Edyfil F.C.Tablet 50 mg: Each film coated tablet contains Sildenafil Citrate 70.24 mg (e.q. Sildenafil 50 mg).
Edyfil F.C.Tablet 100 mg: Each film coated tablet contains Sildenafil Citrate 140.48 mg (e.q. Sildenafil 100 mg).
Pharmacology: Pharmacodynamics: The physiological mechanism of erection of the penis involves the release of nitric oxide (NO) in the corpus cavernosum during sexual stimulation. Nitric oxide then activates the enzyme guanylate cyclase, which results in increased levels of cyclic guanosine monophosphate (cGMP), producing smooth muscle relaxation in the corpus cavernosum and allowing inflow of blood.
Sildenafil has no direct relaxant effect on isolated human corpus cavernosum but enhances the effect of NO by inhibiting the phosphodiesterase type 5 (PDE5), which is responsible for degradation of cGMP in the corpus cavernosum.
When sexual stimulation causes local release of NO, inhibition of PDE5 by sildenafil causes increased levels of cGMP in the corpus cavernosum, resulting in smooth muscle relaxation and inflow of blood to the corpus cavernosum.
Pharmacokinetics: Sildenafil pharmacokinetics are dose-proportional over the recommended dose range.
It is eliminated predominantly by hepatic metabolism (mainly CYP3A4) and is converted to an active metabolite with properties similar to the parent, sildenafil.
Absorption: Sildenafil is rapidly absorbed after oral administration, with absolute bioavailability of about 40% (range 25%-63%). In man, the mean maximum free plasma concentration of sildenafil following a single oral dose of 100 mg is approximately 18 ng/mL or 38 nM. Maximum observed plasma concentrations are reached within 30-120 min (median 60 min) of oral dosing in fasted state. When sildenafil is taken with a high fat meal, the rate of absorption is reduced, with a mean delay in Tmax of 60 min and a mean reduction in Cmax of 29%.
Distribution: The mean steady-state volume of distribution (VSS) for sildenafil is 105 L, indicating distribution into the tissues. Sildenafil and its major circulating N-desmethyl metabolite are both approximately 96% bound to plasma proteins. Protein-binding is independent of total drug concentrations.
Metabolism: Sildenafil is cleared predominantly by the CYP3A4 (major route) and CYP2C9 (minor route) hepatic microsomal isoenzymes. The major circulating metabolite results from N-demethylation of sildenafil, and is itself further metabolized. This metabolite has a PDE selectivity profile similar to sildenafil. Plasma concentrations of this metabolite are approximately 40% of those seen for sildenafil. The N-desmethyl metabolite is further metabolized, with a terminal half-life of approximately 4 hrs.
Elimination: The total body clearance of sildenafil is 41 L/hr with a resultant terminal phase half-life of 3-5 hrs. After either oral or IV administration, sildenafil is excreted as metabolites predominantly in the faeces (approximately 80% of administered oral dose) and to a lesser extent in the urine (approximately 13% of the administered oral dose).
Sildenafil is indicated for the treatment of erectile dysfunction, which is the inability to achieve or maintain a penile erection sufficient for satisfactory sexual performance. In order for Sildenafil to be effective, sexual stimulation is required.
Adults: The recommended dose is 50 mg taken, as needed, approximately 1 hr before sexual activity. Based on effectiveness and tolerance, the dose may be increased to a maximum recommended dose of 100 mg or decreased to 25 mg. The maximum recommended daily dose is 100 mg. The maximum recommended dosing frequency is once per day.
Elderly: Dosage adjustments are not required in elderly patients.
Children: Sildenafil is not indicated for use in children (<18 years).
Patients with Impaired Renal Function: Dosage adjustments are not required in patients with mild to moderate renal impairment (creatinine clearance = 30-80 mL/min).
Since sildenafil clearance is reduced in patients with severe renal impairment (creatinine clearance <30 mL/min), a 25-mg dose should be considered.
Patients with Impaired Hepatic Function: Since sildenafil clearance is reduced in patients with hepatic impairment (eg, cirrhosis), a 25-mg dose should be considered.
Patients Using Other Medicines: Given the extent of the interaction with patients receiving concomitant therapy with ritonavir, it is recommended not to exceed a maximum single dose of 25 mg sildenafil in a 48-hr period. A starting dose of 25 mg should be considered in patients receiving concomitant treatment with CYP3A4 inhibitors eg, erythromycin, saquinavir, ketoconazole, itraconazole.
In order to minimize the potential for developing postural hypotension, patients should be stable on α-blocker therapy prior to initiating sildenafil treatment. In addition, initiation of sildenafil at lower doses should be considered.
Mode of Administration: For oral administration.
In cases of overdose, standard supportive measures should be adopted as required. Renal dialysis is not expected to accelerate clearance as sildenafil is highly bound to plasma proteins and is not eliminated in the urine.
Known hypersensitivity to any component of Edyfil.
Sildenafil was shown to potentiate the hypotensive effects of acute and chronic nitrates and its administration to patients who are concurrently using nitric oxide donors, organic nitrates or organic nitrites in any form either regularly or intermittently is therefore contraindicated.
A thorough medical history and physical examination should be undertaken to diagnose erectile dysfunction, determine potential underlying causes and identify appropriate treatment.
There is a degree of cardiac risk associated with sexual activity; therefore, physicians may wish to consider the status of the patients prior to initiating any treatment for erectile dysfunction. However, prior to prescribing sildenafil, physicians should carefully consider whether the patients with certain underlying conditions could be adversely affected by such vasodilatory effects, especially in combination with sexual activity. Patients with increased susceptibility to vasodilators include those with left ventricular outflow obstruction (eg, aortic stenosis, hypertrophic obstructive cardiomyopathy), or those with the rare syndrome of multiple system atrophy manifesting as severely impaired autonomic control of blood pressure.
Agents for the treatment of erectile dysfunction should be used with caution in patients with anatomical deformation of the penis (eg, angulation, cavernosal fibrosis or Peyronie's disease), or in patients who have conditions which may predispose to priapism (eg, sickle cell anaemia, multiple myeloma or leukaemia).
Agents for the treatment of erectile dysfunction should not be used in men for whom sexual activity is inadvisable.
The safety and efficacy of combinations of sildenafil with other treatments for erectile dysfunction have not been studied, and the use of such combinations is not recommended.
Caution is advised when sildenafil is administered to patients taking an α-blocker, as the co-administration may lead to symptomatic hypotension in a few susceptible individuals. In order to minimize the potential for developing postural hypotension, patients should be hemodynamically stable on α-blocker therapy prior to initiating sildenafil treatment. Initiation of sildenafil at lower doses should be considered.
In addition, physicians should advise patients what to do in the event of postural hypotensive symptoms.
There is no safety information on the administration of sildenafil to patients with bleeding disorders or active peptic ulceration, therefore, sildenafil should be administered with caution to these patients.
A minority of patients with inherited condition, retinitis pigmentosa, have genetic disorders of retinal phosphodiesterases. There is no safety information on the administration of sildenafil to patients with retinitis pigmentosa, therefore, sildenafil should be administered with caution to these patients.
Effects on the ability to drive or operate machinery: No recommendations.
Sildenafil is not indicated for use in women. There are no adequate and well controlled studies in pregnant or lactating women.
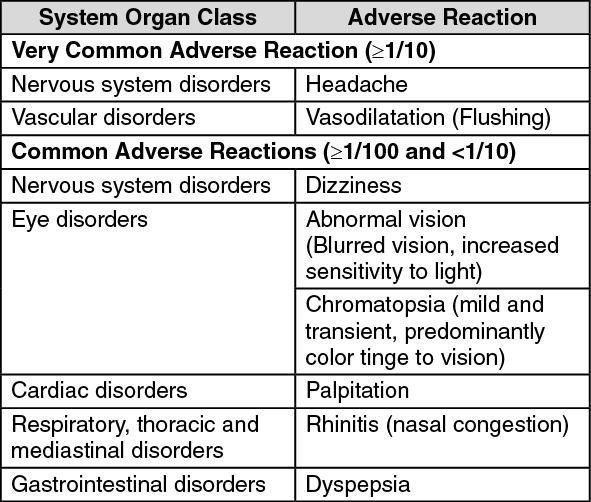
The adverse events were generally transient and mild to moderate in nature.
The incidence of some adverse events increased with dose.
The most commonly reported adverse reactions were headache and flushing.
At doses above the recommended dose range, adverse events were similar to those detailed previously but generally were reported more frequently. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Other possible side effects are:
Immune System Disorders: Hypersensitivity reaction (including skin rash).
Cardiac Disorders: Tachycardia.
Vascular Disorders: Hypotension, syncope, epistaxis.
Gastrointestinal Disorders: Vomiting.
Eye Disorders: Eye pain, red eyes/bloodshot eyes.
Reproductive System and Breast Disorders: Prolonged erection and/or priapism.
Sildenafil metabolism is principally mediated by the cytochrome P-450 (CYP) isoforms 3A4 (major route) and 2C9 (minor route). Inhibitors of these isoenzymes may reduce sildenafil clearance. Co-administration of CYP3A4 inhibitors (e.g. ketoconazole, erythromycin, cimetidine) will reduce sildenafil clearance.
Co-administration of the HIV protease inhibitor, ritonavir, which is a highly potent P-450 inhibitor with sildenafil resulted in increase in sildenafil Cmax and plasma AUC. Sildenafil had no effect on ritonavir pharmacokinetics.
Single doses of antacid (magnesium hydroxide/aluminium hydroxide) did not affect the bioavailability of sildenafil.
Sildenafil is a weak inhibitor of the cytochrome P-450 isoforms 1A2, 2C9, 2C19, 2D6, 2E1 and 3A4 (IC50 >150 micromole). Given sildenafil peak plasma concentrations of approximately 1 micromole after recommended dose, it is unlikely that will alter the clearance of substrates of these isoenzymes.
Sildenafil (50 mg) did not potentiate the increase in bleeding time caused by aspirin (150 mg).
Sildenafil (50 mg) did not potentiate the hypotensive effects of alcohol with maximum blood alcohol levels of 0.08% (80 mg/dL).
No interaction was seen when sildenafil (100 mg) was co-administered with amlodipine in hypertensive patients.
When the α-blocker doxazosin (4 mg) and sildenafil (25, 50 or 100 mg) were administered simultaneously to patients with benign prostatic hyperplasia (BPH), additional average reductions of supine blood pressure were observed. When higher doses of sildenafil and doxazosin (4 mg) were administered simultaneously, there were infrequent reports of patients who experienced symptomatic postural hypotension within 1-4 hrs of dosing. Simultaneous administration of sildenafil to patients taking α-blocker therapy may lead to symptomatic hypotension in some patients.
Store at temperature below 30°C.
Shelf-Life: 3 years.
G04BE03 - sildenafil ; Belongs to the class of drugs used in erectile dysfunction.
Edyfil FC tab 100 mg
10 × 4's;12 × 4's
Edyfil FC tab 50 mg
10 × 4's;12 × 4's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
