Pharmacotherapeutic Group: Direct-acting antiviral.
ATC Code: J05AP07.
Pharmacology: Pharmacodynamics: Mechanism of action: Daclatasvir is an inhibitor of nonstructural protein 5A (NS5A), a multifunctional protein that is an essential component of the HCV replication complex. Daclatasvir inhibits both viral RNA replication and virion assembly.
Antiviral activity in cell culture: Daclatasvir is an inhibitor of HCV genotypes 1a and 1b replication in cell-based replicon assays with effective concentration (50% reduction, EC
50) values of 0.003-0.050 and 0.001-0.009 nM, respectively, depending on the assay method. The daclatasvir EC
50 values in the replicon system were 0.003-1.25 nM for genotypes 3a, 4a, 5a and 6a, and 0.034-19 nM for genotype 2a as well as 0.020 nM for infectious genotype 2a (JFH-1) virus.
Daclastavir showed additive to synergistic interactions with interferon alfa, HCV nonstructural protein 3 (NS3) PIs, HCV nonstructural protein 5B (NS5B) non-nucleoside inhibitors, and HCV NS5B nucleoside analogues in combination studies using the cell-based HCV replicon system. No antagonism of antiviral activity was observed.
No clinically relevant antiviral activity was observed against a variety of RNA and DNA viruses, including HIV, confirming that daclastavir, which inhibits a HCV-specific target, is highly selective for HCV.
Resistance in cell culture: Substitutions conferring daclatasvir resistance in genotypes 1-4 were observed in the N-terminal 100 amino acid region of NS5A in a cell-based replicon system. L31V and Y93H were frequently observed resistance substitutions in genotype 1b, while M28T, L31V/M, Q3OE/H/R, and Y93C/H/N were frequently observed resistance substitutions in genotype 1a. These substitutions conferred low level resistance (EC
50 <1 nM) for genotype 1b, and higher levels of resistance for genotype 1a (EC
50 up to >350 nM). The most resistant variants with single amino acid substitution in genotype 2a and genotype 3a were F28S (EC
50 >300 nM) and Y93H (EC
50 >1,000 nM), respectively. In genotype 4, amino acid substitutions at 30 and 93 (EC
50 <16 nM) were frequently selected.
Cross-resistance: HCV replicons expressing daclatasvir-associated resistance substitutions remained fully sensitive to interferon alfa and other anti-HCV agents with different mechanisms of action, such as NS3 protease and NS5B polymerase (nucleoside and non-nucleoside) inhibitors.
Clinical efficacy and safety: In clinical studies of daclatasvir in combination with sofosbuvir or with peginterferon alfa and ribavirin, plasma HCV RNA values were measured using the COBAS TaqMan HCV test (version 2.0), for use with the High Pure System, with a lower limit of quantification (LLOQ) of 25 IU/ml. SVR was the primary endpoint to determine the HCV cure rate, which as defined as HCV RNA less than LLOQ at 12 weeks after the end of treatment (SVR12) for AI444040, ALLY-1 (AI444215), ALLY-2 (AI444216), ALLY-3 (AI444218), AI444042 and as HCV RNA undetectable at 24 weeks after the end of treatment (SVR24) for study AI444010.
Daclatasvir in combination with sofosbuvir: The efficacy and safety of daclatasvir 60 mg once daily in combination with sofosbuvir 400 mg once daily, with or without ribavirin, in the treatment of infection with chronic HCV genotype 1, 2, or 3 were evaluated in four open-label studies (AI444040, ALLY-1, ALLY-2 and ALLY-3).
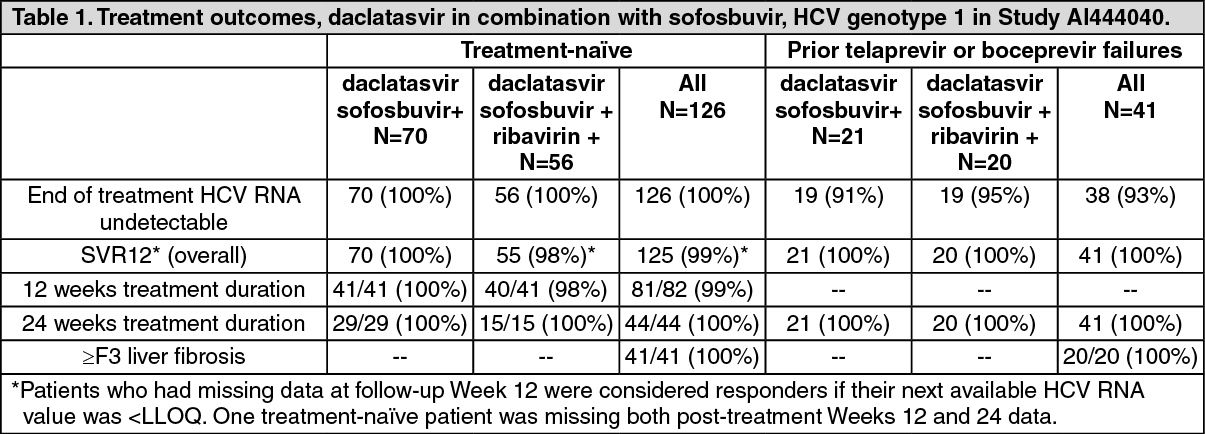
In study AI444040, 211 adults with HCV genotype 1, 2, or 3 infection and without cirrhosis received daclatasvir and sofosbuvir, with or without ribavirin. Among the 167 patients with HCV genotype 1 infection, 126 were treatment-naive and 41 had failed prior therapy with a PI regimen (boceprevir or telaprevir). All 44 patients with HCV genotype 2 (n=26) or 3 (n=18) infection were treatment-naive.
Treatment duration was 12 weeks for 82 treatment-naive HCV genotype 1 patients, and 24 weeks for all other patients in the study. The 211 patients had a median age of 54 years (range: 20 to 70); 83% were white; 12% were black/African-American; 2% were Asian; 20% were Hispanic or Latino. The mean score on the FibroTest (a validated non-invasive diagnostic assay) was 0.460 (range: 0.03 to 0.89). Conversion of the FibroTest score to the corresponding METAVIR score suggests that 35% of all patients (49% of patients with prior PI failure, 30% of patients with genotype 2 or 3) had ≥F3 liver fibrosis. Most patients (71%, including 98% of prior PI failures) had IL-28B rs12979860 non-CC genotypes.
SVR12 was achieved by 99% patients with HCV genotype 1, 96% of those with genotype 2 and 89% of those with genotype 3 (see Tables 1 and 2). Response was rapid (viral load at Week 4 showed that more than 97% of patients responded to therapy), and was not influenced by HCV subtype (1a/1b), IL28B genotype, or use of ribavirin. Among treatment-naive patients with HCV RNA results at both follow-up Weeks 12 and 24, concordance between SVR12 and SVR24 was 99.5% independent of treatment duration.
Treatment-naive patients with HCV genotype 1 who received 12 weeks of treatment had a similar response as those treated for 24 weeks (Table 1). (See Tables 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Advanced cirrhosis and post-liver transplant (ALLY-1): In the study ALLY-1, the regimen of daclatasvir, sofosbuvir, and ribavirin administered for 12 weeks was evaluated in 113 adults with chronic hepatitis C and Child-Pugh A, B or C cirrhosis (n=60) or HCV recurrence after liver transplantation (n=53). Patients with HCV genotype 1, 2, 3, 4, 5 or 6 infection were eligible to enroll. Patients received daclatasvir 60 mg once daily, sofosbuvir 400 mg once daily, and ribavirin (600 mg starting dose) for 12 weeks and were monitored for 24 weeks post treatment.
Patients demographics and main disease characteristics are summarised in Table 3. (See Table 3.)
Click on icon to see table/diagram/image
SVR12 was achieved by 83% (50/60) of patients in the cirrhosis cohort, with a marked difference between patients with Child-Pugh A or B (92-94%) as compared to those with Child-Pugh C and 94% of patients in the post-liver transplant cohort (Table 4). SVR rates were comparable regardless of age, race, gender, IL28B allele status, or baseline HCV RNA level. In the cirrhosis cohort, 4 patients with hepatocellular carcinoma underwent liver transplantation after 1-71 days of treatment; 3 of the 4 patients received 12 weeks of post-liver transplant treatment extension and 1 patient, treated for 23 days before transplantation, did not receive treatment extension. All 4 patients achieved SVR12. (See Table 4.)
Click on icon to see table/diagram/image
HCV/HIV co-infection (ALLY-2): In study ALLY-2, the combination of daclatasvir and sofosbuvir administered for 12 weeks was evaluated in 153 adults with chronic hepatitis C and HIV co-infection; 101 patients were HCV treatment-naive and 52 patients had failed prior HCV therapy. Patients with HCV genotype 1, 2, 3, 4, 5, or 6 infection were eligible to enroll, including patients with compensated cirrhosis (Child-Pugh A). The dose of daclatasvir was adjusted for concomitant antiretroviral use. Patient demographics and baseline disease characteristics are summarised in Table 5.
Click on icon to see table/diagram/image
Overall, SVR12 was achieved by 97% (149/153) of patients administered daclatasvir and sofosbuvir for 12 weeks in ALLY-2. SVR rates were >94% across combination antiretroviral therapy (cART) regimens, including boosted-PI-, NNRTI-, and integrase inhibitor (INSTI)-based therapies. SVR rates were comparable regardless of HIV regimen, age, race, gender, IL28B allele status, or baseline HCV RNA level. Outcomes by prior treatment experience are presented in Table 6.
A third treatment group in study ALLY-2 included 50 HCV treatment-naive HIV co-infected patients who received daclatasvir and sofosbuvir for 8 weeks. Demographic and baseline characteristics of these 50 patients were generally comparable to those for patients who received 12 weeks of study treatment. The SVR rate for patients treated for 8 weeks was lower with this treatment duration as summarized in Table 6. (See Table 6.)
Click on icon to see table/diagram/image
HCV Genotype 3 (ALLY-3): In study ALLY-3, the combination of daclatasvir and sofosbuvir administered for 12 weeks was evaluated in 152 adults infected with HCV genotype 3; 101 patients were treatment-naive and 51 patients had failed prior antiviral therapy. Median age was 55 years (range: 24 to 73); 90% of patients were white; 4% were black/African-American; 5% were Asian; 16% were Hispanic or Latino. The median viral load as 6.42 log
10 IU/ml, and 21% of patients had compensated cirrhosis. Most patients (61%) had IL-28B rs12979860 non-CC genotypes. SVR12 was achieved in 90% of treatment-naive patients and 86% of treatment-experienced patients. Response was rapid (viral load at Week 4 showed that more than 95% of patients responded to therapy) and was not influenced by IL28B genotype. SVR12 rates were lower among patients with cirrhosis (see Table 7).
Click on icon to see table/diagram/image
Daclatasvir in combination with peginterferon alfa and ribavirin: AI444042 and AI444010 were randomised, double-blind studies that evaluated the efficacy and safety of daclatasvir in combination with peginterferon alfa and ribavirin (pegIFN/RBV) in the treatment of chronic HCV infection in treatment-naive adults with compensated liver disease (including cirrhosis).
AI444042 enrolled patients with HCV genotype 4 infection and AI444010 enrolled patients with either genotype 1 or 4.
AI444042: Patients received daclatasvir 60 mg once daily (n=82) or placebo (n=42) plus pegIFN/RBV for 24 weeks. Patients in the daclatasvir treatment group who did not have HCV RNA undetectable at both Weeks 4 and 12 and all placebo-treated patients continued pegIFN/RBV for another 24 weeks.
Treated patients had a median age of 49 years (range: 20 to 71); 77% of patients were white; 19% were black/African-American; 4% were Hispanic or Latino. Ten percent of patients had compensated cirrhosis, and 75% of patients had IL-28B rs12979860 non-CC genotypes. Treatment outcomes in study AI444042 are presented in Table 8. Response was rapid (at Week 4 91% of daclatasvir-treated patients had HCV RNA <LLOQ). SVR12 rates were higher for patients with the IL-28B CC genotype than for those with non-CC genotypes and for patients with baseline HCV RNA less than 800,000 IU/ml but consistently higher in the daclatasvir-treated patients than for placebo-treated patients in all subgroups.
AI444010: Patients received daclatasvir 60 mg once daily (n=158) or placebo (n=78) plus pegIFN/RBV through Week 12. Patients assigned to daclatasvir 60 mg once-daily treatment group who had HCV RNA <LLOQ at Week 4 and undetectable at Week 10 were then randomised to receive another 12 weeks of daclatasvir 60 mg +pegIFN/RBV or placebo +pegIFN/RBV for a total treatment duration of 24 weeks. Patients originally assigned to placebo and those in the daclatasvir group who did not achieve HCV RNA <LLOQ at Week 4 and undetectable at Week 10 continued pegIFN/RBV to complete 48 weeks of treatment. Treated patients had a median age of 50 years (range: 18 to 67); 79% of patients were white; 13% were black/African-American; 1% were Asian; 9% were Hispanic or Latino. Seven percent of patients had compensated cirrhosis; 92% had HCV genotype 1 (72% 1a and 20% 1b) and 8% had HCV genotype 4; 65% of patients had IL-28B rs12979860 non-CC genotypes.
Treatment outcomes in study AI444010 for patients with HCV genotype 4 are presented in Table 8.
For HCV genotype 1, SVR12 rates were 64% (54% for 1a; 84% for 1b) for patients treated with daclatasvir + pegIFN/RBV and 36% for patients treated with placebo + pegIFN/RBV. For daclatasvir treated patients with HCV RNA results at both follow-up Weeks 12 and 24, concordance of SVR12 and SVR24 was 97% for HCV genotype 1 and 100% for HCV genotype 4. (See Table 8.)
Click on icon to see table/diagram/image
Long term efficacy data: Limited data are available from an ongoing follow-up study to assess durability of response up to 3 years after treatment with daclatasvir. Among patients who achieved SVR12 with daclatasvir and sofosbuvir (± ribavirin) with a median duration of post-SVR12 follow-up of 15 months, no relapses have occurred. Among patients who achieved SVR12 with daclatasvir + pegIFN/RBV with a median duration of post-SVR12 follow-up of 22 months, 1% of patients relapsed.
Resistance in clinical studies: Daclatasvir in combination with sofosbuvir: Frequency of baseline NS5A resistance-associated variants (RAVs): Baseline NS5A RAVs were frequently observed in clinical studies of daclatasvir plus sofosbuvir+/- ribavirin, with approximately 11% in genotype 1 infection (GT1a: 28, 30, 31, or 93; GT1b: 31 or 93), 50% in genotype 2 infection (L31M), 8% in genotype 3 infection (Y93H) and in 71% in genotype 4 infection (L28M or L30R).
Impact of baseline NS5A RAVs on cure rates: The baseline NS5A RAVs described previously had no major impact on cure rates in patients treated with sofosbuvir + daclatasvir +/- ribavirin, with the exception of the Y93H RAV in genotype 3 infection (seen in 16/192 [8%] of patients). The SVR12 rate in genotype-3 infected patients with this RAV is reduced (in practice as relapse after end of treatment response), especially in patients with cirrhosis.
The overall cure rate for genotype-3 infected patients who were treated for 12 weeks with sofosbuvir + daclatasvir (without ribavirin) in the presence and absence of the Y93H RAV was 7/13 (54%) and 134/145 (92%), respectively. There was no Y93H RAV present at baseline for genotype-3 infected patients treated for 12-weeks with sofosbuvir + daclatasvir + ribavirin, and thus SVR outcomes cannot be assessed.
Emerging resistance: In a pooled analysis of 629 patients who received daclatasvir and sofosbuvir with or without ribavirin in Phase 2 and 3 studies for 12 or 24 weeks, 36 patients qualified for resistance analysis due to virologic failure or early study discontinuation and having HCV RNA greater than 1,000 IU/ml.
Observed emergent NS5A resistance-associated variants are reported in Table 9. (See Table 9.)
Click on icon to see table/diagram/image
The sofosbuvir resistance-associated substitution S282T emerged in only 1 non-SVR12 patient infected with genotype 3.
No data are available on the persistence of daclatasvir resistance-associated substitutions beyond 6 months post-treatment in patients treated with daclatasvir and sofosbuvir with/without ribavirin. Emergent daclatasvir resistance-associated substitutions have been shown to persist for 2 years post-treatment and beyond for patients treated with other daclatasvir-based regimens.
Daclatasvir in combination with peginterferon alfa and ribavirin: Baseline NS5A RAVs were seen in approximately 10% of treatment-naive patients with genotype 1 infection (GT1a: 28, 30, 31, or 93; GT1b: 31 or 93) and 61% with genotype 4 infection (28, 30, 31). The majority of patients (5/9 [56%] genotype 1a, 6/8 [75%] genotype 1b and 52/57 [91%] genotype 4 patients) with these pretreatment NS5A RAVs described previously achieved SVR. NS5A RAVs generally emerged at failure (139/153 genotype 1a and 49/57 genotype 1b). The most frequently detected NS5A RAVs included Q30E or Q30R in combination with L31M. The majority of genotype 1a failures had emergent NS5A variants detected at Q30 (127/139 [91%]), and the majority of genotype 1b failures had emergent NS5A variants detected at L31 (37/49 [76%]) and/or Y93H (34/49 [69%]).
Pharmacokinetics: Absorption: Daclatasvir administered as a tablet was readily absorbed following multiple oral doses with peak plasma concentrations occurring between 1 and 2 hours.
Daclatasvir C
max, AUC, and C
min increased in a near dose-proportional manner. Steady state was achieved after 4 days of once-daily administration. At the 60 mg dose, exposure to daclatasvir was similar between healthy subjects and HCV-infected patients.
In vitro and
in vivo studies showed that daclatasvir is a substrate of P-gp. The absolute bioavailability of the tablet formulation is 67%.
Effect of food on oral absoprtion: In healthy subjects, administration of daclatasvir 60 mg tablet after a high-fat meal decreased daclatasvir C
max and AUC by 28% and 23%, respectively, compared with administration under fasting conditions. Administration of daclatasvir 60 mg tablet after a light meal resulted in no reduction in daclatasvir exposure.
Distribution: At steady state, protein binding of daclatasvir in HCV-infected patients was approximately 99% and independent of dose at the dose range studied (1 mg to 100 mg). In patients who received daclatasvir 60 mg tablet orally followed by 100μg [
13C,
15N]-daclatasvir intravenous dose, estimated volume of distribution at steady state was 47 I.
In vitro studies indicate that daclatasvir is actively and passively transported into hepatocytes. The active transport is mediated by OCT1 and other unidentified uptake transporters, but not by organic anion transporter (OAT) 2, sodium-taurocholate cotransporting polypeptide (NTCP), or OATPs.
Daclatasvir is an inhibitor of P-gp, OATP 1B1 and BCRP.
In vitro daclatasvir is an inhibitor of renal uptake transporters, OAT1 and 3, and OCT2, but is not expected to have a clinical effect on the pharmacokinetics of substrates of these transporters.
Biotransformation: In vitro and
in vivo studies demonstrate that daclatasvir is a substrate of CYP3A, with CYP3A4 being the major CYP isoform responsible for the metabolism. No metabolites circulated at levels more than 5% of the parent concentration. Daclatasvir
in vitro did not inhibit (IC
50 >40 μM) CYP enzymes 1A2, 2B6, 2C8, 2C9, 2C19, or 2D6.
Elimination: The liver is the major clearance organ for daclatasvir in humans.
In vitro studies indicate that daclatasvir is actively and passively transported into hepatocytes. The active transport is mediated by OCT1 and other unidentified uptake transporters. Following multiple-dose administration of daclatasvir in HCV-infected patients, the terminal elimination half-life of daclatasvir ranged from 12 to 15 hours. In patients who received daclatasvir 60 mg tablet orally followed by 100 μg [
13C,
15N]-daclatasvir intravenous dose, the total clearance was 4.24 l/h.
Special populations: Renal impairment: Daclatasvir unbound AUC was estimated to be 18%, 39% and 51% higher for subjects with creatinine clearance (CLcr) values of 60, 30 and 15 ml/min, respectively, relative to subjects with normal renal function. Subjects with end-stage renal disease requiring haemodialysis had a 27% increase in daclatasvir AUC and a 20% increase in unbound AUC compared to subjects with normal renal function (see Dosage & Administration).
Hepatic impairment: The C
max and AUC of total daclatasvir (free and protein-bound drug) were lower in subjects with hepatic impairment; however, hepatic impairment did not have a clinically significant effect on the free drug concentrations of daclatasvir (see Dosage & Administration).
Elderly: Population pharmacokinetic analysis of data from clinical studies indicated that age had no apparent effect on the pharmacokinetics of daclatasvir.
Paediatric population: The pharmacokinetics of daclatasvir in paediatric patients have not been evaluated.
Gender: Population pharmacokinetic analysis identified gender as a statistically significant covariate on daclatasvir apparent oral clearance (CL/F) with female subjects having slightly lower CL/F, but the magnitude of the effect on daclatasvir exposure is not clinically important.
Race: Population pharmacokinetic analysis of data from clinical studies identified race (categories "other" [patients who are not white, black or Asian] and "black") as a statistically significant covariate on daclatasvir apparent oral clearance (CL/F) and apparent volume of distribution (Vc/F) resulting in slightly higher exposures compared to white patients, but the magnitude of the effect on daclatasvir exposure is not clinically important.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image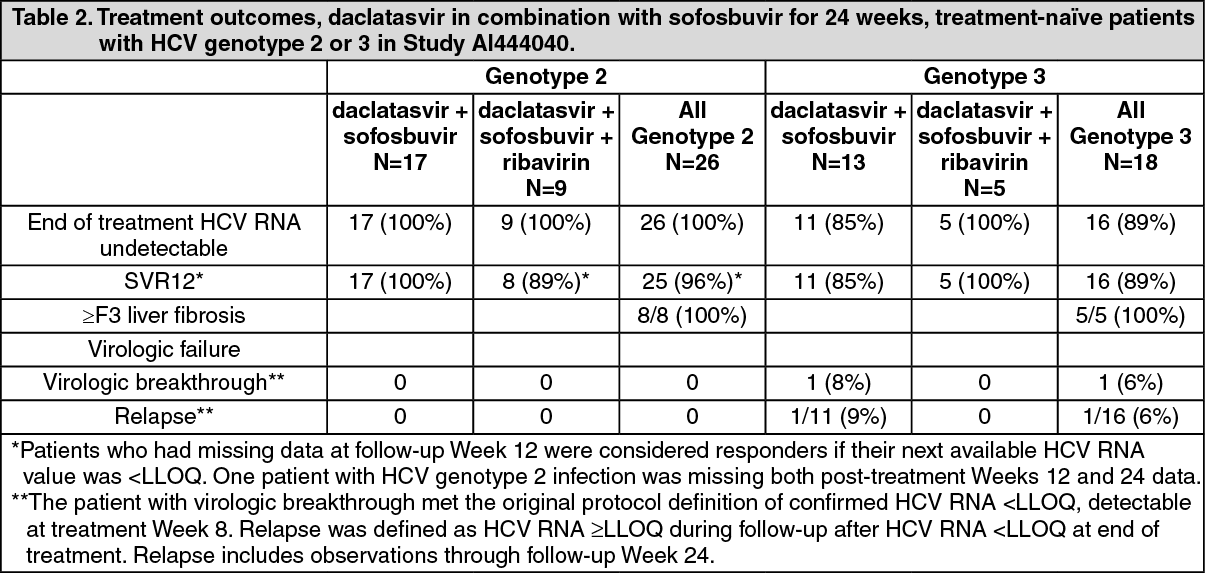 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image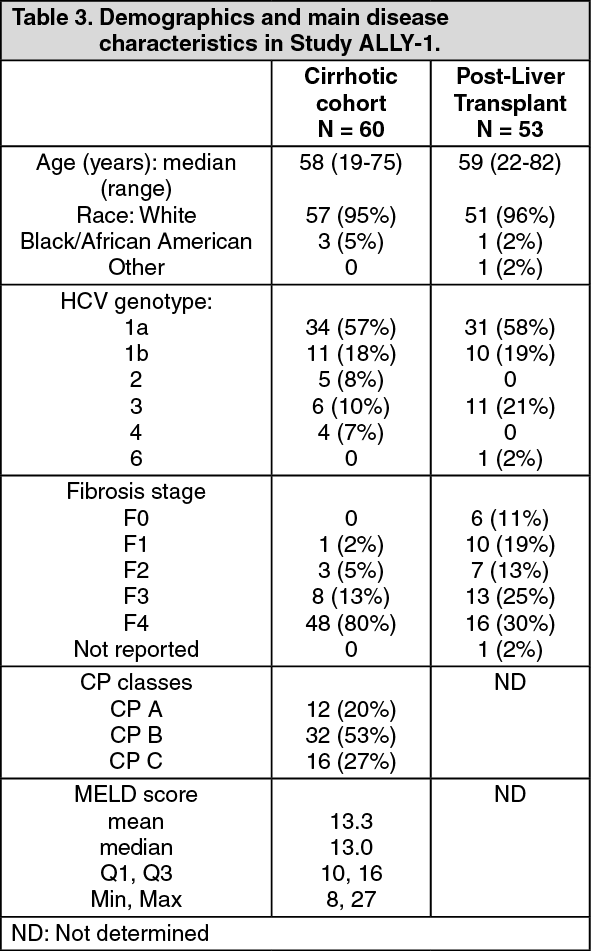 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image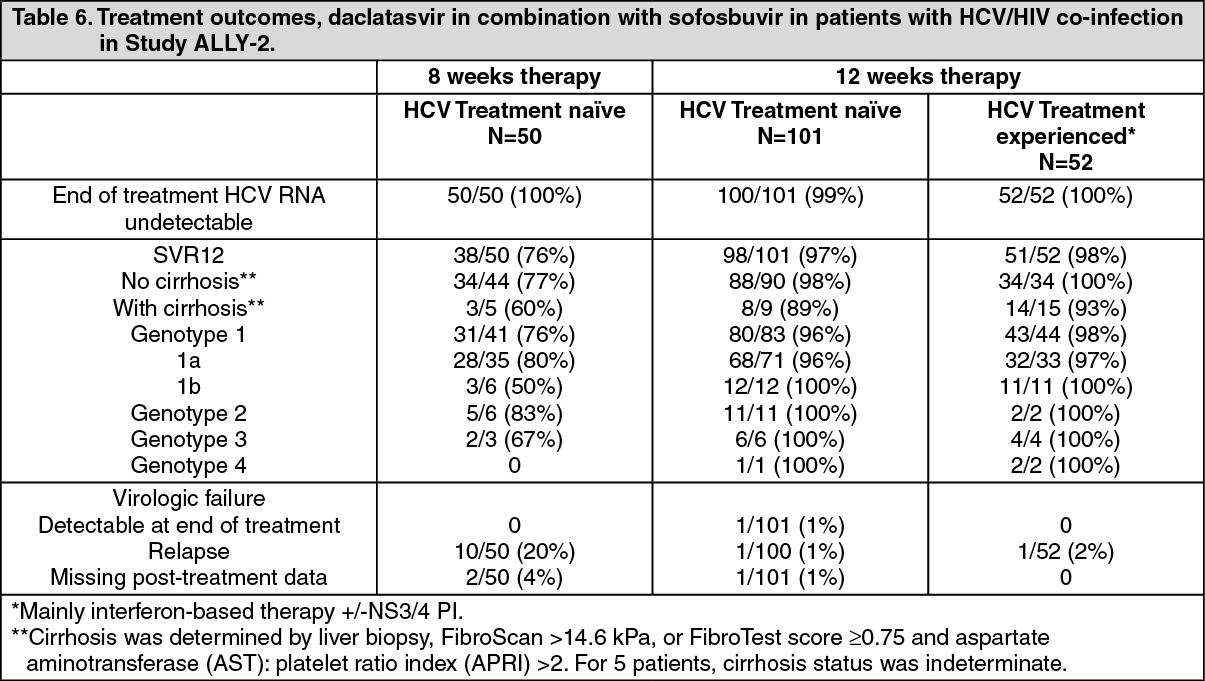 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image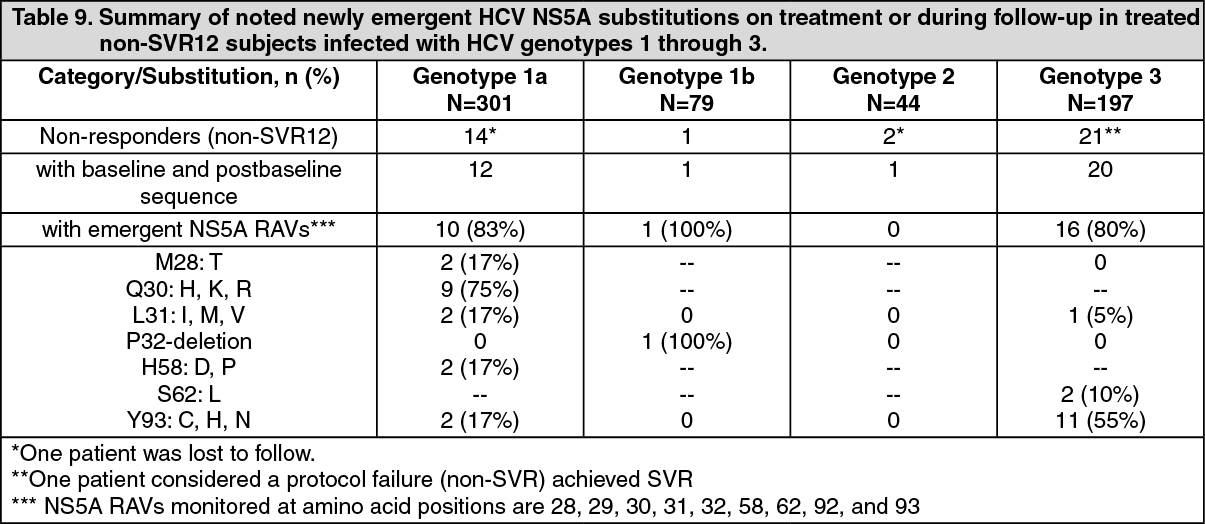 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
