


 Sign Out
Sign Out

Pharmacology: Mechanism of action (MOA): The elimination of estrogen-mediated stimulatory effects is a prerequisite for tumor response in cases where the growth of tumor tissue depends on the presence of estrogens. In postmenopausal women, estrogens are mainly derived from the action of the aromatase enzyme, which converts adrenal androgens - primarily androstenedione and testosterone - to estrone (E1) and estradiol (E2). The suppression of estrogen biosynthesis in peripheral tissues and the cancer tissue itself can therefore be achieved by specifically inhibiting the aromatase enzyme.
Letrozole is a non-steroidal aromatase inhibitor. It inhibits the aromatase enzyme by competitively binding to the hem of the cytochrome P450 subunit of the enzyme, resulting in a reduction of estrogen biosynthesis in all tissues.
Pharmacodynamics: In healthy postmenopausal women, single doses of 0.1 mg, 0.5 mg and 2.5 mg letrozole suppress serum estrone and estradiol by 75 to 78% and 78% from baseline, respectively. Maximum suppression is achieved in 48 to 78 hours.
In postmenopausal patients with advanced breast cancer, daily doses of 0.1 to 5 mg suppress plasma concentration of estradiol, estrone, and estrone sulphate by 75 to 95% from baseline in all patients treated. With doses of 0.5 mg and higher, many values of estrone and estrone sulphate are below the limit of detection in the assays, indicating that higher estrogen suppression is achieved with these doses. Estrogen suppression was maintained throughout treatment in all these patients.
Letrozole is highly specific in inhibiting aromatase activity. Impairment of adrenal steroidogenesis has not been observed. No clinically relevant changes were found in the plasma concentrations of cortisol, aldosterone, 11-deoxycortisol, 17-hydroxyprogesterone, and ACTH, or in plasma renin activity among postmenopausal patients treated with a daily dose of letrozole 0.1 to 5 mg. The ACTH stimulation test performed after 6 and 12 weeks of treatment with daily doses of 0.1 mg, 0.25 mg, 0.5 mg, 1 mg, 2.5 mg, and 5 mg did not indicate any attenuation of aldosterone or cortisol production. Thus, glucocorticoid and mineralocorticoid supplementation is not necessary.
No changes were noted in plasma concentrations of androgens (androstenedione and testosterone) among healthy postmenopausal women after 0.1 mg, 0.5 mg, and 2.5 mg single doses of letrozole or in plasma concentrations of androstenedione among postmenopausal patients treated with daily doses of 0.1 to 5 mg, indicating that the blockade of estrogen biosynthesis does not lead to accumulation of androgenic precursors. Plasma levels of LH and FSH are not affected by letrozole in patients, nor is thyroid function as evaluated by TSH, T4 and T3 uptake.
Clinical Studies: Adjuvant Treatment: Study BIG 1-98 (CFEM345 0019): BIG 1-98 was a multicenter, double-blind study in which over 8,000 postmenopausal women with hormone receptor-positive early breast cancer were randomized to one of the following treatments: A. tamoxifen for 5 years; B. Femara for 5 years; C. tamoxifen for 2 years followed by Femara for 3 years; D. Femara for 2 years followed by tamoxifen for 3 years.
The primary endpoint was disease-free survival (DFS); secondary efficacy endpoints were time to distant metastasis (TDM), distant disease-free survival (DDFS), overall survival (OS), systemic disease-free survival (SDFS), invasive contralateral breast cancer and time to breast cancer recurrence.
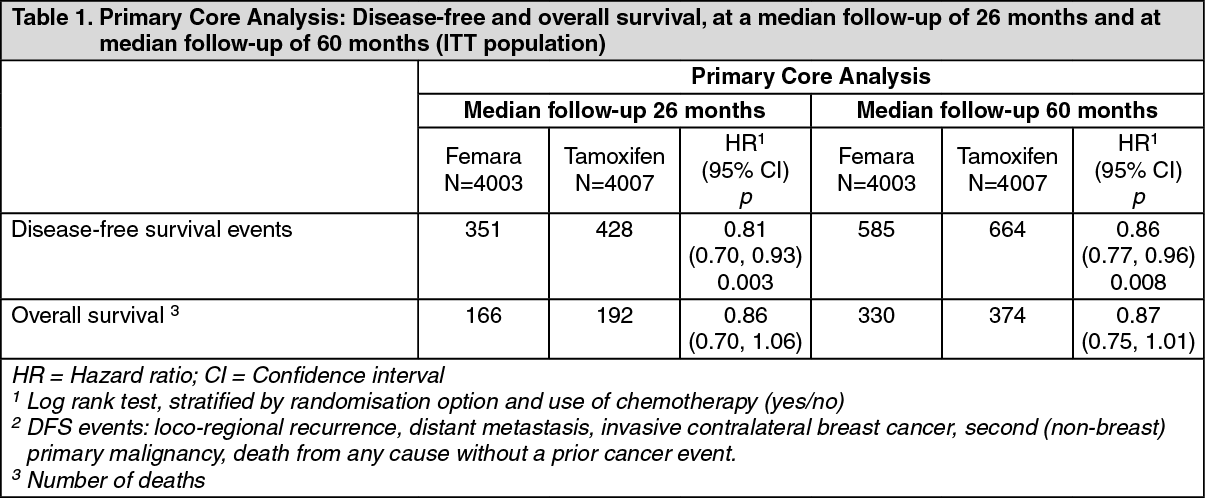
Efficacy results at a median follow-up of 26 and 60 months: Data in Table 1 reflect the results of the Primary Core Analysis based on data from the monotherapy arms (A and B) and from the two switching arms (C and D) at a median treatment duration of 24 months and a median follow-up of 26 months and at a median treatment duration of 32 months and a median follow-up of 60 months.
The 5-year DFS rates were 84% for Femara and 81.4% for tamoxifen. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageResults at a median follow-up of 96 months (monotherapy arms only): The Monotherapy Arms Analysis long-term update of the efficacy of Femara monotherapy compared to tamoxifen monotherapy (median duration of adjuvant treatment: 5 years) is presented in Table 2. (See Table 2).
 Click on icon to see table/diagram/image
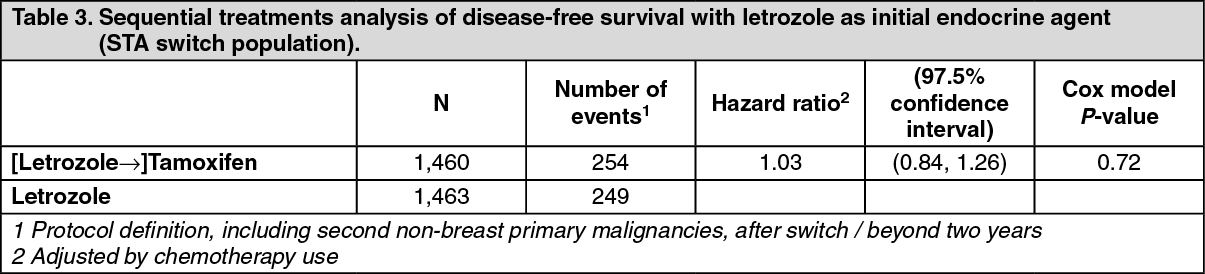
Click on icon to see table/diagram/imageSequential Treatments Analysis: The Sequential Treatments Analysis (STA) addresses the second primary question of BIG 1-98, namely whether sequencing of tamoxifen and letrozole would be superior to monotherapy. There were no significant differences in DFS, OS, SDFS, or DDFS from switch with respect to monotherapy (Table 3). (See Table 3).
 Click on icon to see table/diagram/image
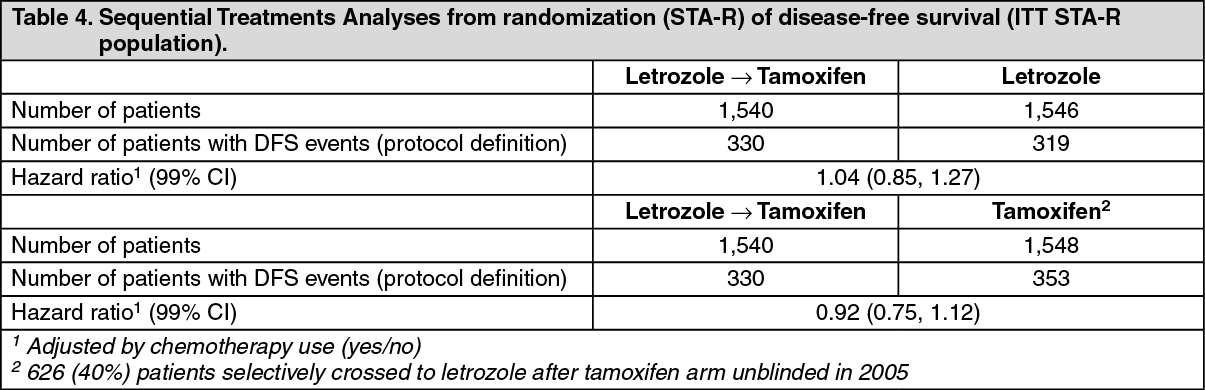
Click on icon to see table/diagram/imageThere were no significant differences in DFS, OS, SDFS or DDFS in any of the STA from randomization pairwise comparisons (Table 4). (See Table 4).
 Click on icon to see table/diagram/image
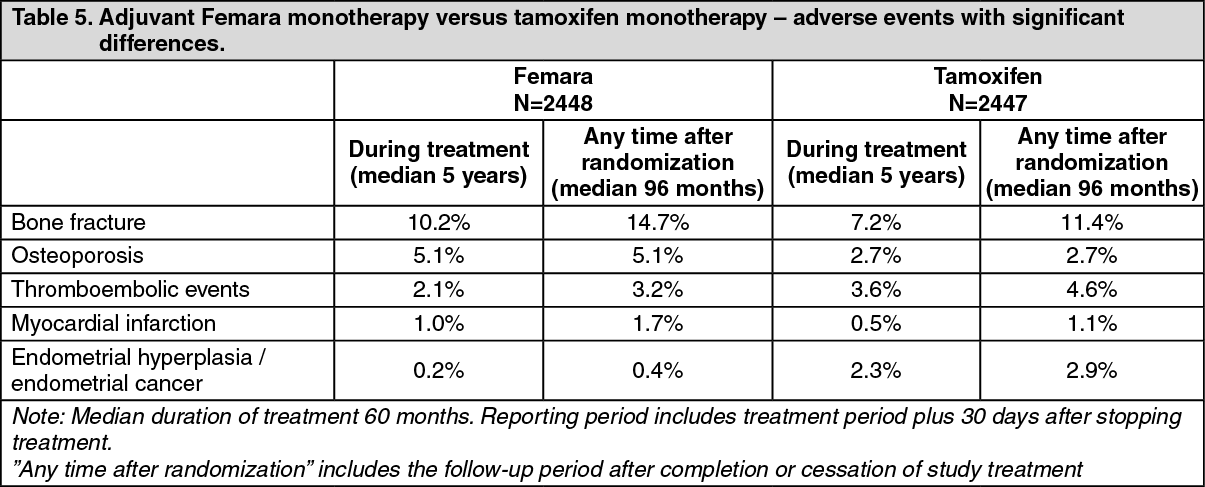
Click on icon to see table/diagram/imageThe following tables 5 and table 6 provide information on significant differences in Femara versus tamoxifen monotherapy and in the Femara-tamoxifen sequential treatment therapy: (See Tables 5 and 6).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image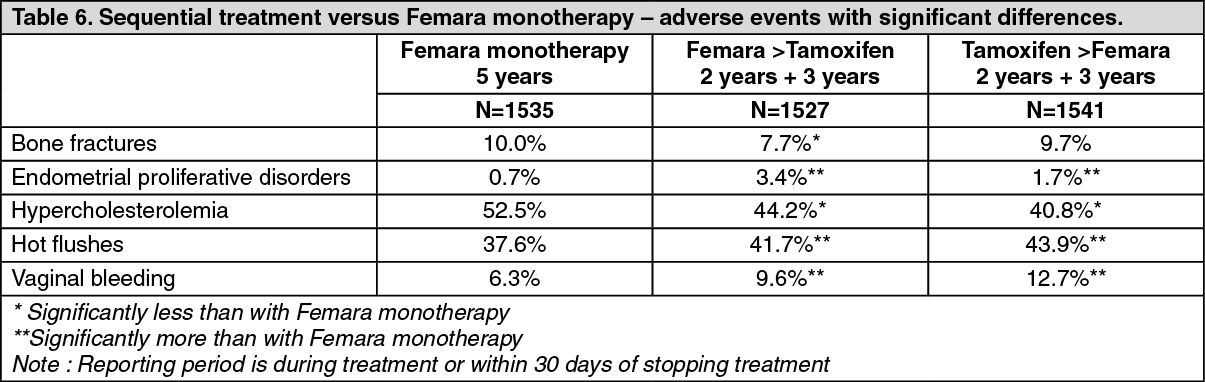 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageStudy CFEM345D2407: Study D2407 was an open-label, randomized, multicentre post-authorization safety study designed to compare the effects of adjuvant treatment with letrozole and tamoxifen on bone mineral density (BMD) and serum lipid profiles. In total, 263 patients were assigned either letrozole for 5 years (133 postmenopausal women) or tamoxifen for 2 years followed by letrozole for 3 years (130 patients). All evaluations of BMD and of serum lipids were conducted treatment-blinded in specialist central laboratories. The primary analysis of BMD and serum lipids was at 2 years.
There was a statistically significant difference between treatments at 2 years in the primary endpoint, lumbar spine (L2-L4) BMD with a median decrease of 4.1% in the letrozole arm compared to a median increase of 0.3% in the tamoxifen arm. The results for total hip BMD were similar to those for lumbar spine but less pronounced.
No patient with a normal BMD at baseline became osteoporotic during 5 years of treatment. One patient with osteopenia at baseline (T-score of -1.9) developed osteoporosis during the treatment period (assessment by central review).
Although treatment differences at the end of 5 years were attenuated such that there was no statistically significant difference between treatments in the protocol-defined clinically relevant BMD-related changes overall, there remained substantial differences in the effects of the two treatments on BMD and skeletal events. In patients with a normal T-score at baseline, significantly more patients in the letrozole arm than in the sequential treatment arm had reductions of at least 6% in lumbar spine BMD within 1 year or cumulative reductions of at least 8% over the entire treatment period. Although there was no significant difference overall between treatment arms in clinical fractures, three-quarters of the fractures in the sequential treatment arm occurred after the switch to letrozole. Both clinical fractures and impending fractures, however, tended to occur in patients whose skeletal status was compromised - i.e. patients with lower BMD T-scores at baseline, and patients with a history of fractures.
Total cholesterol levels (fasting) decreased by a median 16% in the tamoxifen arm at 6 months, and remained so for the duration of tamoxifen therapy. In the letrozole arm, total cholesterol levels were relatively stable throughout treatment. LDL cholesterol levels decreased in the tamoxifen arm but remained stable in the letrozole arm. Consequently, there were statistically significant differences in favour of tamoxifen in total cholesterol, LDL cholesterol and HDL: LDL ratio over the first 2 years of the study. There were no significant differences between treatments in triglycerides.
Extended adjuvant treatment: Study (MA-17) (CFEM345MA17): In a multicenter, double-blind, randomized, placebo-controlled study (MA-17), over 5,100 postmenopausal women with receptor-positive or unknown primary breast cancer who had completed adjuvant treatment with tamoxifen (4.5 to 6 years) were randomized to either Femara or placebo for 5 years.
The primary endpoint was disease-free survival, defined as the interval between randomization and the earliest occurrence of loco-regional recurrence, distant metastasis, or contralateral breast cancer.
The first planned interim analysis at a median follow-up of around 28 months (25% of patients being followed-up for at least 38 months), showed that Femara significantly reduced the risk of breast cancer recurrence by 42% compared with placebo (HR 0.58; 95% CI 0.45, 0.76; P=0.00003). The benefit in favor of letrozole was observed regardless of nodal status. There was no significant difference in overall survival: (Femara 51 deaths; placebo 62; HR 0.82; 95% CI 0.56, 1.19).
Consequently, after first interim analysis the study was unblinded and continued in an open-label fashion; patients in the placebo arm were allowed to switch to Femara for up to 5 years. Patients who opted not to switch were followed by observation only. Over 60% of eligible patients (disease-free at unblinding) opted to switch to Femara. The final analysis included 1,551 women who switched from placebo to Femara at a median of 31 months (range 12 to 106 months) after completion of tamoxifen adjuvant therapy. Median duration of Femara after switch was 40 months.
The final analysis conducted at a median follow-up of 62 months confirmed the significant reduction in the risk of breast cancer recurrence with Femara. (See Table 7).
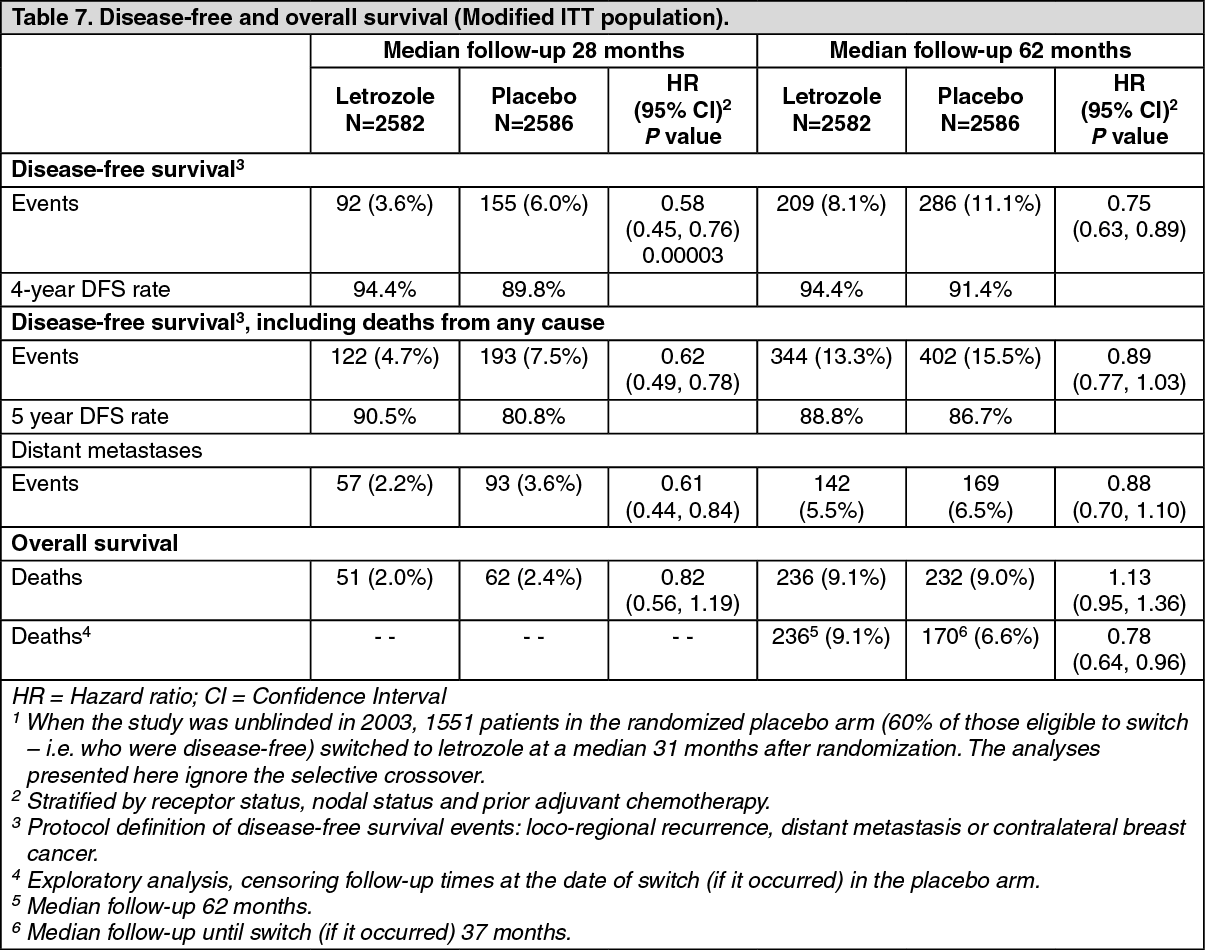 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the MA-17 bone substudy in which concomitant calcium and vitamin D were given, greater decreases in BMD compared to baseline occurred with Femara compared with placebo. The only statistically significant difference occurred at 2 years and was in total hip BMD (letrozole median decrease of 3.8% vs placebo median decrease of 2.0%).
In the MA-17 lipid substudy there were no significant differences between letrozole and placebo in total cholesterol or in any lipid fraction.
In the updated quality of life substudy there were no significant differences between treatments in physical component summary score or mental component summary score, or in any domain score in the SF-36 scale. In the MENQOL scale, significantly more women in the Femara arm than in the placebo arm were most bothered (generally in the first year of treatment) by those symptoms deriving from estrogen deprivation - hot flushes and vaginal dryness. The symptom that bothered most patients in both treatment arms was aching muscles, with a statistically significant difference in favor of placebo.
Pre-operative treatment: Study CFEM345E P024A: double blind trial (P024) was conducted in 337 postmenopausal breast cancer patients randomly allocated either Femara 2.5 mg for 4 months or tamoxifen for 4 months. At baseline all patients had tumors stage T2-T4c, N0-2, M0, ER and/or PgR positive and none of the patients would have qualified for breast-conserving surgery. Based on clinical assessment there were 55% objective responses in the Femara arm versus 36% for the tamoxifen arm (P<0.001). This finding was consistently confirmed by ultrasound (Femara 35% vs tamoxifen 25%, P=0.04) and mammography (Femara 34% vs tamoxifen 16%, P<0.001). In total 45% of patients in the Femara group versus 35% of patients in the tamoxifen group (P=0.02) underwent breast-conserving therapy). During the 4-month pre-operative treatment period, 12% of patients treated with Femara and 17% of patients treated with tamoxifen had disease progression on clinical assessment.
First-line treatment: Study CFEM345C P025: One controlled double-blind trial was conducted comparing Femara (letrozole) 2.5 mg to tamoxifen 20 mg as first-line therapy in postmenopausal women with advanced breast cancer. In 907 women, letrozole was superior to tamoxifen in time to progression (primary endpoint) and in overall objective response, time to treatment failure and clinical benefit.
The results are summarized in Table 8. (See Table 8).
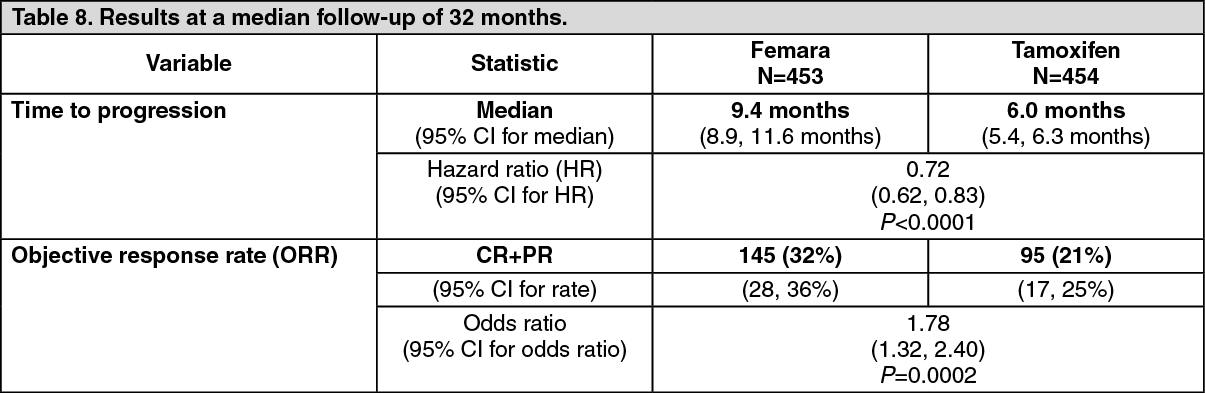 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTime to progression was significantly longer, and response rate significantly higher for letrozole irrespective of whether adjuvant anti-estrogen therapy had been given or not. Time to progression was significantly longer for letrozole irrespective of dominant site of disease. Median time to progression was 12.1 months for Femara and 6.4 months for tamoxifen in patients with soft tissue disease only and median 8.3 months for Femara and 4.6 months for tamoxifen in patients with visceral metastases.
Study design allowed patients to cross over upon progression to the other therapy or discontinue from the study. Approximately 50% of patients crossed over to the opposite treatment arm and crossover was virtually completed by 36 months. The median time to crossover was 17 months (Femara to tamoxifen) and 13 months (tamoxifen to Femara).
Femara treatment in the first-line therapy of advanced breast cancer resulted in a median overall survival of 34 months compared with 30 months for tamoxifen (logrank test P=0.53, not significant). The absence of an advantage for Femara on overall survival could be explained by the crossover design of the study.
Second-line treatment: Two well-controlled clinical trials were conducted comparing two letrozole doses (0.5 mg and 2.5 mg) to megestrol acetate and to aminoglutethimide, respectively, in postmenopausal women with advanced breast cancer previously treated with anti-estrogens.
Study AR/BC2: Statistically significant differences were observed in favour of letrozole 2.5 mg compared to megestrol acetate in overall objective tumor response rate (24% vs 16%, P=0.04), and in time to treatment failure (P=0.04). Overall survival and time to progression was not significantly different between the 2 arms (P=0.2 and P=0.07, respectively).
Study AR/BC3: Letrozole 2.5 mg was statistically superior to aminoglutethimide 250 mg bd for time to progression (P=0.008), time to treatment failure (P=0.003) and overall survival (P=0.002). In this study, the response rate was not significantly different between letrozole 2.5 mg and aminoglutethimide (P=0.06).
Male breast cancer: Use of Femara in men with breast cancer has not been studied.
Pharmacokinetics: Absorption: Letrozole is rapidly and completely absorbed from the gastrointestinal tract (mean absolute bioavailability: 99.9%). Food slightly decreases the rate of absorption (median tmax: 1 hour fasted versus 2 hours fed; and mean Cmax: 129 ± 20.3 nmol/L fasted versus 98.7 ± 18.6 nmol/L fed), but the extent of absorption (AUC) is not changed. The minor effect on the absorption rate is not considered to be of clinical relevance, and therefore letrozole may be taken without regard to meal times.
Distribution: Plasma protein binding of letrozole is approximately 60%, mainly to albumin (55%). The concentration of letrozole in erythrocytes is about 80% of that in plasma. After administration of 2.5 mg 14C-labelled letrozole, approximately 82% of the radioactivity in plasma was unchanged compound. Systemic exposure to metabolites is therefore low. Letrozole is rapidly and extensively distributed to tissues. Its apparent volume of distribution at steady state is about 1.87 ± 0.47 L/kg.
Biotransformation/metabolism: Metabolic clearance to a pharmacologically inactive carbinol metabolite is the major elimination pathway of letrozole (CLm=2.1 L/h), but is relatively slow when compared to hepatic blood flow (about 90 L/h). The cytochrome P450 isoenzymes 3A4 and 2A6 were found to be capable of converting letrozole to this metabolite. Formation of minor unidentified metabolites, and direct renal and faecal excretion play only a minor role in the overall elimination of letrozole. Within 2 weeks after administration of 2.5 mg 14C-labelled letrozole to healthy postmenopausal volunteers, 88.2 ± 7.6% of the radioactivity was recovered in urine and 3.8 ± 0.9% in faeces. At least 75% of the radioactivity recovered in urine up to 216 hours (84.7 ± 7.8% of the dose) was attributed to the glucuronide of the carbinol metabolite, about 9% to two unidentified metabolites, and 6% to unchanged letrozole.
Elimination: The apparent terminal elimination half-life in plasma is between about 2 to 4 days. After daily administration of 2.5 mg, steady-state levels are reached within 2 to 6 weeks. Plasma concentrations at steady state are approximately 7 times higher than concentrations measured after a single dose of 2.5 mg, while they are 1.5 to 2 times higher than the steady-state values predicted from the concentrations measured after a single dose, indicating a slight non-linearity in the pharmacokinetics of letrozole upon daily administration of 2.5 mg. Since steady-state levels are maintained over time, it can be concluded that no continuous accumulation of letrozole occurs.
Linearity/non-linearity: The pharmacokinetics of letrozole were dose proportional after single oral doses up to 10 mg (dose range: 0.01 to 30 mg) and after daily doses up to 1.0 mg (dose range: 0.1 to 5 mg). After a 30 mg single oral dose there was a slightly dose over-proportional increase in AUC value. With daily doses of 2.5 and 5 mg the AUC values increased about 3.8 and 12 fold instead of 2.5 and 5 fold, respectively, when compared to the 1.0 mg/day dose. The recommended dose of 2.5 mg/day may thus be a borderline dose at which an onset of over-proportionality becomes apparent, whereas at 5 mg/day the over-proportionality is more pronounced. The dose over-proportionality is likely to be the result of a saturation of metabolic elimination processes. Steady levels were reached after 1 to 2 months at all dosage regimens tested (0.1-5.0 mg daily).
Special Populations: Elderly: Age had no effect on the pharmacokinetics of letrozole.
Renal Impairment: In a study involving 16 postmenopausal volunteers with varying degrees of renal function (24-hour creatinine clearance 9 to 116 mL/min), no effect on the pharmacokinetics systemic exposure of letrozole was found after a single dose of 2.5 mg. In addition to the previously mentioned study assessing the influence of renal impairment on letrozole, a covariate analysis was performed on the data of two pivotal studies (Study AR/BC2 and Study AR/BC3). Calculated creatinine clearance (CLcr) [Study AR/BC2 range: 19 to 187 mL/min; Study AR/BC3 range: 10 to 180 mL/min] showed no statistically significant association between letrozole plasma trough levels at steady-state (Cmin). Furthermore, data of Study AR/BC2 and Study AR/BC3 in second-line metastatic breast cancer showed no evidence of an adverse effect of letrozole on CLcr or an impairment of renal function.
Therefore, no dose adjustment is required for patients with renal impairment (CLcr ≥10 mL/min). Little information is available in patients with severe impairment of renal function (CLcr <10 mL/min).
Hepatic Impairment: In a similar study involving subjects with varying degrees of hepatic function, the mean AUC values of the volunteers with moderate hepatic impairment (Child-Pugh score B) was 37% higher than in normal subjects, but still within the range seen in subjects without impaired function. In a study comparing the pharmacokinetics of letrozole after a single oral dose in eight subjects with liver cirrhosis and severe hepatic impairment (Child-Pugh score C) to those in healthy volunteers (n=8), AUC and t½ increased by 95% and 187%, respectively. Breast cancer patients with severe hepatic impairment are thus expected to be exposed to higher levels of letrozole than patients without severe hepatic dysfunction. However, since in patients dosed at 5 or 10 mg/day no increase in toxicity was observed, a dose reduction in patients with severe hepatic impairment appears not to be warranted, although such patients should be kept under close supervision. In addition, in two well-controlled studies involving 359 patients with advanced breast cancer, no effect of renal impairment (calculated creatinine clearance: 20 to 50 mL/min) or hepatic dysfunction was found on the letrozole concentration.
Toxicology: Non-clinical Safety Data: In a variety of preclinical safety studies conducted in standard animal species, there was no evidence of systemic or target organ toxicity.
Letrozole showed a low degree of acute toxicity in rodents exposed to up to 2,000 mg/kg. In dogs, letrozole caused signs of moderate toxicity at 100 mg/kg.
In repeated-dose toxicity studies in rats and dogs up to 12 months, the main findings observed can be attributed to the pharmacological action of the compound. The no-adverse effect level was 0.3 mg/kg in both species.
Oral administration of letrozole to female rats resulted in decreases in mating and pregnancy ratios and increases in pre-implantation loss.
The pharmacological effects of letrozole resulted in skeletal, neuroendocrine and reproductive findings in a juvenile rat study. Bone growth and maturation were decreased from the lowest dose (0.003 mg/kg/day) in males and increased from the lowest dose (0.003 mg/kg) in females. Bone Mineral Density (BMD) was also decreased at that dose in females. In the same study, decreased fertility at all doses was accompanied by hypertrophy of the hypophysis, testicular changes which included a degeneration of the seminiferous tubular epithelium and atrophy of the female reproductive tract. With the exception of bone size in females and morphological changes in the testes, all effects were at least partially reversible.
Both in vitro and in vivo investigations on letrozole's mutagenic potential revealed no indications of any genotoxicity.
In a 104-week rat carcinogenicity study, no treatment-related tumors were noted in male rats. In female rats, a reduced incidence of benign and malignant mammary tumors at all the doses of letrozole was found.
In a 104-week mouse carcinogenicity study, no treatment-related tumors were noted in male mice. In female mice, a generally dose-related increase in the incidence of benign ovarian granulosa theca cell tumors was observed at all doses of letrozole tested. These tumors were considered to be related to the pharmacological inhibition of estrogen synthesis and may be due to increased LH resulting from the decrease in circulating estrogen.
Oral administration of letrozole to gravid Sprague-Dawley rats resulted in a slight increase in the incidence of fetal malformation (domed head and fused centrum/vertebrae) among the animals treated. Similar malformations were not seen in New Zealand White rabbits. However, it was not possible to show whether this was an indirect consequence of the pharmacological properties (inhibition of estrogen biosynthesis), or a direct effect of letrozole in its own right (see CONTRAINDICATIONS and USE IN PREGNANCY & LACTATION).
Preclinical observations were confined to those associated with the recognized pharmacological action, which is the only safety concern for human use derived from animal studies.