: Studies in lactating rats have shown excretion of Fycompa and/or its metabolites in milk (for details see Pharmacology: Toxicology: Preclinical safety data under Actions). It is not known whether Fycompa is excreted in human milk. A risk to the newborns/infants cannot be excluded. A decision must be made whether to discontinue breastfeeding or to discontinue/abstain from Fycompa therapy taking into account the benefit of breastfeeding for the child and the benefit of therapy for the woman.
Fertility: In the fertility study in rats, prolonged and irregular oestrous cycles were observed at high-dose (30 mg/kg) in females; however, these changes did not affect the fertility and early embryonic development. There were no effects on male fertility (see Pharmacology: Toxicology: Preclinical safety data under Actions). The effect of Fycompa on human fertility has not been established.
Summary of safety profile: In all controlled and uncontrolled trials in patients with partial-onset seizures, 1,639 subjects have received Fycompa of whom 1,147 have been treated for 6 months and 703 for longer than 12 months.
In the controlled and uncontrolled trial in patients with primary generalised tonic-clonic seizures, 114 subjects have received Fycompa of whom 68 have been treated for 6 months and 36 for longer than 12 months.
Adverse reactions leading to discontinuation: In the controlled Phase 3 partial-onset seizures clinical trials, the rate of discontinuation as a result of an adverse reaction was 1.7%, 4.2% and 13.7% in patients randomised to receive Fycompa at the recommended doses of 4 mg, 8 mg and 12 mg/day, respectively, and 1.4% in patients randomised to receive placebo. The adverse reactions most commonly (≥1% in the total Fycompa group and greater than placebo) leading to discontinuation were dizziness and somnolence.
In the controlled Phase 3 primary generalised tonic-clonic seizures clinical trial, the rate of discontinuation as a result of an adverse reaction was 4.9% in patients randomized to receive Fycompa 8 mg, and 1.2% in patients randomized to receive placebo. The adverse reaction most commonly leading to discontinuation (≥2% in the Fycompa group and greater than placebo) was dizziness.
Post-marketing use: Severe cutaneous adverse reactions (SCARs) including drug reaction with eosinophilia and systemic symptoms (DRESS) have been reported in association with Fycompa treatment (see Precautions).
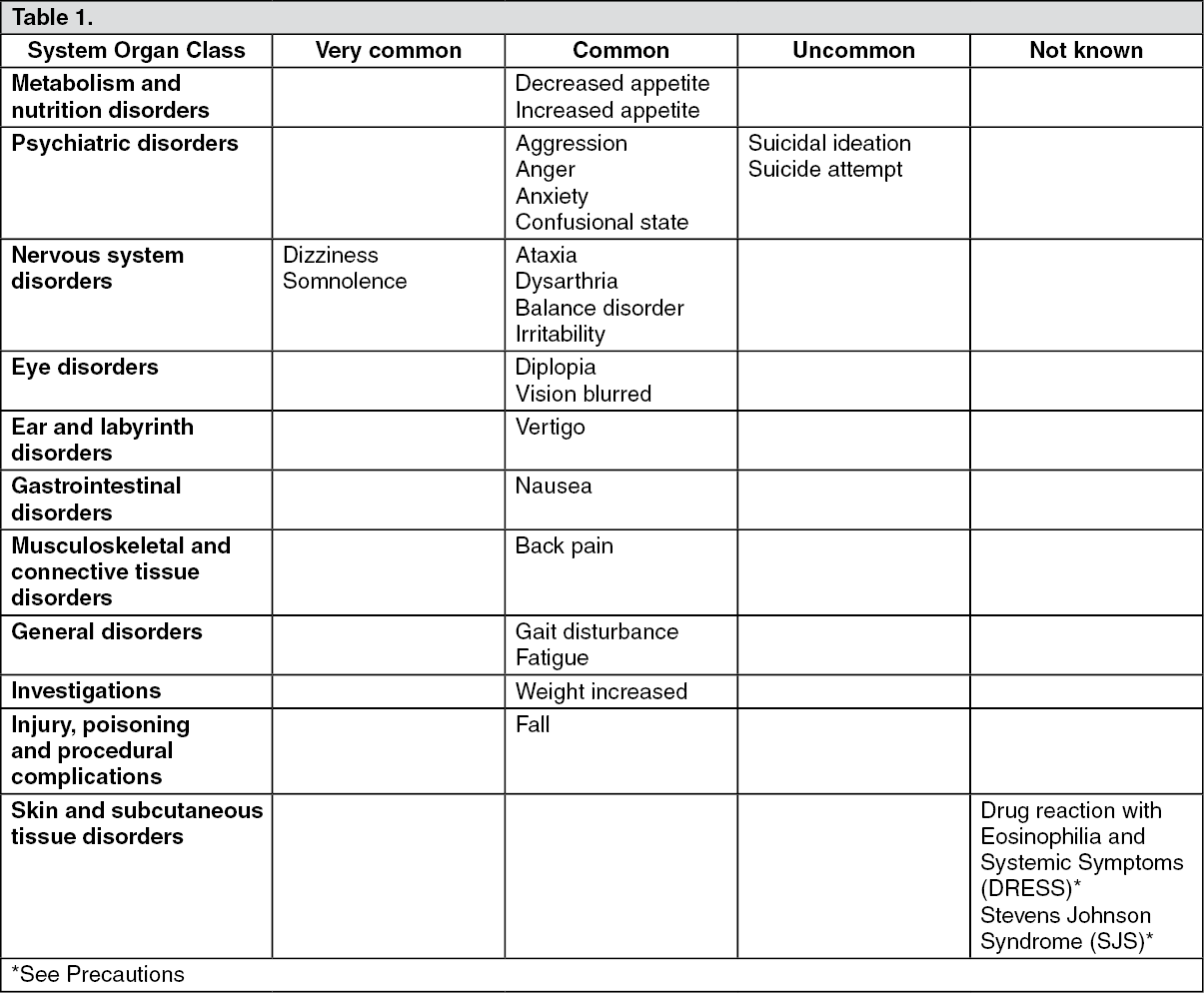
Tabulated list of adverse reactions: In the following table, adverse reactions, which were identified based on review of the full Fycompa clinical studies safety database, are listed by System Organ Class and frequency. The following convention has been used for the classification of adverse reactions: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), not known (cannot be estimated from the available data).
Within each frequency category, adverse reactions are presented in order of decreasing seriousness. (See Table 1.)
 Click on icon to see table/diagram/image
Paediatric population:
Click on icon to see table/diagram/image
Paediatric population: Based on the clinical trial database of 196 adolescents exposed to Fycompa from double-blind studies for partial onset seizures and primary generalized tonic-clonic seizures, the overall safety profile in adolescents was similar to that of adults, except for aggression, which was observed more frequently in adolescents than in adults.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system.
Fycompa is not considered a strong inducer or inhibitor of cytochrome P450 or UGT enzymes (see Pharmacology: Pharmacokinetics under Actions).
Hormonal contraceptives: In healthy women receiving 12 mg (but not 4 or 8 mg/day) for 21 days concomitantly with a combined oral contraceptive, Fycompa was shown to decrease the levonorgestrel exposure (mean Cmax and AUC values were each decreased by 40%). Ethinylestradiol AUC was not affected by Fycompa 12 mg whereas Cmax was decreased by 18%. Therefore, the possibility of decreased efficacy of hormonal progestative-containing contraceptives should be considered for women needing Fycompa 12 mg/day and an additional reliable method (intra-uterine device (IUD), condom) is to be used (see Precautions).
Interactions between Fycompa and other anti-epileptic medicinal products: Potential interactions between Fycompa (up to 12 mg once daily) and other anti-epileptic drugs (AEDs) were assessed in clinical studies and evaluated in the population PK analysis of four pooled Phase 3 studies including patients with partial-onset seizures and primary generalized tonic clonic seizures. The effect of these interactions on average steady state concentration is summarised in the following table. (See Table 2.)
Click on icon to see table/diagram/image
Some anti-epileptic drugs known as CYP450 3A enzyme inducers (carbamazepine, phenytoin, oxcarbazepine) have been shown to increase Fycompa clearance and consequently to decrease plasma concentrations of Fycompa. Conversely, withdrawal of a concomitant CYP450 3A enzyme inducer can be expected to increase plasma concentrations of Fycompa and dose reduction may be required.
Carbamazepine, a known potent enzyme inducer, reduced Fycompa levels by two-thirds in a study performed on healthy subjects.
A similar result was seen in a population pharmacokinetic analysis of patients with partial-onset seizures receiving Fycompa up to 12 mg/day and patients with primary generalised tonic-clonic seizures receiving Fycompa up to 8 mg/day in placebo-controlled clinical trials. The total clearance of Fycompa was increased when administered with carbamazepine (2.75-fold), phenytoin (1.7-fold) and oxcarbazepine (1.9-fold), which are known inducers of enzymes of metabolism (see Pharmacology: Pharmacokinetics under Actions). This effect should be taken into account and managed when adding or withdrawing these anti-epileptic drugs from a patient's treatment regimen.
In a population pharmacokinetic analysis of patients with partial-onset seizures receiving Fycompa up to 12 mg/day in placebo-controlled clinical trials, Fycompa did not affect to a clinically relevant manner the clearance of clonazepam, levetiracetam, phenobarbital, phenytoin, topiramate, zonisamide, carbamazepine, clobazam, lamotrigine and valproic acid, at the highest Fycompa dose evaluated (12 mg/day).
In the epilepsy population pharmacokinetic analysis, Fycompa was found to decrease the clearance of oxcarbazepine by 26%. Oxcarbazepine is rapidly metabolised by cytosolic reductase enzyme to the active metabolite, monohydroxycarbazepine. The effect of Fycompa on monohydroxycarbazepine concentrations is not known.
Fycompa is dosed to clinical effect regardless of other AEDs.
Effect of Fycompa on CYP3A substrates: In healthy subjects, Fycompa (6 mg once daily for 20 days) decreased midazolam AUC by 13%. A larger decrease in exposure of midazolam (or other sensitive CYP3A substrates) at higher Fycompa doses cannot be excluded.
Effect of cytochrome P450 inducers on Fycompa pharmacokinetics: Strong inducers of cytochrome P450, such as rifampicin and hypericum, are expected to decrease Fycompa concentrations and the potential for higher plasma concentrations of reactive metabolites in their presence has not been excluded. Felbamate has been shown to decrease the concentrations of some medicinal products and may also reduce Fycompa concentrations.
Effect of cytochrome P450 inhibitors on Fycompa pharmacokinetics: In healthy subjects, the CYP3A4 inhibitor ketoconazole (400 mg once daily for 10 days) increased Fycompa AUC by 20% and prolonged Fycompa half-life by 15% (67.8 h vs 58.4 h). Larger effects cannot be excluded when Fycompa is combined with a CYP3A inhibitor with longer half-life than ketoconazole or when the inhibitor is given for a longer treatment duration.
Levodopa: In healthy subjects, Fycompa (4 mg once daily for 19 days) had no effect on Cmax or AUC of levodopa.
Alcohol: The effects of Fycompa on tasks involving alertness and vigilance such as driving ability were additive or supra-additive to the effects of alcohol itself, as found in a pharmacodynamic interaction study in healthy subjects. Multiple dosing of Fycompa 12 mg/day increased levels of anger, confusion, and depression as assessed using the Profile of Mood State 5-point rating scale (see Pharmacology: Pharmacodynamics under Actions). These effects may also be seen when Fycompa is used in combination with other central nervous system (CNS) depressants.
Paediatric population: Interaction studies have only been performed in adults.
In a population, pharmacokinetic analysis of the adolescent patients in the Phase 3 clinical studies, there were no notable differences between this population and the overall population.
Incompatibilities: Not applicable.
Special precautions for disposal: No special requirements.
Do not store above 30°C.
Special precautions for storage: This medicinal product does not require any special storage conditions.
N03AX22 - perampanel ; Belongs to the class of other antiepileptics.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image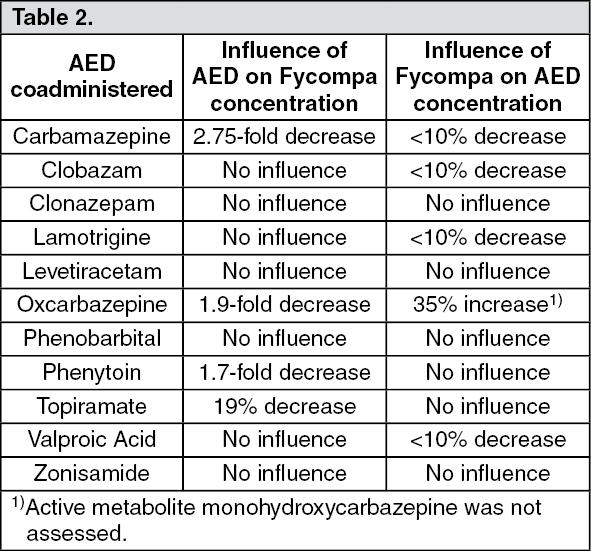 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
