Pharmacotherapeutic Group: Sex hormones and modulators of the genital system, emergency contraceptives.
ATC Code: G03AD02.
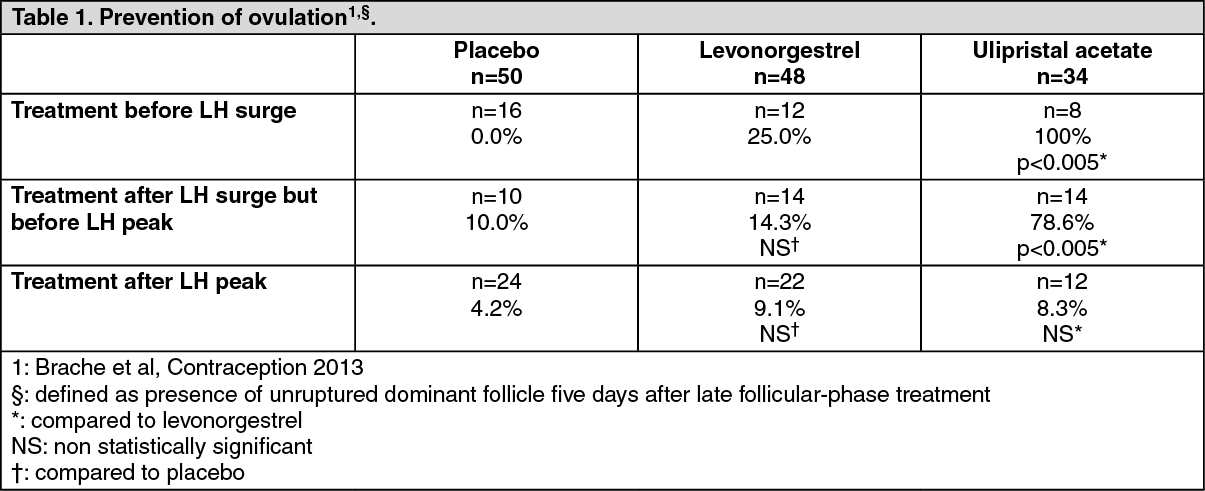
Pharmacology: Pharmacodynamics: Ulipristal acetate is an orally-active synthetic selective progesterone receptor modulator which acts via high-affinity binding to the human progesterone receptor. When used for emergency contraception the mechanism of action is inhibition or delay of ovulation via suppression of the LH surge. Pharmacodynamic data show that even when taken immediately before ovulation is scheduled to occur (when LH has already started to rise), ulipristal acetate is able to postpone follicular rupture for at least 5 days in 78.6% of cases (p<0.005 vs. levonorgestrel and vs. placebo). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Ulipristal acetate also has high affinity for the glucocorticoid receptor and
in vivo, in animals, antiglucocorticoid effects have been observed. However, in humans, no such effect has been observed even after repeat administration at the daily dose of 10 mg. It has minimal affinity to the androgen receptor and no affinity for the human estrogen or mineralocorticoid receptors.
Results from two independent randomized controlled trials (see Table 2) showed the efficacy of ulipristal acetate to be non-inferior to that of levonorgestrel in women who presented for emergency contraception between 0 and 72 hours after unprotected intercourse or contraceptive failure. When the data from the two trials were combined via meta-analysis, the risk of pregnancy with ulipristal acetate was significantly reduced compared to levonorgestrel (p=0.046). (See Table 2.)
Click on icon to see table/diagram/image
Two trials provide efficacy data on Ella used up to 120 hours after unprotected intercourse. In an open-label clinical trial, which enrolled women who presented for emergency contraception and were treated with ulipristal acetate between 48 and 120 hours after unprotected intercourse, a pregnancy rate of 2.1% (26/1241) was observed. In addition, the second comparative trial described previously also provides data on 100 women treated with ulipristal acetate from 72 to 120 hours after unprotected intercourse, in whom no pregnancies were observed.
Limited and inconclusive data from clinical trials suggest a possible trend for a reduced contraceptive efficacy of ulipristal acetate with high body weight or BMI (see Table 3). The meta-analysis of the four clinical studies conducted with ulipristral acetate presented as follows excluded women who had further acts of unprotected intercourse. (See Table 3.)
Click on icon to see table/diagram/image
A post-marketing observational study evaluating efficacy and safety of Ella in adolescents aged 17 and younger showed no difference in the safety and efficacy profile compared to adult women aged 18 and older.
Pharmacokinetics: Absorption: Following oral administration of a single 30 mg dose, ulipristal acetate is rapidly absorbed, with a peak plasma concentration of 176 ± 89 ng/ml occurring approximately 1 hour (0.5-2.0 h) after ingestion, and with an AUC
0-∞ of 556 ± 260 ng.h/ml.
Administration of ulipristal acetate together with a high-fat breakfast resulted in approximately 45% lower mean Cmax, a delayed Tmax (from a median of 0.75 hours to 3 hours) and 25% higher mean AUC
0-∞ compared with administration in the fasted state. Similar results were obtained for the active mono-demethylated metabolite.
Distribution: Ulipristal acetate is highly bound (>98%) to plasma proteins, including albumin, alpha-1-acid glycoprotein, and high density lipoprotein.
Ulipristal acetate is a lipophilic compound and is distributed in breast milk, with a mean daily excretion of 13.35 μg [0-24 hours], 2.16 μg [24-48 hours], 1.06 μg [48-72 hours], 0.58 μg [72-96 hours], and 0.31 μg [96-120 hours].
In vitro data indicate that ulipristal acetate may be an inhibitor of BCRP (Breast Cancer Resistance Protein) transporters at the intestinal level. The effects of ulipristal acetate on BCRP are unlikely to have any clinical consequences.
Ulipristal acetate is not a substrate for either OATP1B1 or OATP1B3.
Biotransformation/Elimination: Ulipristal acetate is extensively metabolized to mono-demethylated, di-methylated and hydroxylated metabolites. The mono-demethylated metabolite is pharmacologically active. In vitro
data indicate that this is predominantly mediated by CYP3A4, and to a small extent by CYP1A2 and CYP2A6. The terminal half-life of ulipristal acetate in plasma following a single 30 mg dose is estimated to 32.4 ± 6.3 hours, with a mean oral clearance (CL/F) of 76.8 ± 64.0 L/h.
Special Populations: No pharmacokinetic studies with ulipristal acetate have been performed in females with impaired renal or hepatic function.
Toxicology: Preclinical Safety Data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, and genotoxicity. Most findings in general toxicity studies were related to its mechanism of action as a modulator of progesterone and glucocorticoid receptors, with antiprogesterone activity observed at exposures similar to therapeutic levels.
Information from reproductive toxicity studies is limited due to the absence of exposure measurement in these studies. Ulipristal acetate has an embryolethal effect in rats, rabbits (at repeated doses above 1 mg/kg) and in monkeys. At these repeated doses, the safety for a human embryo is unknown. At doses which were low enough to maintain gestation in the animal species, no teratogenic effects were observed.
Carcinogenicity studies (in rats and mice) showed that ulipristal acetate is not carcinogenic.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image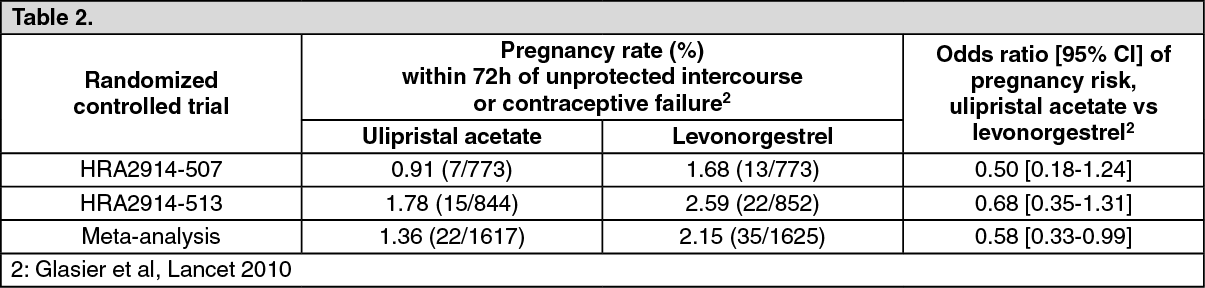 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
