Pharmacotherapeutic group: Sex hormones and modulators of the genital system, progestogens and estrogens, fixed combination.
ATC code: G03AA13.
Pharmacology: Pharmacodynamics: Mechanism of action: EVRA acts through the mechanism of gonadotropin suppression by the estrogenic and progestational actions of ethinyl estradiol (EE) and norelgestromin (NGMN). The primary mechanism of action is inhibition of ovulation, but alterations to the cervical mucus, the fallopian tube motility and to the endometrium may also contribute to the efficacy of the product.
Receptor and sex hormone binding globulin (SHBG) binding studies, as well as studies in animals and humans, have shown that both norgestimate (NGM) and NGMN, the major serum metabolite of NGM following oral administration, exhibit high progestational activity with minimal intrinsic androgenicity, which illustrates the selective action of EVRA. Transdermally-administered norelgestromin in combination with EE does not counteract the estrogen-induced increases in SHBG, resulting in lower levels of free testosterone in serum compared to baseline.
The following non-contraceptive health benefits related to the use of combination hormonal contraceptives are supported by epidemiological studies which largely utilized hormonal contraceptive formulations containing estrogen at doses exceeding 35 micrograms of EE or 50 micrograms of mestranol.
Effects on menses: increased menstrual cycle regularity, decreased blood loss and decreased incidence of iron deficiency anemia, decreased incidence of dysmenorrhea.
Effects related to inhibition of ovulation: decreased incidence of functional ovarian cysts, decreased incidence of ectopic pregnancies.
Other effects: decreased incidence of fibroadenomas and fibrocystic disease of the breast, decreased incidence of acute pelvic inflammatory disease, decreased incidence of endometrial cancer, decreased incidence of ovarian cancer.
Pharmacodynamic effects: Clinical studies: Three contraceptive trials involving 4578 women for 31026 cycles were conducted worldwide. In these trials, 3319 women received EVRA and 1248 women received one of two oral contraceptives, one containing levonorgestrel/EE or one containing desogestrel/EE. The results of these trials showed that the efficacy of EVRA was similar to that of the oral contraceptives.
Exploratory analyses were performed to determine whether in the Phase III studies (n=3319) the population characteristics of age, race and weight were associated with pregnancy. The analyses indicated no association of age and race with pregnancy. With respect to weight, 5 of the 15 pregnancies reported with EVRA were among women with a baseline body weight ≥ 90 kg, which constituted < 3% of the study population. Below 90 kg there was no association between body weight and pregnancy. Although only 10-20% of the variability in pharmacokinetic data can be explained by weight (see Pharmacology: Pharmacokinetics: Effects on age, body weight, and body surface area as follows), the greater proportion of pregnancies among women at or above 90 kg was statistically significant and suggests that EVRA may be less effective in these women.
A multi-centre dose selection study for EVRA showed that EVRA inhibited ovulation to the same extent as the oral contraceptive comparator. The bleeding profile of EVRA in this study was similar to that of the oral contraceptive at all cycles. In addition, user compliance with EVRA dosing was significantly better than that seen with the oral contraceptive.
Among more than 3000 women who used EVRA for up to 13 cycles, the mean change in body weight from baseline to the end of treatment was an increase of 0.3 kg. In a 9-cycle placebo-controlled trial there was no difference between EVRA and placebo in the mean change in body weight from baseline to the end of treatment.
Pharmacokinetic studies with EVRA demonstrated consistent elimination kinetics for NGMN and EE with half-life of approximately 28 hours and 17 hours, respectively. One clinical trial assessed the return of hypothalamic-pituitary-ovarian axis function post-therapy and found that FSH, LH and estradiol mean values, though suppressed during therapy, returned to near baseline values during the 6 weeks post-therapy. Therefore, it is anticipated that following discontinuation of EVRA treatment, return to fertility will be rapid, approximating that seen with oral contraceptives.
Pharmacokinetics: Absorption: Following application of EVRA, both NGMN and EE rapidly appear in the serum, reach a plateau by approximately 48 hours, and are maintained at an approximate steady-state throughout the wear period. C
ss concentrations for NGMN and EE during one week of patch wear are approximately 0.8 ng/ml and 50 pg/ml, respectively, and are generally consistent from all studies and application sites.
The absorption of NGMN and EE following application of EVRA to the abdomen, buttock, upper outer arm and upper torso (excluding breast) was evaluated in a cross-over design study. The results of this study indicated that C
ss and AUC for the buttock, upper arm and torso for each analyte were equivalent. Strict bio-equivalence requirements for AUC were not met in this study for the abdomen. However, in a separate parallel group multiple application pharmacokinetic study, C
ss and AUC for the buttock and abdomen were not statistically different. In a dose-ranging study, EVRA caused effective ovulation suppression when applied to the abdomen. Therefore, all four sites are therapeutically equivalent.
The absorption of NGMN and EE following application of EVRA was studied under conditions encountered in a health club (sauna, whirlpool, treadmill and other aerobic exercises) and in a cold water bath. The results indicated that for NGMN there were no significant treatment effects on C
ss or AUC when compared to normal wear. For EE, slight increases were observed due to treadmill and other aerobic exercises. There was no significant effect of cool water on these parameters.
Results from a study with EVRA of extended wear of a single contraceptive patch for 7 days and 10 days indicated that target C
ss of NGMN and EE were maintained during a 3-day period of extended wear of EVRA (10 days). These findings suggest that clinical efficacy would be maintained even if a scheduled change is missed for as long as 2 full days.
Distribution: NGMN and norgestrel (a serum metabolite of NGMN) are highly bound (> 97%) to serum proteins. NGMN is bound to albumin and not to SHBG, while norgestrel is bound primarily to SHBG, which limits its biological activity. EE is extensively bound to serum albumin.
Metabolism: Since EVRA is applied transdermally, first-pass metabolism (via the gastrointestinal tract and/or liver) of NGMN and EE that would be expected following oral administration is avoided. Hepatic metabolism of NGMN occurs and metabolites include norgestrel, which is largely bound to SHBG, and various hydroxylated and conjugated metabolites. EE is also metabolized to various hydroxylated products and their glucuronide and sulfate conjugates.
Elimination: Following removal of patches, the elimination kinetics of NGMN and EE were consistent for all studies with half-life values of approximately 28 hours and 17 hours, respectively. The metabolites of NGMN and EE are eliminated by renal and fecal pathways.
Linearity/non-linearity: In multiple dose studies, C
ss and AUC for NGMN and EE were found to increase slightly over time when compared to Week 1 of Cycle 1. In a three-cycle study, these pharmacokinetic parameters reached steady-state conditions during all three weeks of Cycle 3. These observations are indicative of linear kinetics of NGMN and EE from EVRA use.
Transdermal versus oral contraceptives: The pharmacokinetic profiles of transdermal and oral combined hormonal contraceptives are different and caution should be exercised when making a direct comparison of these PK parameters.
In a study comparing EVRA to an oral contraceptive containing NGM 250 mcg/EE 35 mcg, C
max values were 2-fold higher for NGMN and EE in subjects administered the oral contraceptive compared to EVRA, while overall exposure (AUC and C
ss) was comparable in subjects treated with EVRA. Inter-subject variability (%CV) for the PK parameters following delivery from EVRA was higher relative to the variability determined from the oral contraceptive.
In a study comparing ORTHO EVRA (a transdermal patch with a similar PK profile to EVRA) to an oral contraceptive containing NGM 250 mcg/EE 35 mcg, overall exposure for NGMN and EE (AUC and C
ss) was higher in subjects treated with ORTHO EVRA for both Cycle 1 and Cycle 2 compared to that for the oral contraceptive, while C
max values were higher in subjects administered the oral contraceptive. Under steady-state conditions, AUC
0-168 and C
ss for EE were approximately 55% and 60% higher, respectively, for the transdermal patch, and the C
max was about 35% higher for the oral contraceptive. Inter-subject variability (%CV) for the PK parameters following delivery from ORTHO EVRA was higher relative to the variability determined from the oral contraceptive.
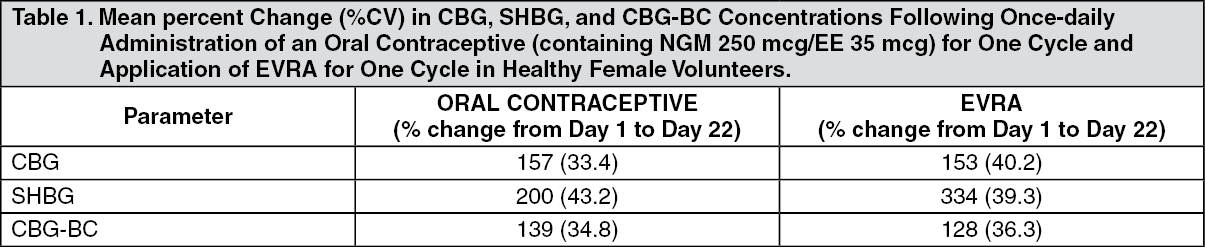
In the following table, percent change in concentrations (%CV) of markers of systemic estrogenic activity (Corticosteroid Binding Globulin [CBG], Sex Hormone Binding Globulin [SHBG], and Corticosteroid Binding Globulin-Binding Capacity [CBG-BC]) from Cycle 1, Day 1 to Cycle 1, Day 22 are presented. Overall, percent change in CBG and CBG-BC concentrations were similar for EVRA and oral contraceptive users; percent change in SHBG concentrations were higher for EVRA users compared to women taking the oral contraceptive. Within each group, the absolute values for CBG, SHBG, and CBG-BC were similar for Cycle 1, Day 22 and Cycle 2, Day 22. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Despite the differences in the PK profiles of EVRA and an oral contraceptive (containing NGM 250 mcg/EE 35 mcg), estrogenic activity, as assessed by hepatic globulin synthesis, was similar when evaluating CBG and CBG-BC and higher for EVRA when evaluating SHBG.
The clinical relevance of the difference in PK profile and pharmacodynamic (PD) response between transdermal and oral delivery is not known.
Effects of age, body weight, and body surface area: The effects of age, body weight, body surface area and race on the pharmacokinetics of NGMN and EE were evaluated in 230 healthy women from nine pharmacokinetic studies of single 7-day applications of EVRA. For both NGMN and EE, increasing age, body weight and body surface area each were associated with slight decreases in C
ss and AUC values. However, only a small fraction (10-20%) of the overall variability in the pharmacokinetics of NGMN and EE following application of EVRA may be associated with any or all of the previously mentioned demographic parameters. There was no significant effect of race with respect to Caucasians, Hispanics and Blacks.
Toxicology: Non-clinical Information: Preclinical data reveal no special hazard for humans based on conventional studies of safety, pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction. Studies conducted to examine the dermal effects of EVRA indicate this system has no potential to produce sensitization and results in only mild irritation when applied to rabbit skin.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
