For breast, non-small cell lung, gastric, and head and neck cancers, premedication consisting of an oral corticosteroid, such as dexamethasone 16 mg per day (e.g. 8 mg BID) for 3 days starting 1 day prior to docetaxel administration, unless contraindicated, can be used. Prophylactic G-CSF may be used to mitigate the risk of hematological toxicities. For prostate cancer, given the concurrent use of prednisone or prednisolone the recommended premedication regimen is oral dexamethasone 8 mg, 12 hours, 3 hours and 1 hour before the docetaxel infusion.
Docetaxel is administered as a one-hour infusion every three weeks.
Breast cancer: In the adjuvant treatment of operable node-positive breast cancer, the recommended dose of docetaxel is 75 mg/m
2 administered 1-hour after doxorubicin 50 mg/m
2 and cyclophosphamide 500 mg/m
2 every 3 weeks for 6 cycles. For the treatment of patients with locally advanced or metastatic breast cancer, the recommended dosage of docetaxel is 100 mg/m
2 in monotherapy. In first-line treatment, docetaxel 75 mg/m
2 is given in combination therapy with doxorubicin (50 mg/m
2).
In combination with capecitabine, the recommended dose of docetaxel is 75 mg/m
2 every three weeks, combined with capecitabine at 1250 mg/m
2 twice daily (within 30 minutes after a meal) for 2 weeks followed by 1-week rest period. For capecitabine dose calculation according to body surface area, see capecitabine summary of product characteristics.
Non-small cell lung cancer: In chemotherapy naive patients treated for non-small cell lung cancer, the recommended dose regimen is docetaxel 75 mg/m
2 immediately followed by cisplatin 75 mg/m
2 over 30-60 minutes. For treatment after failure of prior platinum-based chemotherapy, the recommended dosage is 75 mg/m
2 as a single agent.
Prostate cancer: The recommended dose of docetaxel is 75 mg/m
2. Prednisone or prednisolone 5 mg orally twice daily is administered continuously.
Gastric adenocarcinoma: The recommended dose of docetaxel is 75 mg/m
2 as a 1 hour infusion, followed by cisplatin 75 mg/m
2, as a 1 to 3 hour infusion (both on day 1 only), and followed by 5-fluorouracil 750 mg /m
2 per day given as a 24-hour continuous infusion for 5 days, starting at the end of the cisplatin infusion. Treatment is repeated every three weeks. Patients must receive premedication with antiemetics and appropriate hydration for cisplatin administration. Prophylactic G-CSF should be used to mitigate the risk of hematological toxicities.
Head and neck cancer: Patients must receive premedication with antiemetics and appropriate hydration (prior to and after cisplatin administration). Prophylactic G-CSF may be used to mitigate the risk of haematological toxicities. All patients on the docetaxel-containing arm of the TAX 323 and TAX 324 studies, received prophylactic antibiotics.
Induction chemotherapy followed by radiotherapy (TAX 323): For the induction treatment of inoperable locally advanced squamous cell carcinoma of the head and neck (SCCHN), the recommended dose of docetaxel is 75 mg/m
2 as a 1 hour infusion followed by cisplatin 75 mg/m
2 over 1 hour, on day one, followed by 5-fluorouracil as a continuous infusion at 750 mg/m
2 per day for five days. This regimen is administered every 3 weeks for 4 cycles. Following chemotherapy, patients should receive radiotherapy.
Induction chemotherapy followed by chemo radiotherapy (TAX 324): For the induction treatment of patients with locally advanced (technically unresectable, low probability of surgical cure, and aiming at organ preservation) squamous cell carcinoma of the head and neck (SCCHN), the recommended dose of docetaxel is 75 mg/m
2 as a 1 hour intravenous infusion on day 1, followed by cisplatin 100 mg/m
2 administered as a 30-minute to 3-hour infusion, followed by 5-fluorouracil 1000 mg/m
2/day as a continuous infusion from day 1 to day 4. This regimen is administered every 3 weeks for 3 cycles. Following chemotherapy, patients should receive chemo radiotherapy.
For cisplatin and 5-fluorouracil dose modifications, see the corresponding summary of product characteristics.
Ovarian Cancer: The recommended dosage is 100mg/m
2 administered as one hour infusion every three weeks. When use in combination, docetaxel is administered at the recommended dosage of 75 mg/m
2.
Squamous Cell Carcinoma of the Head and Neck: The recommended dosage is 100mg/m
2 administered as one hour infusion every three weeks. When use in combination, docetaxel is administered at the recommended dosage of 75 mg/m
2.
Dosage adjustment during treatment: General: Docetaxel should be administered when the neutrophil count is =1,500 cells/mm
3. In patients who experienced either febrile neutropenia, neutrophil < 500 cells /mm
3 for more than one week, severe or cumulative cutaneous reactions or severe peripheral neuropathy during docetaxel therapy, the dose of docetaxel should be reduced from 100mg/m
2 to 75mg/m
2 and/or from 75 to 60mg/m
2. If the patient continues to experience these reactions at 60mg/m
2, the treatment should be discontinued.
Adjuvant therapy for breast cancer: In patients who received adjuvant therapy for breast cancer and who experienced complicated neutropenia (including prolonged neutropenia, febrile neutropenia, or infection), it was recommended to use G-CSF to provide prophylactic coverage (eg. Day 4 to 11) in all subsequent cycles. Patients who continued to experience this reaction should remain on G-CSF and have their docetaxel dose reduced to 60mg/m
2.
However, in clinical practice neutropenia could occur earlier. Thus the use of G-CSF should be considered function of the neutropenic risk of the patient and current recommendations. Patients who experience Grade 3 or 4 stomatitis should have their dose decreased to 60mg/m
2.
In combination with cisplatin: For patients who are dosed initially at docetaxel 75mg/m
2 in combination with cisplatin and whose nadir of platelet count during the previous course of therapy is <25000 cells/mm
2, or in patients who experience febrile neutropenia, or in patients with serious non-hematologic toxicities, the docetaxel dosage in subsequent cycles should be reduced to 65mg/m
2. For cisplatin dosage adjustments, see manufacturer's summary of product characteristics.
In combination with capecitabine: For capecitabine dose modifications, see capecitabine summary of product characteristics.
For patients developing the first appearance of a Grade 2 toxicity, which persists at the time of the next docetaxel /capecitabine treatment, delay treatment until resolved to Grade 0-1, and resume at 100% of the original dose.
For patients developing the second appearance of a Grade 2 toxicity, or the first appearance of a Grade 3 toxicity, at any time during the treatment cycle, delay treatment until resolved to Grade 0-1, then resume treatment with docetaxel 55mg/m
2.
For any subsequent appearances of toxicities, or any Grade 4 toxicities, discontinue the docetaxel dose.
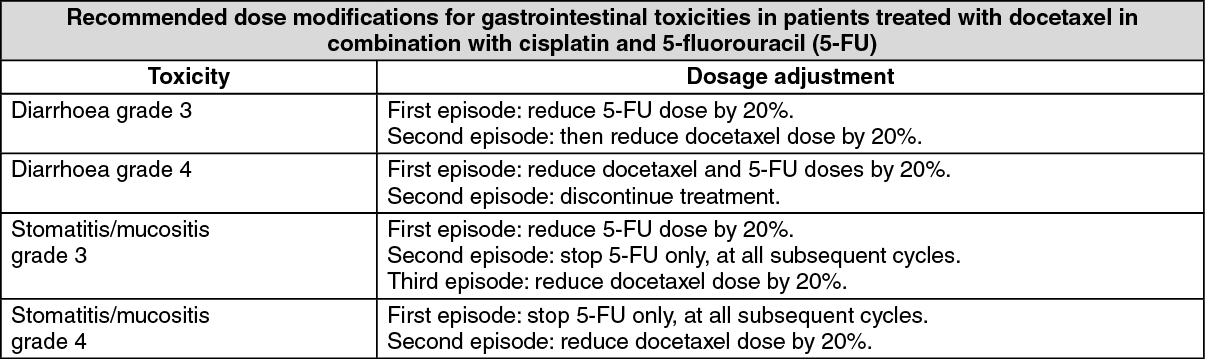
In Combination with Cisplatin and 5-fluorouracil: If an episode of febrile neutropenia, prolonged neutropenia or neutropenic infection occurs despite G-CSF use, the docetaxel dose should be reduced from 75 to 60 mg/m
2. If subsequent episodes of complicated neutropenia occur the docetaxel dose should be reduced from 60 to 45 mg/m
2. In case of Grade 4 thrombocytopenia the docetaxel dose should be reduced from 75 to 60 mg/m
2. Patients should not be retreated with subsequent cycles of docetaxel until neutrophils recover to a level >1,500 cells/mm
3 and platelets recover to a level > 100,000 cells/mm
3. Discontinue treatment if these toxicities persist. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
For cisplatin and 5-fluorouracil dosage adjustments, see manufacturers' summary of product characteristics.
In patients who received an induction treatment with docetaxel for inoperable locally advanced squamous SCCHN and who experienced complicated neutropenia (including prolonged neutropenia, febrile neutropenia, or infection), it was recommended to use G-CSF to provide prophylactic coverage (eg, day 6-15) in all subsequent cycles.
Special populations: Patients with Hepatic Impairment: Based on pharmacokinetic data with docetaxel at 100 mg/m
2 as single agent, patients who have both elevations of transaminase (ALT and/or AST) greater than 1.5 times the upper limit of the normal range (ULN) and alkaline phosphatase greater than 2.5 times the ULN, the recommended dose of docetaxel is 75 mg/m
2 (see Precautions and Pharmacology: Pharmacokinetics under Actions). For those patients with serum bilirubin > ULN and/or ALT and AST > 3.5 times the ULN associated with alkaline phosphatase > 6 times the ULN, no dose reduction can be recommended and docetaxel should not be used unless strictly indicated.
In combination with cisplatin and 5-fluorouracil for the treatment of patients with gastric adenocarcinoma, the pivotal clinical study excluded patients with ALT and/or AST > 1.5 × ULN associated with alkaline phosphatase > 2.5 × ULN, and bilirubin > 1 x ULN; for these patients, no dose-reductions can be recommended and docetaxel should not be used unless strictly indicated. No data are available in patients with hepatic impairment treated by docetaxel in combination in the other indications.
Paediatric Population: The safety and efficacy of DOXOL in nasopharyngeal carcinoma in children aged 1 month to less than 18 years have not been established.
There is no relevant use of DOXOL in the Paediatric population in the indications breast cancer, non-small cell lung cancer, prostate cancer, gastric carcinoma and head and neck cancer, not including type II and III less differentiated nasopharyngeal carcinoma.
Elderly Patients: Based on a population pharmacokinetic analysis, there are no special instructions for use in the elderly.
In combination with capecitabine, for patients 60 years of age or more, a starting dose reduction of capecitabine to 75% is recommended (see capecitabine summary of product characteristics).
Preparation for the intravenous administration: Preparation of the infusion solution: Each vial is of single use and should be used immediately.
DO NOT use other docetaxel medicinal products consisting of 2 vials (concentrate and solvent) with this medicinal product (Docetaxel 20 mg/0.5 ml & 80 mg/2 ml concentrate for solution for infusion, which contains only 1 vial).
Docetaxel 20 mg/0.5 ml & 80 mg/2 ml concentrate for solution for infusion requires NO prior dilution with a solvent and is ready to add to the infusion solution.
Unopened Vials are stored below 30°C. If the vials are stored under refrigeration (2°C - 8°C), allow the required number of boxes of Docetaxel concentrate for solution for infusion to stand below 25°C for 5 minutes before use.
More than one vial of Docetaxel concentrate for solution for infusion may be necessary to obtain the required dose for the patient. Aseptically withdraw the required amount of Docetaxel concentrate for solution for infusion using a calibrated syringe.
The required volume of Docetaxel 20 mg/0.5 ml & 80 mg/2 ml concentrate for solution for infusion must be injected via a single injection (one shot) into a 250 ml infusion bag or bottle containing either 5% glucose solution or sodium chloride 9 mg/ml (0.9%) solution for infusion.
If a dose greater than 200 mg of docetaxel is required, use a larger volume of the infusion vehicle so that a concentration of 0.74 mg/ml docetaxel is not exceeded.
Mix the infusion bag or bottle manually using a rocking motion.
The infusion bag solution should be used within 6 hours below 25°C including the one hour infusion to the patient or used within 24hours when stored between 2 to 8°C in the infusion bag.
As with all parenteral products, Docetaxel infusion solution should be visually inspected prior to use, solutions containing a precipitate should be discarded.
Any unused product or waste material should be disposed of in accordance with local requirements.
If Docetaxel concentrate or infusion solution should come into contact with skin, wash immediately and thoroughly with soap and water. If Docetaxel concentrate or infusion solution should come into contact with mucous membranes, wash immediately and thoroughly with water.
Mode of administration: Intravenous Administration.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
