


 Sign Out
Sign Out

In Table 7, the following frequency categories for adverse drug reactions (ADRs) were calculated based on the Faslodex 500 mg treatment group in pooled safety analyses of studies that compared Faslodex 500 mg with Faslodex 250 mg [CONFIRM (Study D6997C00002), FINDER 1 (Study D6997C00004), FINDER 2 (Study D6997C00006), and NEWEST (Study D6997C00003) studies], or from FALCON (Study D699BC00001) alone that compared Faslodex 500 mg with anastrozole 1 mg. Where frequencies differ between the pooled safety analysis and FALCON, the highest frequency is presented. The frequencies in Table 7 were based on all reported events, regardless of the investigator assessment of causality. The median duration of fulvestrant 500 mg treatment across the pooled dataset (including the studies mentioned previously plus FALCON) was 6.5 months.
Tabulated list of adverse reactions: Adverse reactions listed as follows are classified according to frequency and System Organ Class (SOC). Frequency groupings are defined according to the following convention: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100). Within each frequency grouping adverse reactions are reported in order of decreasing seriousness. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: The descriptions included as follows are based on the safety analysis set of 228 patients who received at least one (1) dose of fulvestrant and 232 patients who received at least one (1) dose of anastrozole, respectively in the Phase 3 FALCON study.
Joint and musculoskeletal pain: In the FALCON study, the number of patients who reported an adverse reaction of joint and musculoskeletal pain was 65 (31.2%) and 48 (24.1%) for fulvestrant and anastrozole arms, respectively. Of the 65 patients in the Faslodex arm, 40% (26/65) of patients reported joint and musculoskeletal pain within the first month of treatment, and 66.2% (43/65) of patients within the first 3 months of treatment. No patients reported events that were CTCAE Grade ≥3 or that required a dose reduction, dose interruption, or discontinued treatment due to these adverse reactions.
Combination therapy with palbociclib: The overall safety profile of fulvestrant when used in combination with palbociclib is based on data from 517 patients with HR-positive, HER2-negative advanced or metastatic breast cancer in the randomised PALOMA3 study (see Pharmacology: Pharmacodynamics under Actions). The most common (≥20%) adverse reactions of any grade reported in patients receiving fulvestrant in combination with palbociclib were neutropenia, leukopenia, infections, fatigue, nausea, anaemia, stomatitis, diarrhoea, thrombocytopenia and vomiting. The most common (≥2%) Grade ≥3 adverse reactions were neutropenia, leukopenia, infections, anaemia, AST increased, thrombocytopenia, and fatigue.
Table 8 reports the adverse reactions from PALOMA3.
Median duration of exposure to fulvestrant was 11.2 months in the fulvestrant + palbociclib arm and 4.8 months in the fulvestrant + placebo arm. Median duration of exposure to palbociclib in the fulvestrant + palbociclib arm was 10.8 months. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNeutropenia: In patients receiving fulvestrant in combination with palbociclib in the PALOMA3 study, neutropenia of any grade was reported in 290 (84.1%) patients, with Grade 3 neutropenia being reported in 200 (58.0%) patients, and Grade 4 neutropenia being reported in 40 (11.6%) patients. In the fulvestrant + placebo arm (n=172), neutropenia of any grade was reported in 7 (4.1%) patients. There were no reports of Grade 3 and 4 neutropenia in the fulvestrant + placebo arm.
In patients receiving fulvestrant in combination with palbociclib, the median time to first episode of any grade neutropenia was 15 days (range: 13-512 days) and the median duration of Grade ≥3 neutropenia was 16 days. Febrile neutropenia has been reported in 3 (0.9%) patients receiving fulvestrant in combination with palbociclib.
Combination Therapy with Abemaciclib (MONARCH 2): The safety of Faslodex (500 mg) plus abemaciclib (150 mg twice daily) versus Faslodex plus placebo was evaluated in MONARCH 2. The data described as follows reflect exposure to Faslodex in 664 patients with HR-positive, HER2-negative advanced breast cancer who received at least one dose of Faslodex plus abemaciclib or placebo in MONARCH 2.
Median duration of treatment was 12 months for patients receiving Faslodex plus abemaciclib and 8 months for patients receiving Faslodex plus placebo.
Dose reductions due to an adverse reaction occurred in 43% of patients receiving Faslodex plus abemaciclib. Adverse reactions leading to dose reductions ≥5% of patients were diarrhea and neutropenia. Abemaciclib dose reduction due to diarrhea of any grade occurred in 19% of patients receiving Faslodex plus abemaciclib compared to 0.4% of patients receiving Faslodex plus placebo. Abemaciclib dose reductions due to neutropenia of any grade occurred in 10% of patients receiving Faslodex plus abemaciclib compared to no patients receiving Faslodex plus placebo.
Permanent study treatment discontinuation due to an adverse event was reported in 9% of patients receiving Faslodex plus abemaciclib and in 3% of patients receiving Faslodex plus placebo. Adverse reactions leading to permanent discontinuation for patients receiving Faslodex plus abemaciclib were infection (2%), diarrhea (1%), hepatotoxicity (1%), fatigue (0.7%), nausea (0.2%), abdominal pain (0.2%), acute kidney injury (0.2%), and cerebral infarction (0.2%).
Deaths during treatment or during the 30-day follow up, regardless of causality, were reported in 18 cases (4%) of Faslodex plus abemaciclib treated patients versus 10 cases (5%) of Faslodex plus placebo treated patients. Causes of death for patients receiving Faslodex plus abemaciclib included: 7 (2%) patient deaths due to underlying disease, 4 (0.9%) due to sepsis, 2 (0.5%) due to pneumonitis, 2 (0.5%) due to hepatotoxicity, and one (0.2%) due to cerebral infarction.
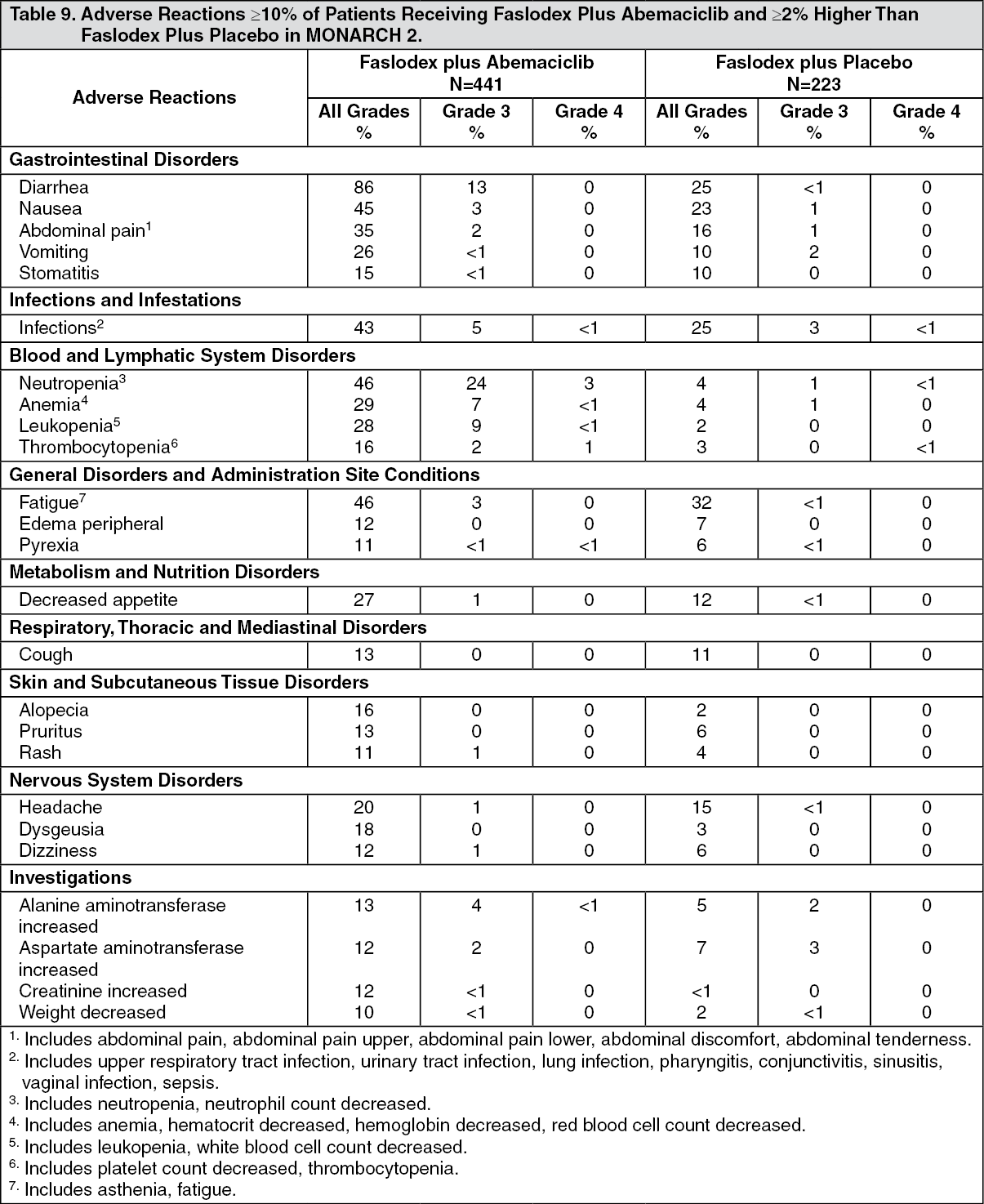
The most common adverse reactions reported (≥20%) in the Faslodex plus abemaciclib arm were diarrhea, fatigue, neutropenia, nausea, infections, abdominal pain, anemia, leukopenia, decreased appetite, vomiting, and headache (Table 9). The most frequently reported (≥5%) Grade 3 or 4 adverse reactions were neutropenia, diarrhea, leukopenia, anemia, and infections. (See Table 9.)
 Click on icon to see table/diagram/image
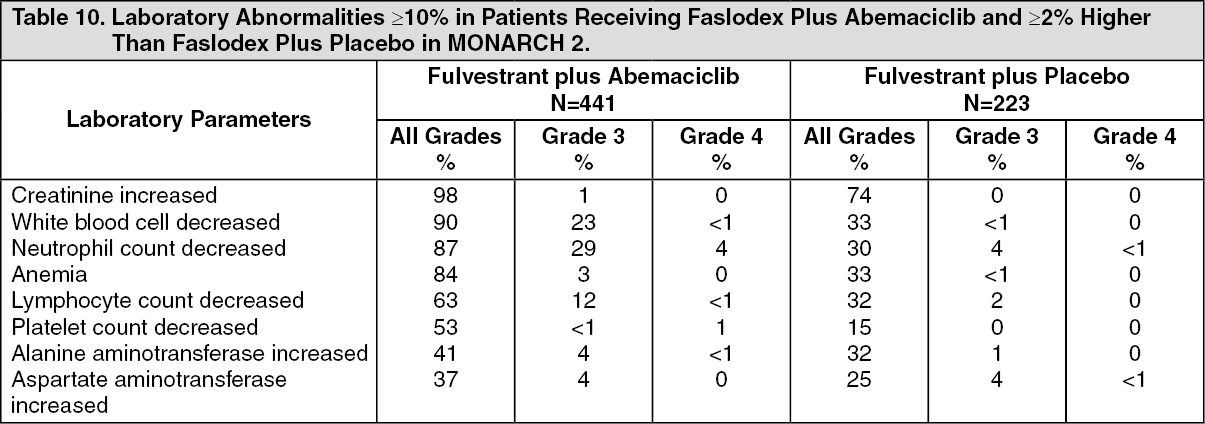
Click on icon to see table/diagram/imageAdditional adverse reactions in MONARCH 2 include venous thromboembolic events (deep vein thrombosis, pulmonary embolism, cerebral venous sinus thrombosis, subclavian vein thrombosis, axillary vein thrombosis, and DVT inferior vena cava), which were reported in 5% of patients treated with Faslodex plus abemaciclib as compared to 0.9% of patients treated with Faslodex plus placebo. (See Table 10.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCombination Therapy with Ribociclib (MONALEESA-3): The safety of Faslodex 500 mg plus ribociclib 600 mg versus Faslodex plus placebo was evaluated in MONALEESA-3. The data described as follows reflect exposure to Faslodex plus ribociclib in 483 out of 724 postmenopausal patients with HR-positive, HER2-negative advanced or metastatic breast cancer for initial endocrine based therapy or after disease progression on endocrine therapy who received at least one dose of Faslodex plus ribociclib or placebo in MONALEESA-3. Median duration of treatment was 15.8 months for Faslodex plus ribociclib and 12 months for Faslodex plus placebo.
Dose reductions due to adverse reactions occurred in 32% of patients receiving Faslodex plus ribociclib and in 3% of patients receiving Faslodex plus placebo. Among patients receiving Faslodex plus ribociclib, 8% were reported to have permanently discontinued both Faslodex plus ribociclib, and 9% were reported to have discontinued ribociclib alone due to ARs. Among patients receiving Faslodex plus placebo, 4% were reported to have permanently discontinued both Faslodex and placebo and 2% were reported to have discontinued placebo alone due to ARs.
Adverse reactions leading to treatment discontinuation of Faslodex plus ribociclib (as compared to Faslodex plus placebo) were ALT increased (5% vs. 0%), AST increased (3% vs. 0.6%), and vomiting (1% vs. 0%).
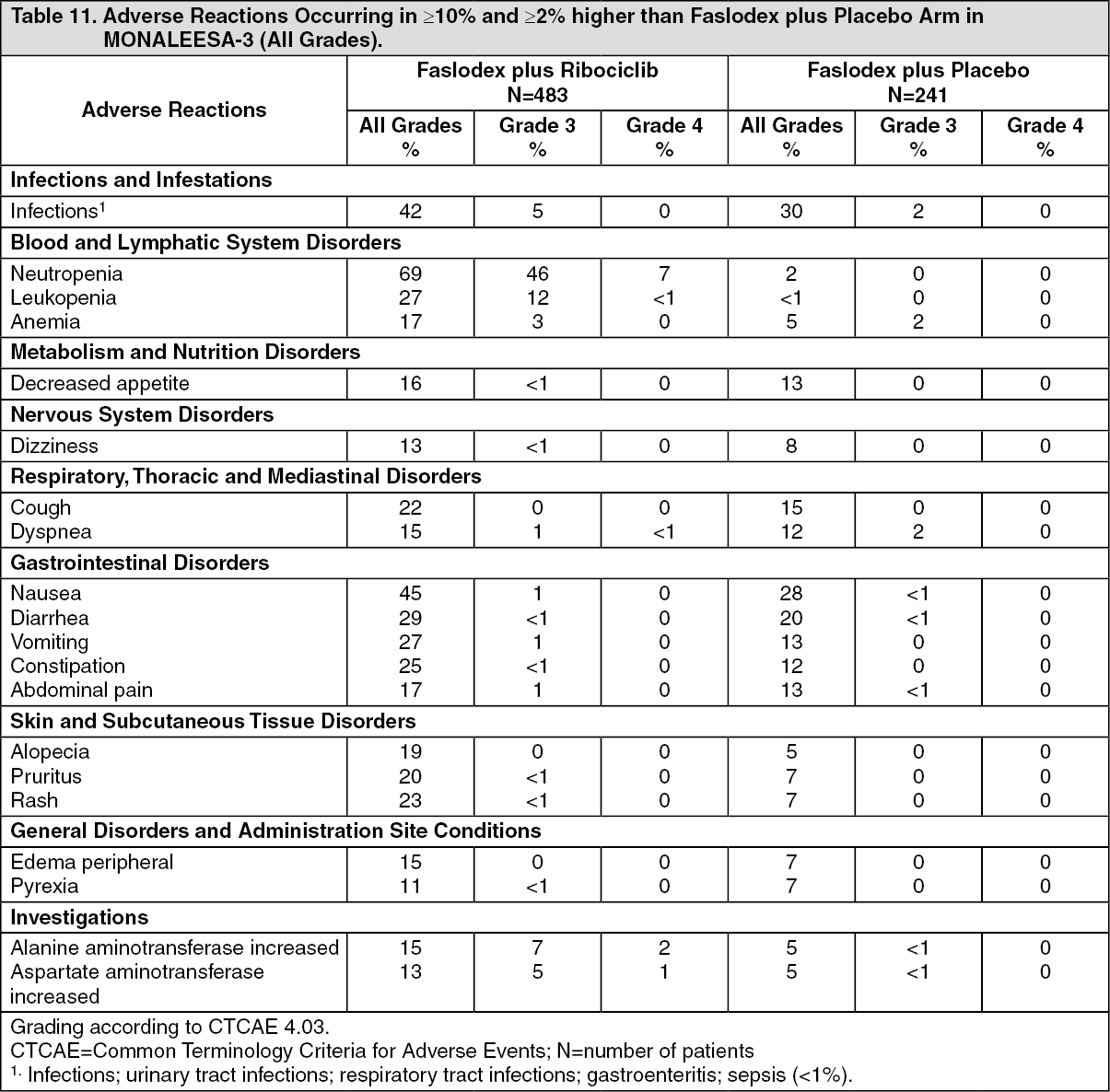
The most common adverse reactions (reported at a frequency ≥20% on the Faslodex plus ribociclib arm and ≥2% higher than Faslodex plus placebo) were neutropenia, infections, leukopenia, cough, nausea, diarrhea, vomiting, constipation, pruritus, and rash. The most frequently reported Grade 3/4 adverse reactions (reported at a frequency ≥5%) in patients receiving Faslodex plus ribociclib in descending frequency were neutropenia, leukopenia, infections, and abnormal liver function tests.
Adverse reactions and laboratory abnormalities occurring in patients in MONALEESA-3 are listed in Table 11 and Table 12, respectively. (See Table 11.)
 Click on icon to see table/diagram/image
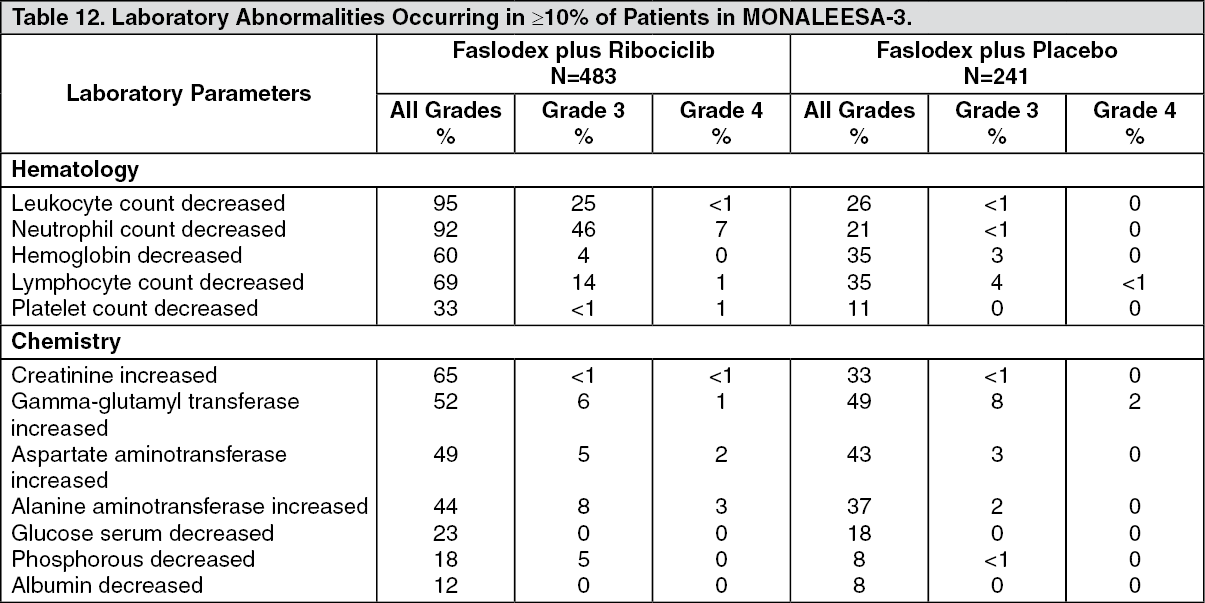
Click on icon to see table/diagram/imageAdditional adverse reactions in MONALEESA-3 for patients receiving Faslodex plus ribociclib included asthenia (14%), dyspepsia (10%), thrombocytopenia (9%), dry skin (8%), dysgeusia (7%), electrocardiogram QT prolonged (6%), dry mouth (5%), vertigo (5%), dry eye (5%), lacrimation increased (4%), erythema (4%), hypocalcemia (4%), blood bilirubin increased (1%), and syncope (1%). (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form