


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Cetuximab is a chimeric monoclonal IgG1 antibody that is specifically directed against the epidermal growth factor receptor (EGFR).
EGFR signalling pathways are involved in the control of cell survival, cell cycle progression, angiogenesis, cell migration and cellular invasion/metastasis.
Cetuximab binds to the EGFR with an affinity that is approximately 5- to 10-fold higher than that of endogenous ligands. Cetuximab blocks binding of endogenous EGFR ligands resulting in inhibition of the function of the receptor. It further induces the internalisation of EGFR, which can lead to down-regulation of EGFR. Cetuximab also targets cytotoxic immune effector cells towards EGFR expressing tumour cells (antibody dependent cell-mediated cytotoxicity, ADCC).
Cetuximab does not bind to other receptors belonging to the HER family.
The protein product of the proto-oncogene RAS (rat sarcoma) is a central down-stream signal- transducer of EGFR. In tumours, activation of RAS by EGFR contributes to EGFR-mediated increased proliferation, survival and the production of pro-angiogenic factors.
RAS is one of the most frequently activated family of oncogenes in human cancers. Mutations of RAS genes at certain hot-spots on exons 2, 3 and 4 result in constitutive activation of RAS proteins independently of EGFR signalling.
Pharmacodynamic effects: In both in vitro and in vivo assays, cetuximab inhibits the proliferation and induces apoptosis of human tumour cells that express EGFR. In vitro cetuximab inhibits the production of angiogenic factors by tumour cells and blocks endothelial cell migration. In vivo cetuximab inhibits expression of angiogenic factors by tumour cells and causes a reduction in tumour neo-vascularisation and metastasis.
Immunogenicity: The development of human anti-chimeric antibodies (HACA) is a class effect of monoclonal chimeric antibodies. Current data on the development of HACAs is limited. Overall, measurable HACA titres were noted in 3.4% of the patients studied, with incidences ranging from 0% to 9.6% in the target indication studies. No conclusive data on the neutralising effect of HACAs on cetuximab is available to date. The appearance of HACA did not correlate with the occurrence of hypersensitivity reactions or any other undesirable effect to cetuximab.
Colorectal cancer: A diagnostic assay (EGFR pharmDx) was used for immunohistochemical detection of EGFR expression in tumour material. A tumour was considered to be EGFR-expressing, if one stained cell could be identified. Approximately 75% of the patients with metastatic colorectal cancer screened for clinical studies had an EGFR-expressing tumour and were therefore considered eligible for cetuximab treatment. The efficacy and safety of cetuximab have not been documented in patients with tumours where EGFR was not detected.
Study data demonstrate that patients with metastatic colorectal cancer and activating RAS mutations are highly unlikely to benefit from treatment with cetuximab or a combination of cetuximab and chemotherapy and as add-on to FOLFOX4 a significant negative effect on progression-free survival time (PFS) was shown.
Cetuximab as a single agent or in combination with chemotherapy was investigated in 5 randomised controlled clinical studies and several supportive studies. The 5 randomised studies investigated a total of 3734 patients with metastatic colorectal cancer, in whom EGFR expression was detectable and who had an ECOG performance status of ≤ 2. The majority of patients included had an ECOG performance status of ≤ 1. In all studies, cetuximab was administered as described in Dosage & Administration.
The KRAS exon 2 status was recognised as predictive factor for the treatment with cetuximab in 4 of the randomised controlled studies (EMR 62 202-013, EMR 62 202-047, CA225006, and CA225025). KRAS mutational status was available for 2072 patients. Further post-hoc analyses were performed for studies EMR 62 202-013 and EMR 62 202-047, where also mutations on RAS genes (NRAS and KRAS) other than KRAS exon 2 have been determined. Only in study EMR 62 202-007, a post-hoc analysis was not possible.
In addition, cetuximab was investigated in combination with chemotherapy in an investigator- initiated randomised controlled phase-III study (COIN, COntinuous chemotherapy plus cetuximab or INtermittent chemotherapy). In this study EGFR expression was not an inclusion criterion. Tumour samples from approximately 81% of patients were analysed retrospectively for KRAS expression.
FIRE-3, an investigator-sponsored clinical phase III study, compared the treatment of FOLFIRI in combination with either cetuximab or bevacizumab in the first-line treatment of patients with KRAS exon 2 wild-type mCRC. Further post-hoc analyses on mutations on RAS genes other than KRAS exon 2 have been evaluated.
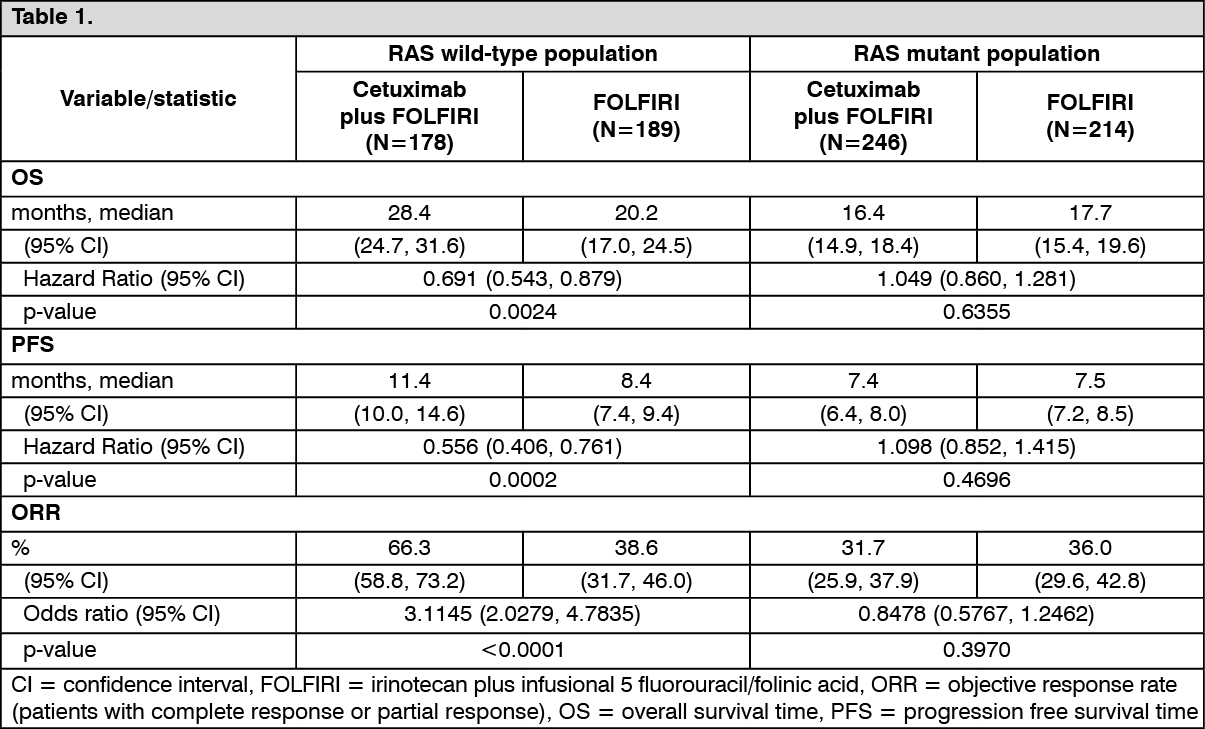
Cetuximab in combination with chemotherapy: EMR 62 202-013: This randomised study in patients with metastatic colorectal cancer who had not received prior treatment for metastatic disease compared the combination of cetuximab and irinotecan plus infusional 5-fluorouracil/folinic acid (FOLFIRI) (599 patients) to the same chemotherapy alone (599 patients). The proportion of patients with KRAS wild-type tumours from the patient population evaluable for KRAS status comprised 63%. For the assessment of the RAS status, mutations other than those on exon 2 of the KRAS gene were determined from all evaluable tumour samples within the KRAS exon 2 wild-type population. The RAS mutant population consists of patients with known KRAS exon 2 mutations as well as additionally identified RAS mutations.
The efficacy data generated in this study are summarised in the table as follows: (See Table 1).
 Click on icon to see table/diagram/image
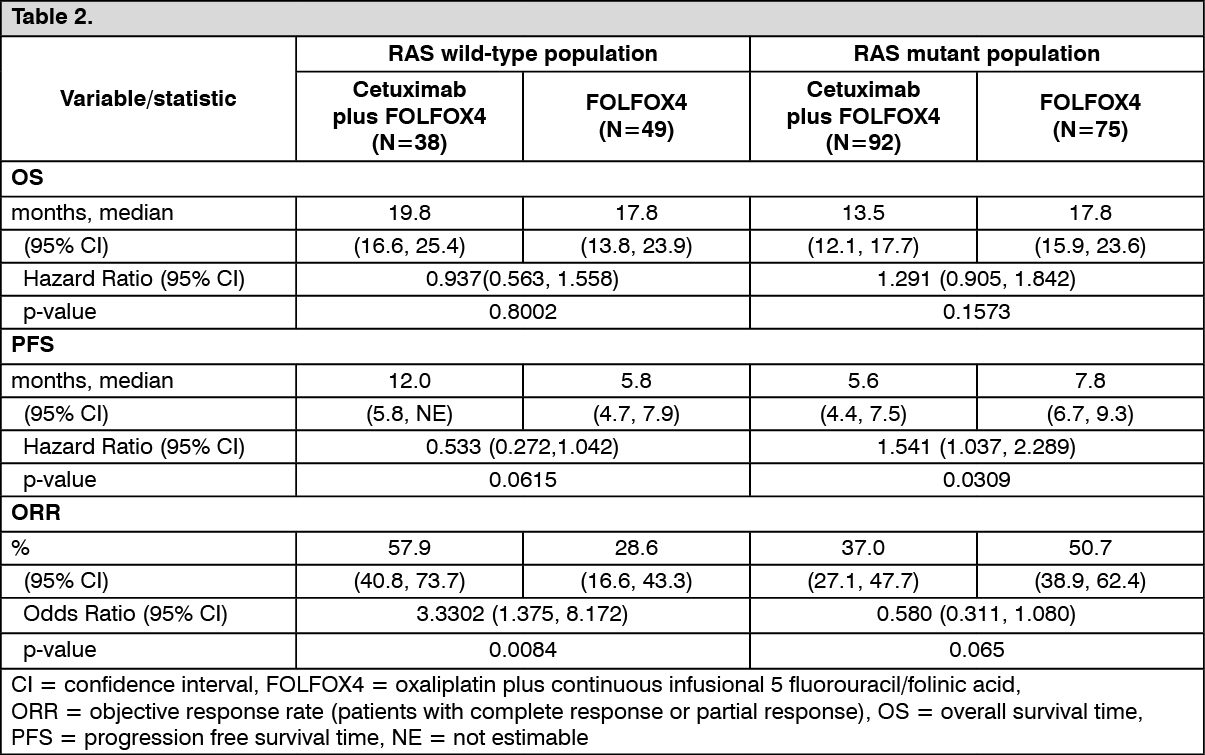
Click on icon to see table/diagram/imageEMR 62 202-047: This randomised study in patients with metastatic colorectal cancer who had not received prior treatment for metastatic disease compared the combination of cetuximab and oxaliplatin plus continuous infusional 5-fluorouracil/folinic acid (FOLFOX4) (169 patients) to the same chemotherapy alone (168 patients). The proportion of patients with KRAS wild-type tumours from the patient population evaluable for KRAS status comprised 57%. For the assessment of the RAS status, mutations other than those on exon 2 of the KRAS gene were determined from all evaluable tumour samples within the KRAS exon 2 wild-type population. The RAS mutant population consists of patients with known KRAS mutations as well as additionally identified RAS mutations.
The efficacy data generated in this study are summarised in the table as follows: (See Table 2).
 Click on icon to see table/diagram/image
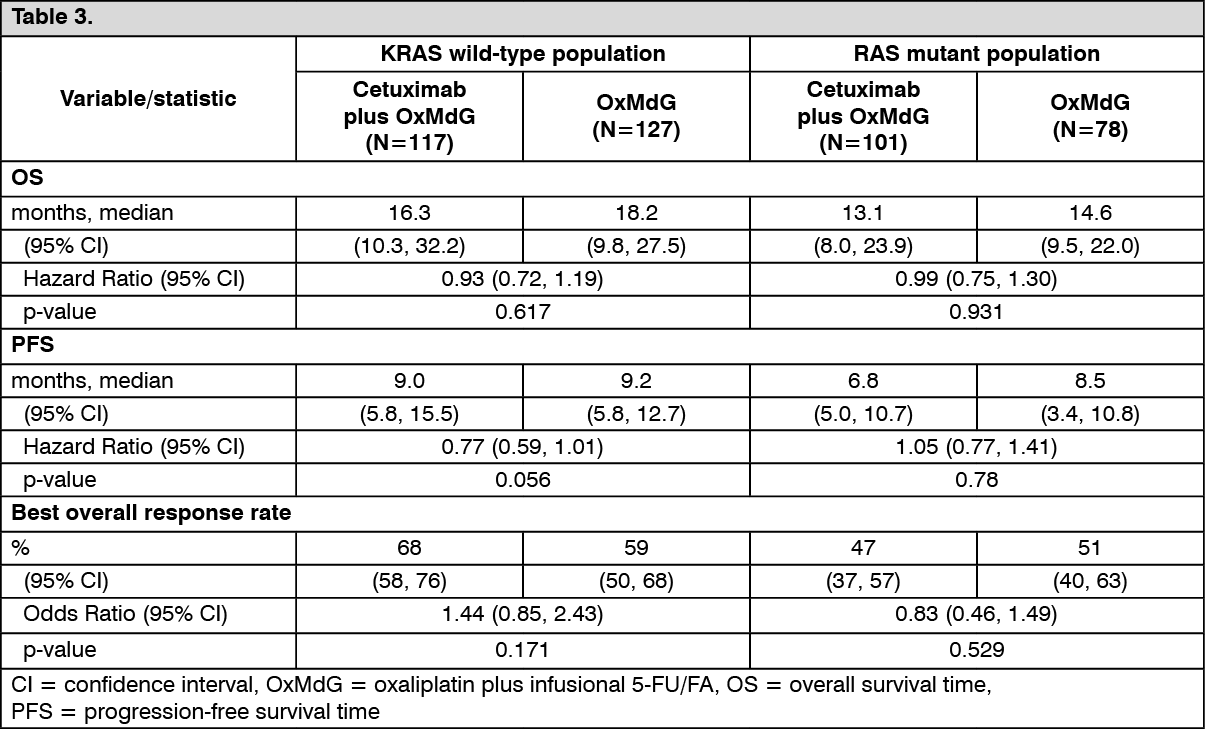
Click on icon to see table/diagram/imageIn particular a negative effect of cetuximab add-on in the RAS mutant population was observed. COIN: This was an open-label, 3-arm, randomised study in 2445 patients with inoperable metastatic or locoregional colorectal cancer who had not received prior treatment for metastatic disease and compared oxaliplatin plus fluoropyrimidines (infusional 5- fluorouracil/folinic acid [OxMdG] or capecitabine [XELOX]) in combination with cetuximab to the same chemotherapy regimen alone. The third experimental arm used an intermittent OxMdG or XELOX regimen without cetuximab. Data for the XELOX regimen and the third experimental arm are not presented.
Tumour samples from approximately 81% of patients were analysed retrospectively for KRAS expression, of which 55% were KRAS wild-type. Of these, 362 patients received cetuximab and oxaliplatin plus fluoropyrimidines (117 patients OxMdG and 245 patients XELOX) and 367 patients received oxaliplatin plus fluoropyrimidines alone (127 patients OxMdG and 240 patients XELOX). Of the KRAS mutant population, 297 patients received cetuximab and oxaliplatin plus fluoropyrimidines (101 patients OxMdG and 196 patients XELOX) and 268 patients received oxaliplatin plus fluoropyrimidines alone (78 patients OxMdG and 190 patients XELOX).
The efficacy data on the OxMdG regimen generated in this study are summarised in the table as follows: (See Table 3).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn time related endpoints no trends indicating clinical benefit could be shown for patients who received cetuximab in combination with the XELOX regimen.
There were significant dose reductions and delays of capecitabine or oxaliplatin administration mainly due to higher frequency of diarrhoea in the cetuximab containing arm. In addition, significantly fewer patients treated with cetuximab received second-line therapy.
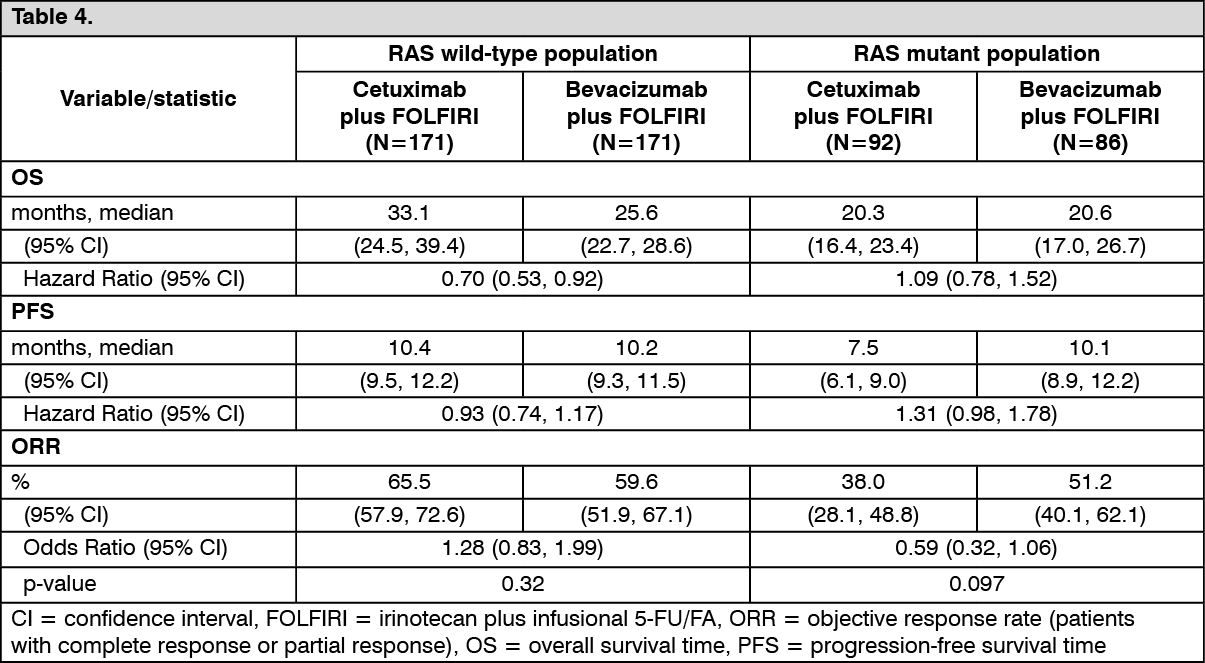
FIRE-3 (First-line combination of cetuximab with FOLFIRI): The FIRE-3 trial was a multicenter randomized phase III trial investigating head-to-head 5-FU, folinic acid and irinotecan (FOLFIRI) combined with either cetuximab or bevacizumab in patients with KRAS exon 2 wild- type metastatic colorectal cancer (mCRC). RAS status was evaluable in tumour samples of 407 KRAS exon 2 wild-type patients reflecting 69% of the overall KRAS exon 2 wildtype patient population (592 patients). Of these, 342 patients had RAS wild-type tumors while RAS mutations were identified in 65 patients. The RAS mutant population comprises these 65 patients together with 113 patients with KRAS exon 2 mutant tumors treated before study enrolment was restricted to patients with KRAS exon 2 wild-type mCRC.
The efficacy data generated in this study are summarised in the table as follows: (See Table 4).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the KRAS wild-type population of the CALGB/SWOG 80405 study (n=1137), superiority of cetuximab plus chemotherapy over bevacizumab plus chemotherapy was not shown based on an interim analysis. Analyses on the RAS wild-type population are required to appropriately evaluate this data.
CA225006: This randomised study in patients with metastatic colorectal cancer who had received initial combination treatment with oxaliplatin plus fluoropyrimidine for metastatic disease compared the combination of cetuximab and irinotecan (648 patients) with irinotecan alone (650 patients). Following disease progression, treatment with EGFR-targeting agents was initiated in 50% of patients in the irinotecan-alone arm.
In the overall population, irrespective of KRAS status, the results reported for cetuximab plus irinotecan (648 patients) vs irinotecan alone (650 patients) were: median overall survival time (OS) 10.71 vs 9.99 months (HR 0.98), median progression free survival time (PFS) 4.0 vs 2.6 months (HR 0.69), and objective response rate (ORR) 16.4% vs 4.2%.
With respect to the KRAS status, tumour samples were only available from 23% of the patients (300 of 1298). From the KRAS evaluated population 64% of the patients (192) had KRAS wild- type tumours and 108 patients KRAS mutations. On the basis of this data and since no independent review of imaging data was conducted, results in relation to mutation status are considered non-interpretable.
EMR 62 202-007: This randomised study in patients with metastatic colorectal cancer after failure of irinotecan-based treatment for metastatic disease as the last treatment before study entry compared the combination of cetuximab and irinotecan (218 patients) with cetuximab monotherapy (111 patients).
The combination of cetuximab with irinotecan compared to cetuximab alone reduced the overall risk of disease progression by 46% and significantly increased objective response rate. In the randomised trial, the improvement in overall survival time did not reach statistical significance; however, in the follow-up treatment, nearly 50% of the patients of the cetuximab alone arm received a combination of cetuximab and irinotecan after progression of disease, which may have influenced overall survival time.
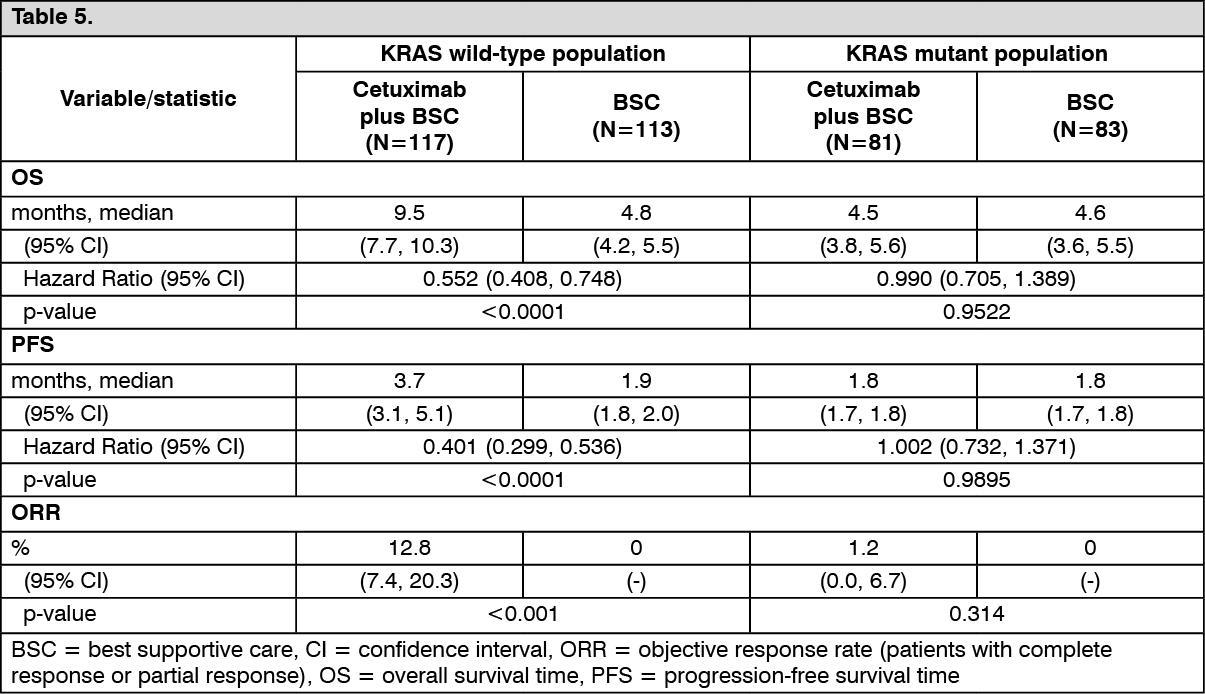
Cetuximab as a single agent: CA225025: This randomised study in patients with metastatic colorectal cancer who had received prior oxaliplatin-, irinotecan- and fluoropyrimidine-based treatment for metastatic disease compared the addition of cetuximab as a single agent to best supportive care (BSC) (287 patients) with best supportive care (285 patients). The proportion of patients with KRAS wild-type tumours from the patient population evaluable for KRAS status comprised 58%.
The efficacy data generated in this study are summarised in the table as follows: (See Table 5).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSquamous cell cancer of the head and neck: Immunohistochemical detection of EGFR expression was not performed since more than 90% of patients with squamous cell cancer of the head and neck have tumours that express EGFR.
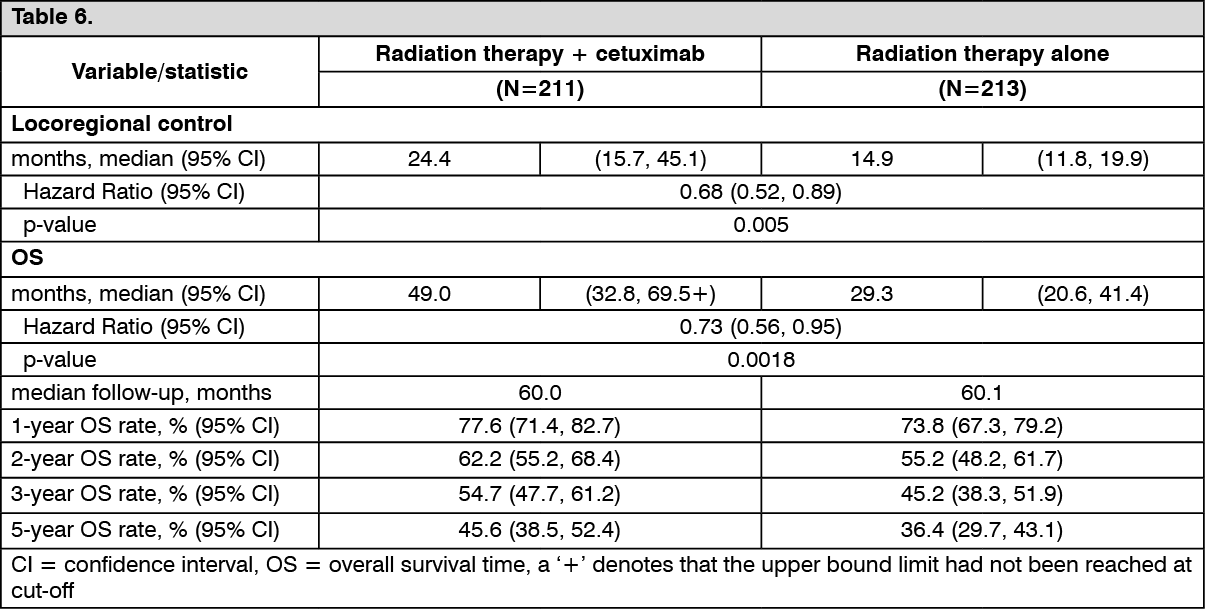
Cetuximab in combination with radiation therapy for locally advanced disease: EMR 62 202-006: This randomised study compared the combination of cetuximab and radiation therapy (211 patients) with radiation therapy alone (213 patients) in patients with locally advanced squamous cell cancer of the head and neck. Cetuximab was started one week before radiation therapy and administered at the doses described in Dosage & Administration until the end of the radiation therapy period.
The efficacy data generated in this study are summarised in the table as follows: (See Table 6).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePatients with a good prognosis as indicated by tumour stage, Karnofsky performance status (KPS) and age had a more pronounced benefit, when cetuximab was added to radiation therapy. No clinical benefit could be demonstrated in patients with KPS ≤ 80 who were 65 years of age or older.
The use of cetuximab in combination with chemo-radiotherapy has so far not been adequately investigated. Thus, a benefit-risk ratio for this combination has not yet been established.
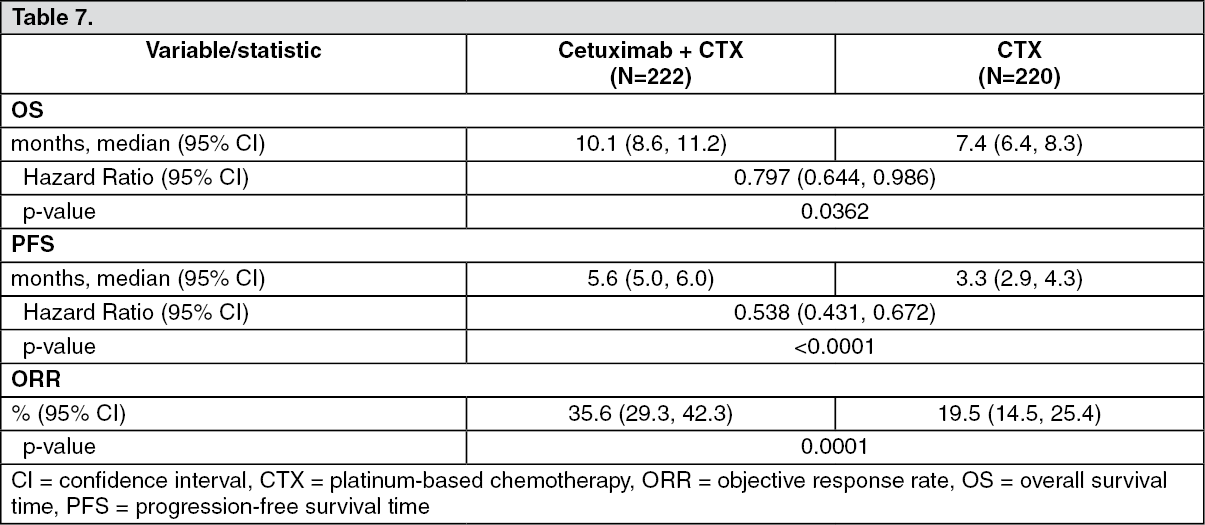
Cetuximab in combination with platinum-based chemotherapy in recurrent and/or metastatic disease: EMR 62 202-002: This randomised study in patients with recurrent and/or metastatic squamous cell cancer of the head and neck who had not received prior chemotherapy for this disease compared the combination of cetuximab and cisplatin or carboplatin plus infusional 5-fluorouracil (222 patients) to the same chemotherapy alone (220 patients). Treatment in the cetuximab arm consisted of up to 6 cycles of platinum-based chemotherapy in combination with cetuximab followed by cetuximab as maintenance therapy until disease progression.
The efficacy data generated in this study are summarised in the table as follows: (See Table 7).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePatients with a good prognosis as indicated by tumour stage, Karnofsky performance status (KPS) and age had a more pronounced benefit, when cetuximab was added to platinum-based chemotherapy. In contrast to progression free survival time, no benefit in overall survival time could be demonstrated in patients with KPS ≤ 80 who were 65 years of age or older.
Pharmacokinetics: Cetuximab pharmacokinetics were studied when cetuximab was administered as monotherapy or in combination with concomitant chemotherapy or radiation therapy in clinical studies. Intravenous infusions of cetuximab exhibited dose-dependent pharmacokinetics at weekly doses ranging from 5 to 500 mg/m2 body surface area.
When cetuximab was administered at an initial dose of 400 mg/m2 body surface area, the mean volume of distribution was approximately equivalent to the vascular space (2.9 l/m2 with a range of 1.5 to 6.2 l/m2). The mean Cmax (± standard deviation) was 185±55 microgram per ml. The mean clearance was 0.022 l/h per m2 body surface area. Cetuximab has a long elimination half-life with values ranging from 70 to 100 hours at the target dose.
Cetuximab serum concentrations reached stable levels after three weeks of cetuximab monotherapy. Mean peak cetuximab concentrations were 155.8 microgram per ml in week 3 and 151.6 microgram per ml in week 8, whereas the corresponding mean trough concentrations were 41.3 and 55.4 microgram per ml, respectively. In a study of cetuximab administered in combination with irinotecan, the mean cetuximab trough levels were 50.0 microgram per ml in week 12 and 49.4 microgram per ml in week 36.
Several pathways have been described that may contribute to the metabolism of antibodies. All of these pathways involve the biodegradation of the antibody to smaller molecules, i.e. small peptides or amino acids.
Pharmacokinetics in special populations: An integrated analysis across all clinical studies showed that the pharmacokinetic characteristics of cetuximab are not influenced by race, age, gender, renal or hepatic status.
Only patients with adequate renal and hepatic function have been investigated to date (serum creatinine ≤ 1.5 fold, transaminases ≤ 5 fold and bilirubin ≤ 1.5 fold the upper limit of normal).
Toxicology: Preclinical safety data: Dose-dependent skin alterations, starting at dose levels equivalent to those used in humans, were the major findings observed in toxicity studies with Cynomolgus monkeys (a chronic repeat-dose toxicity study and an embryo-foetal development study).
An embryo-foetal toxicity study in Cynomolgus monkeys revealed no signs of teratogenicity. However, dependent on the dose, an increased incidence of abortion was observed.
Non-clinical data on genotoxicity and local tolerance including accidental administration by routes other than the intended infusion revealed no special hazard for humans.
No formal animal studies have been performed to establish the carcinogenic potential of cetuximab or to determine its effects on male and female fertility.
Toxicity studies with co-administration of cetuximab and chemotherapeutic agents have not been performed.
No non-clinical data on the effect of cetuximab on wound healing are available to date. However, in preclinical wound healing models EGFR selective tyrosine kinase inhibitors were shown to retard wound healing.