


 Sign Out
Sign Out




Pharmacology: Pharmacodynamics: Mechanism of action: Apixaban is a potent, oral, reversible, direct and highly selective active site inhibitor of factor Xa. It does not require antithrombin III for antithrombotic activity. Apixaban inhibits free and clot-bound factor Xa, and prothrombinase activity. Apixaban has no direct effects on platelet aggregation, but indirectly inhibits platelet aggregation induced by thrombin. By inhibiting factor Xa, apixaban prevents thrombin generation and thrombus development. Preclinical studies of apixaban in animal models have demonstrated antithrombotic efficacy in the prevention of arterial and venous thrombosis at doses that preserved haemostasis.
Pharmacodynamic effects: The pharmacodynamic effects of apixaban are reflective of the mechanism of action (FXa inhibition). As a result of FXa inhibition, apixaban prolongs clotting tests, such as prothrombin time (PT), INR, and activated partial thromboplastin time (aPTT). Changes observed in these clotting tests at the expected therapeutic dose are small and subject to a high degree of variability. They are not recommended to assess the pharmacodynamic effects of apixaban. In the thrombin generation assay, apixaban reduced endogenous thrombin potential, a measure of thrombin generation in human plasma.
Apixaban also demonstrates anti-FXa activity as evident by reduction in Factor Xa enzyme activity in multiple commercial anti-FXa kits, however, results differ across kits. Data from clinical trials are only available for the Rotachrom Heparin chromogenic assay. Anti-Factor Xa activity exhibits a close direct linear relationship with apixaban plasma concentration, reaching maximum values at the time of apixaban peak plasma concentrations. The relationship between apixaban plasma concentration and anti-Factor Xa activity is approximately linear over a wide dose range of apixaban.
Table 1 as follows shows the predicted steady-state exposure and anti-Factor Xa activity for each indication. In patients taking apixaban for the prevention of VTE following hip or knee replacement surgery, the results demonstrate a less than 1.6-fold fluctuation in peak-to-trough levels. In non-valvular atrial fibrillation patients taking apixaban for the prevention of stroke and systemic embolism, the results demonstrate a less than 1.7-fold fluctuation in peak-to-trough levels. In patients taking apixaban for the treatment of DVT and PE or prevention of recurrent DVT and PE, the results demonstrate a less than 2.2-fold fluctuation in peak-to-trough levels. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAlthough treatment with apixaban does not require routine monitoring of exposure, a calibrated quantitative anti-Factor Xa assay may be useful in exceptional situations where knowledge of apixaban exposure may help to inform clinical decisions, e.g., overdose and emergency surgery.
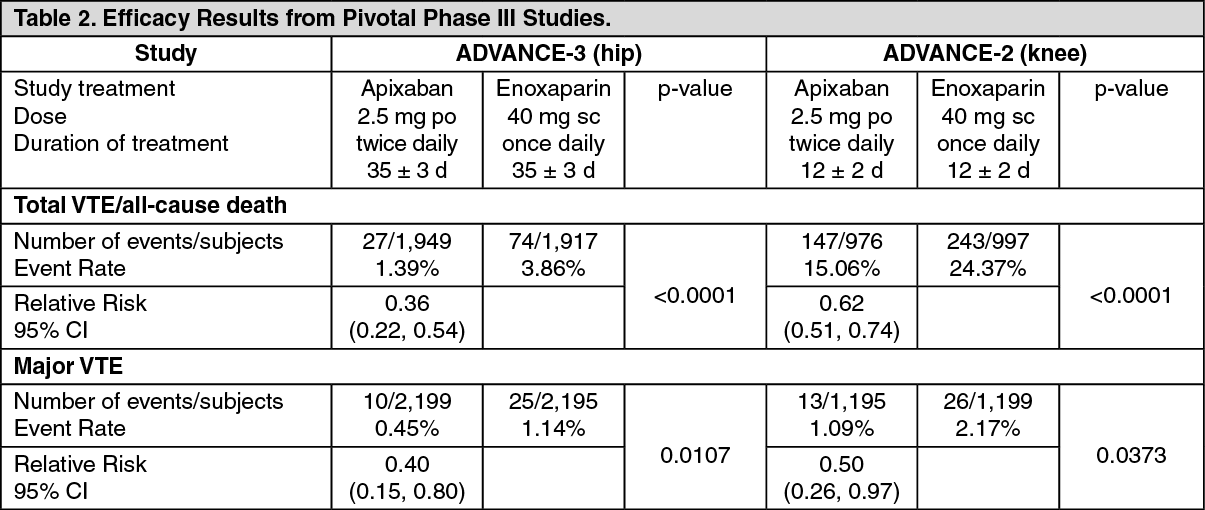
Clinical efficacy and safety: Prevention of VTE (VTEp): elective hip or knee replacement surgery: The apixaban clinical program was designed to demonstrate the efficacy and safety of apixaban for the prevention of VTE in a broad range of adult patients undergoing elective hip or knee replacement. A total of 8,464 patients were randomised in two pivotal, double-blind, multi-national studies, comparing apixaban 2.5 mg given orally twice daily (4,236 patients) or enoxaparin 40 mg once daily (4,228 patients). Included in this total were 1,262 patients (618 in the apixaban group) of age 75 or older, 1,004 patients (499 in the apixaban group) with low body weight (≤60 kg), 1,495 patients (743 in the apixaban group) with BMI ≥33 kg/m2, and 415 patients (203 in the apixaban group) with moderate renal impairment.
The ADVANCE-3 study included 5,407 patients undergoing elective hip replacement, and the ADVANCE-2 study included 3,057 patients undergoing elective knee replacement. Subjects received either apixaban 2.5 mg given orally twice daily (po bid) or enoxaparin 40 mg administered subcutaneously once daily (sc od). The first dose of apixaban was given 12 to 24 hours post-surgery, whereas enoxaparin was started 9 to 15 hours prior to surgery. Both apixaban and enoxaparin were given for 32-38 days in the ADVANCE-3 study and for 10-14 days in the ADVANCE-2 study.
Based on patient medical history in the studied population of ADVANCE-3 and ADVANCE-2 (8,464 patients), 46% had hypertension, 10% had hyperlipidemia, 9% had diabetes, and 8% had coronary artery disease.
Apixaban demonstrated a statistically superior reduction in the primary endpoint, a composite of all VTE/all-cause death, and in the Major VTE endpoint, a composite of proximal DVT, nonfatal PE, and VTE-related death, compared to enoxaparin in both elective hip or knee replacement surgery (see Table 2).
 Click on icon to see table/diagram/image
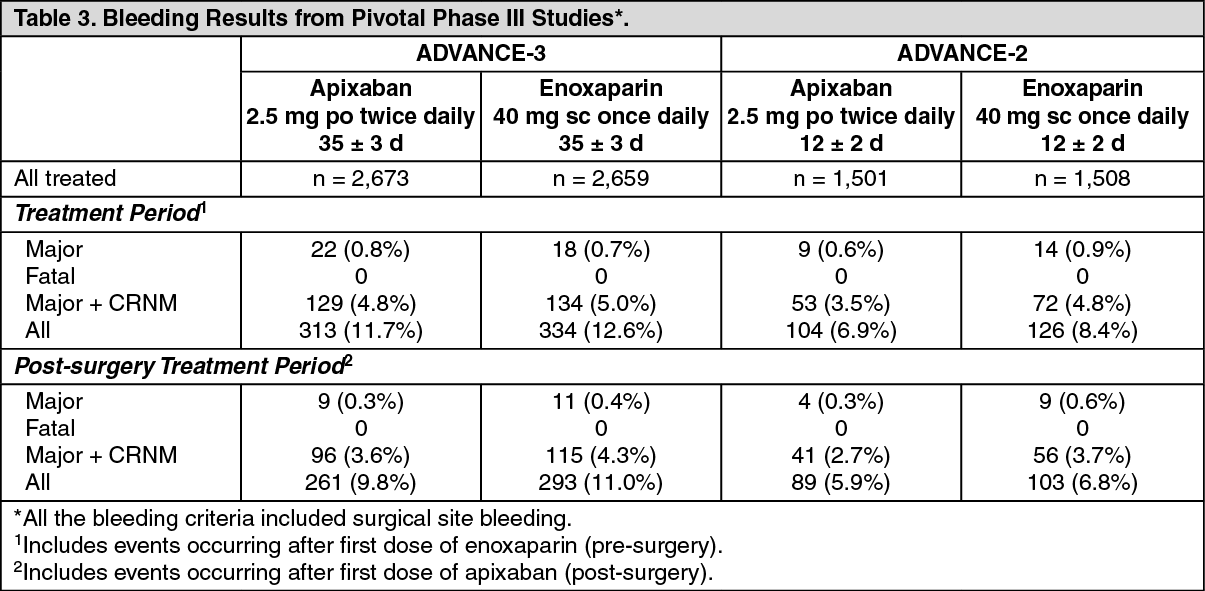
Click on icon to see table/diagram/imageThe safety endpoints of major bleeding, the composite of major and CRNM bleeding, and all bleeding showed similar rates for patients treated with apixaban 2.5 mg compared with enoxaparin 40 mg (see Table 3). All the bleeding criteria included surgical site bleeding. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe overall incidences of adverse reactions of bleeding, anaemia and abnormalities of transaminases (e.g., ALT levels) were numerically lower in patients on apixaban compared to enoxaparin in the phase II and phase III studies in elective hip and knee replacement surgery.
In the knee replacement surgery study during the intended treatment period, in the apixaban arm 4 cases of PE were diagnosed against no cases in the enoxaparin arm. No explanation can be given to this higher number of PE.
Prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation (NVAF): A total of 23,799 patients were randomised in the clinical program (ARISTOTLE: apixaban versus warfarin, AVERROES: apixaban versus ASA) including 11,927 randomised to apixaban. The program was designed to demonstrate the efficacy and safety of apixaban for the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation (NVAF) and one or more additional risk factors, such as: prior stroke or transient ischaemic attack (TIA); age ≥75 years; hypertension; diabetes mellitus; symptomatic heart failure (NYHA Class ≥II).
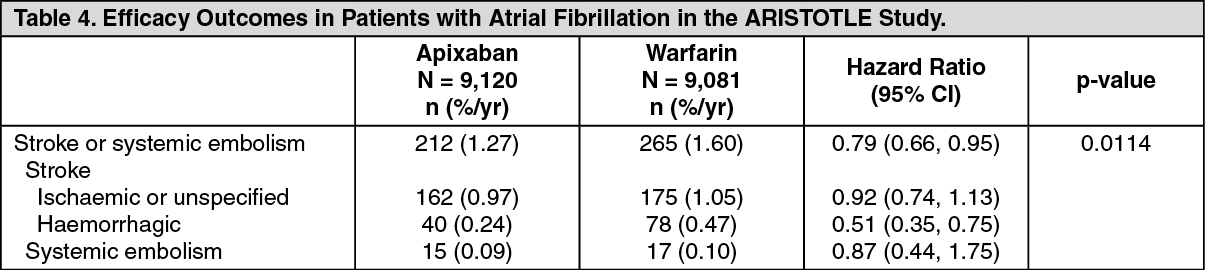
ARISTOTLE STUDY: In the ARISTOTLE study a total of 18,201 patients were randomised to double-blind treatment with apixaban 5 mg twice daily (or 2.5 mg twice daily in selected patients [4.7%], see Dosage & Administration) or warfarin (target INR range 2.0-3.0), patients were exposed to study drug for a mean of 20 months. The mean age was 69.1 years, the mean CHADS2 score was 2.1 and 18.9% of patients had prior stroke or TIA.
In the study, apixaban achieved statistically significant superiority in the primary endpoint of prevention of stroke (haemorrhagic or ischaemic) and systemic embolism (see Table 4) compared with warfarin. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor patients randomised to warfarin, the median percentage of time in therapeutic range (TTR) (INR 2-3) was 66%.
Apixaban showed a reduction of stroke and systemic embolism compared to warfarin across the different levels of center TTR; within the highest quartile of TTR according to center, the hazard ratio for apixaban vs warfarin was 0.73 (95% CI, 0.38, 1.40).
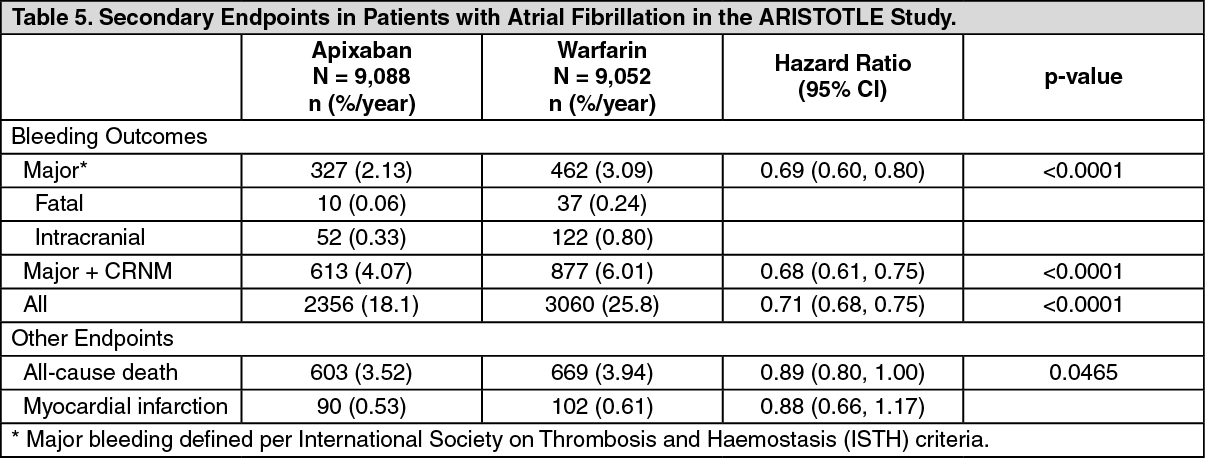
Key secondary endpoints of major bleeding and all-cause death were tested in a pre-specified hierarchical testing strategy to control the overall type 1 error in the trial. Statistically significant superiority was also achieved in the key secondary endpoints of both major bleeding and all-cause death (see Table 5). With improving monitoring of INR, the observed benefits of apixaban compared to warfarin regarding all-cause death diminish. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe overall discontinuation rate due to adverse reactions was 1.8% for apixaban and 2.6% for warfarin in the ARISTOTLE study.
The efficacy results for prespecified subgroups, including CHADS2 score, age, body weight, gender, status of renal function, prior stroke or TIA and diabetes were consistent with the primary efficacy results for the overall population studied in the trial.
The incidence of ISTH major gastrointestinal bleeds (including upper GI, lower GI, and rectal bleeding) was 0.76%/year with apixaban and 0.86%/year with warfarin.
The major bleeding results for prespecified subgroups including CHADS2 score, age, body weight, gender, status of renal function, prior stroke or TIA and diabetes were consistent with the results for the overall population studied in the trial.
AVERROES STUDY: In the AVERROES study a total of 5,598 patients considered to be unsuitable for VKA by the investigators were randomised to treatment with apixaban 5 mg twice daily (or 2.5 mg twice daily in selected patients [6.4%], see Dosage & Administration) or ASA. ASA was given at a once daily dose of 81 mg (64%), 162 (26.9%), 243 (2.1%), or 324 mg (6.6%) at the discretion of the investigator. Patients were exposed to study active substance for a mean of 14 months. The mean age was 69.9 years, the mean CHADS2 score was 2.0 and 13.6% of patients had prior stroke or TIA.
Common reasons for unsuitability for VKA therapy in the AVERROES study included unable/unlikely to obtain INRs at requested intervals (42.6%), patient refused treatment with VKA (37.4%), CHADS2 score = 1 and physician did not recommend VKA (21.3%), patient could not be relied on to adhere to VKA medicinal product instruction (15.0%), and difficulty/expected difficulty in contacting patient in case of urgent dose change (11.7%).
AVERROES was stopped early based on a recommendation by the independent Data Monitoring Committee due to clear evidence of reduction of stroke and systemic embolism with an acceptable safety profile.
The overall discontinuation rate due to adverse reactions was 1.5% for apixaban and 1.3% for ASA in the AVERROES study.
In the study, apixaban achieved statistically significant superiority in the primary endpoint of prevention of stroke (haemorrhagic, ischaemic or unspecified) or systemic embolism (see Table 6) compared to ASA. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThere was no statistically significant difference in the incidence of major bleeding between apixaban and ASA (see Table 7).
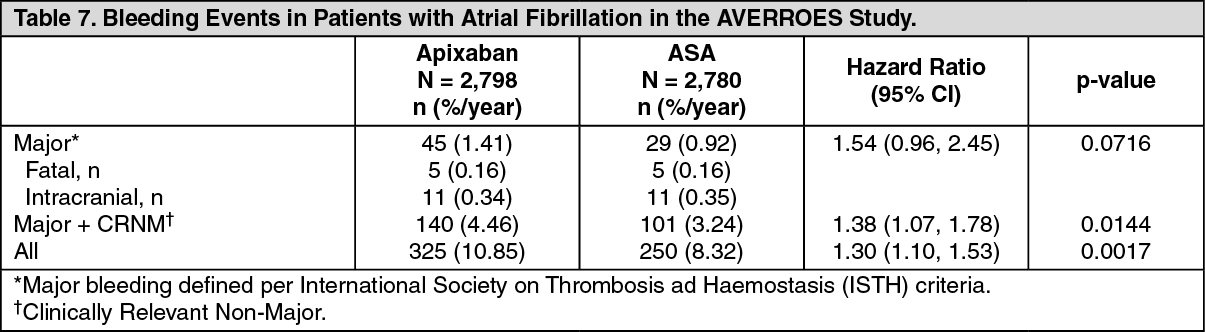 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNVAF patients with ACS and/or undergoing PCI: AUGUSTUS, an open-label, randomised, controlled, 2 by 2 factorial design trial, enrolled 4614 patients with NVAF who had ACS (43%) and/or underwent PCI (56%). All patients received background therapy with a P2Y12 inhibitor (clopidogrel: 90.3%) prescribed per local standard of care.
Patients were randomised up to 14 days after the ACS and/or PCI to either apixaban 5 mg twice daily (2.5 mg twice daily if two or more of the dose-reduction criteria were met; 4.2% received lower dose) or VKA and to either ASA (81 mg once daily) or placebo. The mean age was 69.9 years, 94% of patients randomised had a CHA2DS2-VASc score >2, and 47% had a HAS-BLED score >3. For patients randomised to VKA, the proportion of time in therapeutic range (TTR) (INR 2-3) was 56%, with 32% of time below TTR and 12% above TTR.
The primary objective of AUGUSTUS was to assess safety, with a primary endpoint of ISTH major or CRNM bleeding. In the apixaban versus VKA comparison, the primary safety endpoint of ISTH major or CRNM bleeding at month 6 occurred in 241 (10.5%), and 332 (14.7%) patients in the apixaban arm and in the VKA arm respectively (HR=0.69, 95% CI: 0.58, 0.82; 2-sided p<0.0001 for non-inferiority and p<0.0001 for superiority). For VKA, additional analyses using subgroups by TTR showed that the highest rate of bleeding was associated with the lowest quartile of TTR. The rate of bleeding was similar between apixaban and the highest quartile of TTR.
In the ASA versus placebo comparison, the primary safety endpoint of ISTH major or CRNM bleeding at month 6 occurred in 367 (16.1%), and 204 (9.0%) patients in the ASA arm and in the placebo arm respectively (HR=1.88, 95% CI: 1.58, 2.23; two-sided p<0.0001).
Specifically, in apixaban-treated patients, major or CRNM bleeding occurred in 157 (13.7%), and 84 (7.4%) patients in the ASA arm and in the placebo arm respectively. In VKA-treated patients, major or CRNM bleeding occurred in 208 (18.5%), and 122 (10.8%) patients in the ASA arm and in the placebo arm respectively.
Other treatment effects were evaluated as a secondary objective of the study, with composite endpoints.
In the apixaban versus VKA comparison, the composite endpoint of death or re-hospitalization occurred in 541 (23.5%) and 632 (27.4%) patients in the apixaban and in the VKA arm, respectively. The composite endpoint of death or ischemic event (stroke, myocardial infarction, stent thrombosis or urgent revascularization) occurred in 170 (7.4%), and 182 (7.9%) patients in the apixaban and in the VKA arm, respectively.
In the ASA versus placebo comparison, the composite endpoint of death or re-hospitalization occurred in 604 (26.2%) and 569 (24.7%) patients in the ASA and in the placebo arm, respectively. The composite endpoint of death or ischemic event (stroke, myocardial infarction, stent thrombosis or urgent revascularization) occurred in 163 (7.1%), and 189 (8.2%) patients in the ASA and in the placebo arm, respectively.
Patients undergoing cardioversion: EMANATE, an open-label, multi-center study, enrolled 1500 patients who were either oral anticoagulant naïve or pre-treated less than 48 hours and scheduled for cardioversion for NVAF. Patients were randomized 1:1 to apixaban or to heparin and/or VKA for the prevention of cardiovascular events. Electrical and/or pharmacologic cardioversion was conducted after at least 5 doses of 5 mg twice daily apixaban (or 2.5 mg twice daily in selected patients (see Dosage & Administration) or at least 2 hours after a 10 mg loading dose (or a 5 mg loading dose in selected patients (see Dosage & Administration) if earlier cardioversion was required. In the apixaban group, 342 patients received a loading dose (331 patients received the 10 mg dose and 11 patients received the 5 mg dose).
There were no strokes (0%) in the apixaban group (n=753) and 6 (0.80%) strokes in the heparin and/or VKA group (n = 747; RR 0.00, 95% CI 0.00, 0.64). All-cause death occurred in 2 patients (0.27%) in the apixaban group and 1 patient (0.13%) in the heparin and/or VKA group. No systemic embolism events were reported.
Major bleeding and CRNM bleeding events occurred in 3 (0.41%) and 11 (1.50%) patients, respectively, in the apixaban group, compared to 6 (0.83%) and 13 (1.80%) patients in the heparin and/or VKA group.
This exploratory study showed comparable efficacy and safety between apixaban and heparin and/or VKA treatment groups in the setting of cardioversion.
Treatment of DVT, treatment of PE and prevention of recurrent DVT and PE (VTEt): The clinical program (AMPLIFY: apixaban versus enoxaparin/warfarin, AMPLIFY-EXT: apixaban versus placebo) was designed to demonstrate the efficacy and safety of apixaban for the treatment of DVT and/or PE (AMPLIFY), and extended therapy for the prevention of recurrent DVT and/or PE following 6 to 12 months of anticoagulant treatment for DVT and/or PE (AMPLIFY-EXT). Both studies were randomised, parallel-group, double-blind, multinational trials in patients with symptomatic proximal DVT or symptomatic PE. All the key safety and efficacy endpoints were adjudicated by an independent blinded committee.
AMPLIFY STUDY: In the AMPLIFY study a total of 5,395 patients were randomised to treatment with apixaban 10 mg twice daily orally for 7 days followed by apixaban 5 mg twice daily orally for 6 months, or enoxaparin 1 mg/kg twice daily subcutaneously for at least 5 days (until INR≥2) and warfarin (target INR range 2.0-3.0) orally for 6 months.
The mean age was 56.9 years and 89.8% of randomised patients had unprovoked VTE events.
For patients randomised to warfarin, the mean percentage of time in therapeutic range (INR 2.0-3.0) was 60.9. Apixaban showed a reduction in recurrent symptomatic VTE or VTE-related death across the different levels of center TTR; within the highest quartile of TTR according to center, the relative risk for apixaban vs enoxaparin/warfarin was 0.79 (95% CI, 0.39, 1.61).
In the study, apixaban was shown to be non-inferior to enoxaparin/warfarin in the combined primary endpoint of adjudicated recurrent symptomatic VTE (nonfatal DVT or nonfatal PE) or VTE-related death (see Table 8).
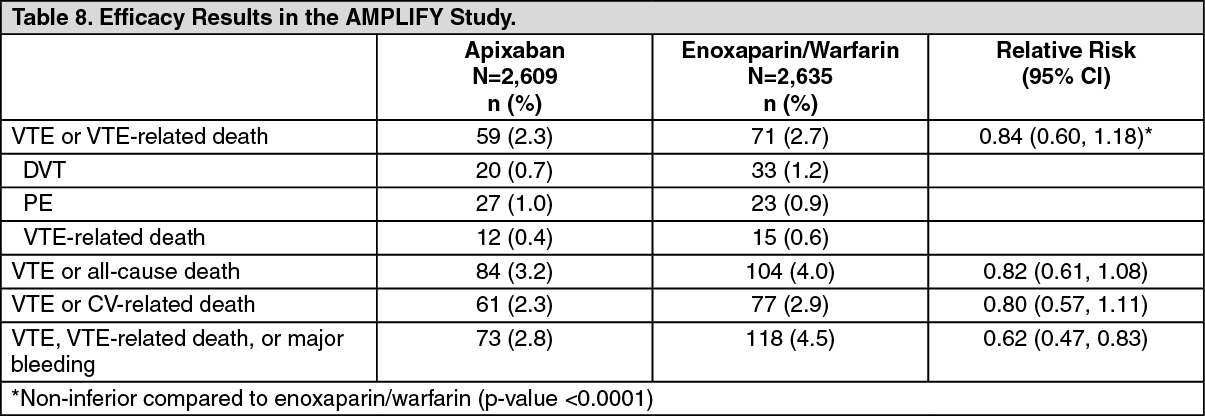 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageApixaban efficacy in initial treatment of VTE was consistent between patients who were treated for a PE [Relative Risk 0.9; 95% CI (0.5, 1.6)] or DVT [Relative Risk 0.8; 95% CI (0.5, 1.3)]. Efficacy across subgroups, including age, gender, body mass index (BMI), renal function, extent of index PE, location of DVT thrombus, and prior parenteral heparin use was generally consistent.
The primary safety endpoint was major bleeding. In the study, apixaban was statistically superior to enoxaparin/warfarin in the primary safety endpoint [Relative Risk 0.31, 95% confidence interval (0.17, 0.55), P-value <0.0001] (see Table 9).
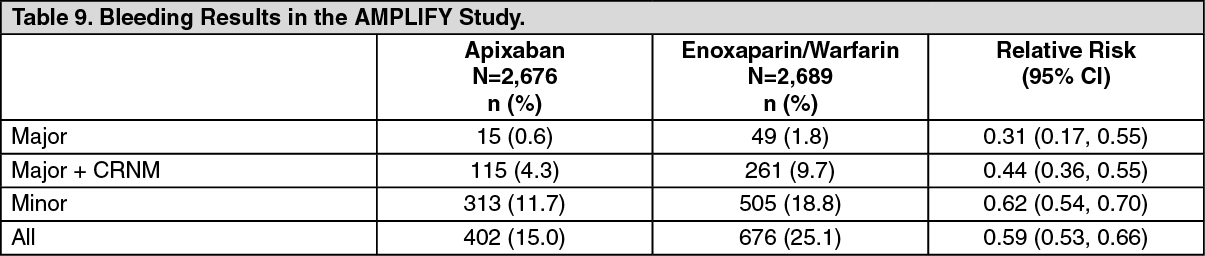 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe adjudicated major bleeding and CRNM bleeding at any anatomical site were generally lower in the apixaban group as compared to the enoxaparin/warfarin group. Adjudicated ISTH major gastrointestinal bleeding occurred in 6 (0.2%) apixaban-treated patients and 17 (0.6%) enoxaparin/warfarin-treated patients.
AMPLIFY-EXT STUDY: In the AMPLIFY-EXT study a total of 2,482 patients were randomised to treatment with apixaban 2.5 mg twice daily orally, apixaban 5 mg twice daily orally, or placebo for 12 months after completing 6 to 12 months of initial anticoagulant treatment. Of these, 836 patients (33.7%) participated in the AMPLIFY study prior to enrollment in the AMPLIFY-EXT study.
The mean age was 56.7 years and 91.7% of randomised patients had unprovoked VTE events.
In the study, both doses of apixaban were statistically superior to placebo in the primary endpoint of symptomatic, recurrent VTE (nonfatal DVT or nonfatal PE) or all-cause death (see Table 10).
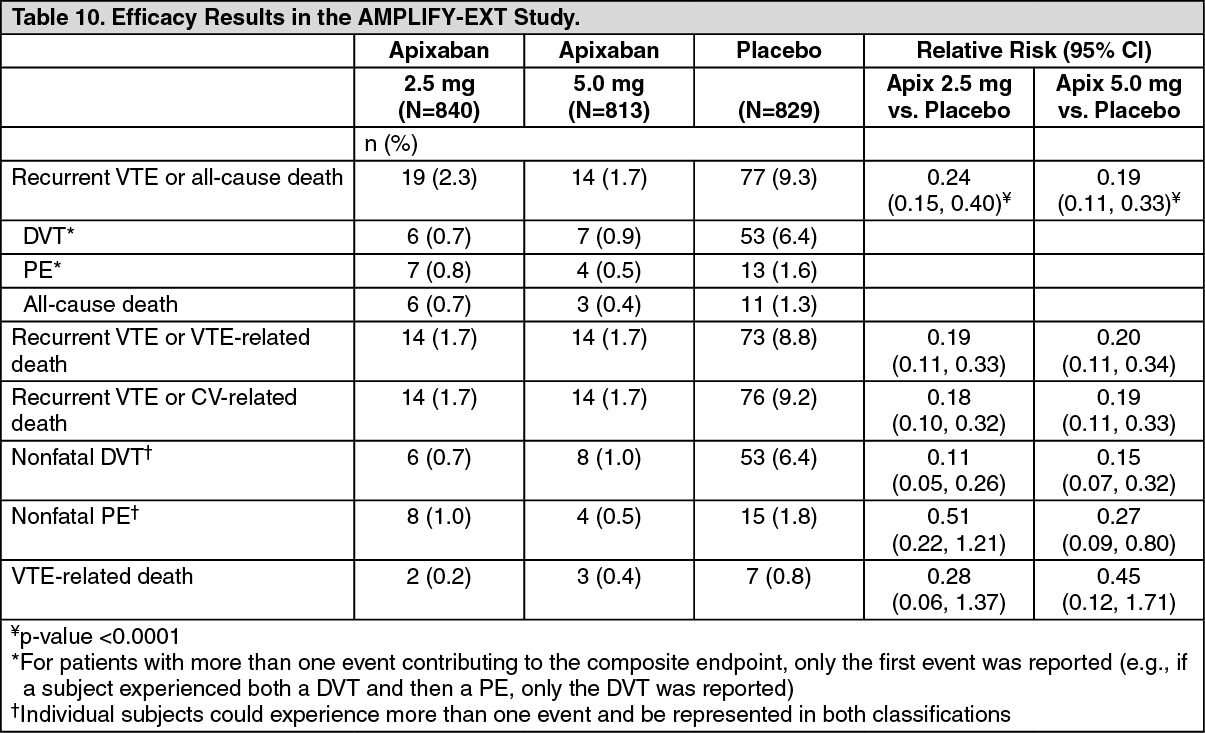 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageApixaban efficacy for prevention of a recurrence of a VTE was maintained across subgroups, including age, gender, BMI, and renal function.
The primary safety endpoint was major bleeding during the treatment period. In the study, the incidence in major bleeding for both apixaban doses was not statistically different from placebo. There was no statistically significant difference in the incidence of major + CRNM, minor, and all bleeding between the apixaban 2.5 mg twice daily and placebo treatment groups (see Table 11).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdjudicated ISTH major gastrointestinal bleeding occurred in 1 (0.1%) apixaban-treated patient at the 5 mg twice daily dose, no patients at the 2.5 mg twice daily dose, and 1 (0.1%) placebo-treated patient.
Paediatric population: The European Medicines Agency has deferred the obligation to submit the results of studies with Eliquis in one or more subsets of the paediatric population in venous and arterial embolism and thrombosis (see Dosage & Administration for information on paediatric use).
Pharmacokinetics: Absorption: The absolute bioavailability of apixaban is approximately 50% for doses up to 10 mg. Apixaban is rapidly absorbed with maximum concentrations (Cmax) appearing 3 to 4 hours after tablet intake. Intake with food does not affect apixaban AUC or Cmax at the 10 mg dose. Apixaban can be taken with or without food.
Apixaban demonstrates linear pharmacokinetics with dose-proportional increases in exposure for oral doses up to 10 mg. At doses ≥25 mg apixaban displays dissolution limited absorption with decreased bioavailability. Apixaban exposure parameters exhibit low to moderate variability reflected by a within-subject and inter-subject variability of ~20% CV and ~30% CV, respectively.
Following oral administration of 10 mg of apixaban as 2 crushed 5 mg tablets suspended in 30 mL of water, exposure was comparable to exposure after oral administration of 2 whole 5 mg tablets. Following oral administration of 10 mg of apixaban as 2 crushed 5 mg tablets with 30 g of apple puree, the Cmax and AUC were 21% and 16% lower, respectively, when compared to administration of 2 whole 5 mg tablets. The reduction in exposure is not considered clinically relevant.
Following administration of a crushed 5 mg apixaban tablet suspended in 60 mL of D5W and delivered via a nasogastric tube, exposure was similar to exposure seen in other clinical trials involving healthy subjects receiving a single oral 5 mg apixaban tablet dose.
Given the predictable, dose-proportional pharmacokinetic profile of apixaban, the bioavailability results from the conducted studies are applicable to lower apixaban doses.
Distribution: Plasma protein binding in humans is approximately 87%. The volume of distribution (Vss) is approximately 21 litres.
Biotransformation and elimination: Apixaban has multiple routes of elimination. Of the administered apixaban dose in humans, approximately 25% was recovered as metabolites, with the majority recovered in faeces. Renal excretion of apixaban accounts for approximately 27% of total clearance. Additional contributions from biliary and direct intestinal excretion were observed in clinical and non-clinical studies, respectively.
Apixaban has a total clearance of about 3.3 L/h and a half-life of approximately 12 hours.
O-demethylation and hydroxylation at the 3-oxopiperidinyl moiety are the major sites of biotransformation. Apixaban is metabolised mainly via CYP3A4/5 with minor contributions from CYP1A2, 2C8, 2C9, 2C19, and 2J2. Unchanged Apixaban is the major active substance-related component in human plasma with no active circulating metabolites present. Apixaban is a substrate of transport proteins, P-gp and breast cancer resistance protein (BCRP).
Elderly: Elderly patients (above 65 years) exhibited higher plasma concentrations than younger patients, with mean AUC values being approximately 32% higher and no difference in Cmax.
Renal impairment: There was no impact of impaired renal function on peak concentration of apixaban. There was an increase in apixaban exposure correlated to decrease in renal function, as assessed via measured creatinine clearance. In individuals with mild (creatinine clearance 51-80 mL/min), moderate (creatinine clearance 30-50 mL/min) and severe (creatinine clearance 15-29 mL/min) renal impairment, apixaban plasma concentrations (AUC) were increased 16%, 29%, and 44%, respectively, compared to individuals with normal creatinine clearance. Renal impairment had no evident effect on the relationship between apixaban plasma concentration and anti-FXa activity.
In subjects with end-stage renal disease (ESRD), the AUC of apixaban was increased by 36% when a single dose of apixaban 5 mg was administered immediately after haemodialysis, compared to that seen in subjects with normal renal function. Haemodialysis, started two hours after administration of a single dose of apixaban 5 mg, decreased apixaban AUC by 14% in these ESRD subjects, corresponding to an apixaban dialysis clearance of 18 mL/min. Therefore, haemodialysis is unlikely to be an effective means of managing apixaban overdose.
Hepatic impairment: In a study comparing 8 subjects with mild hepatic impairment, Child-Pugh A score 5 (n = 6) and score 6 (n = 2), and 8 subjects with moderate hepatic impairment, Child-Pugh B score 7 (n = 6) and score 8 (n = 2), to 16 healthy control subjects, the single-dose pharmacokinetics and pharmacodynamics of apixaban 5 mg were not altered in subjects with hepatic impairment. Changes in anti-Factor Xa activity and INR were comparable between subjects with mild to moderate hepatic impairment and healthy subjects.
Gender: Exposure to apixaban was approximately 18% higher in females than in males.
Ethnic origin and race: The results across phase I studies showed no discernible difference in apixaban pharmacokinetics between White/Caucasian, Asian and Black/African American subjects. Findings from a population pharmacokinetic analysis in patients who received apixaban were generally consistent with the phase I results.
Body weight: Compared to apixaban exposure in subjects with body weight of 65 to 85 kg, body weight >120 kg was associated with approximately 30% lower exposure and body weight <50 kg was associated with approximately 30% higher exposure.
Pharmacokinetic/pharmacodynamic relationship: The pharmacokinetic/pharmacodynamic (PK/PD) relationship between apixaban plasma concentration and several PD endpoints (anti-FXa activity, INR, PT, aPTT) has been evaluated after administration of a wide range of doses (0.5 - 50 mg). The relationship between apixaban plasma concentration and anti-Factor Xa activity was best described by a linear model. The PK/PD relationship observed in patients was consistent with that established in healthy subjects.
Toxicology: Preclinical Safety Data: Preclinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, fertility and embryo-foetal development and juvenile toxicity.
The major observed effects in the repeated dose toxicity studies were those related to the pharmacodynamic action of apixaban on blood coagulation parameters. In the toxicity studies, little to no increase of bleeding tendency was found. However, since this may be due to a lower sensitivity of the non-clinical species compared to humans, this result should be interpreted with caution when extrapolating to humans.
In rat milk, a high milk to maternal plasma ratio (Cmax about 8, AUC about 30) was found, possibly due to active transport into the milk.