


 Sign Out
Sign Out

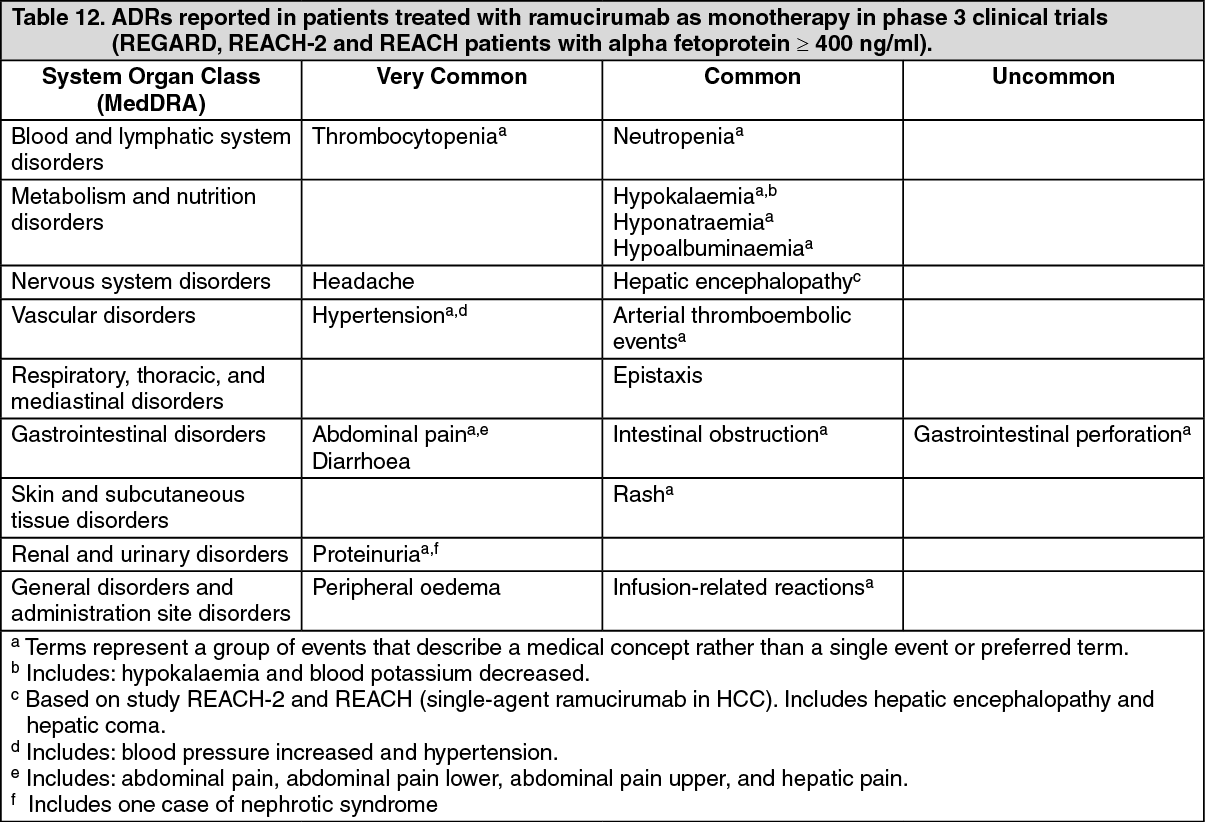
The most common adverse reactions observed in patients treated with ramucirumab as monotherapy are: peripheral oedema, hypertension, diarrhea, abdominal pain, headache, proteinuria and thrombocytopenia.
The most common adverse reactions observed in patients treated with ramucirumab in combination with chemotherapy are: fatigue/asthenia, neutropenia, diarrhoea, epistaxis and stomatitis.
The most common adverse reactions observed in patients treated with ramucirumab in combination with erlotinib are: infections, diarrhoea, hypertension, stomatitis, proteinuria, alopecia and epistaxis.
Tabulated list of adverse reactions: Tables 12 and 13 as follows list the adverse drug reactions (ADRs) from placebo controlled phase III clinical trials associated with ramucirumab used either as a monotherapy treatment for gastric cancer and HCC or in combination with different chemotherapy regimens or erlotinib for the treatment of gastric cancer, mCRC and NSCLC. ADRs are listed as follows by MedDRA body system organ class.
The following convention has been used for classification of frequency for ADR tables: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1/1,000), Very rare (<1/10,000), Not known (cannot be estimated from the available data).
Within each frequency grouping, ADRs are presented in order of decreasing seriousness. (See Tables 12 and 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image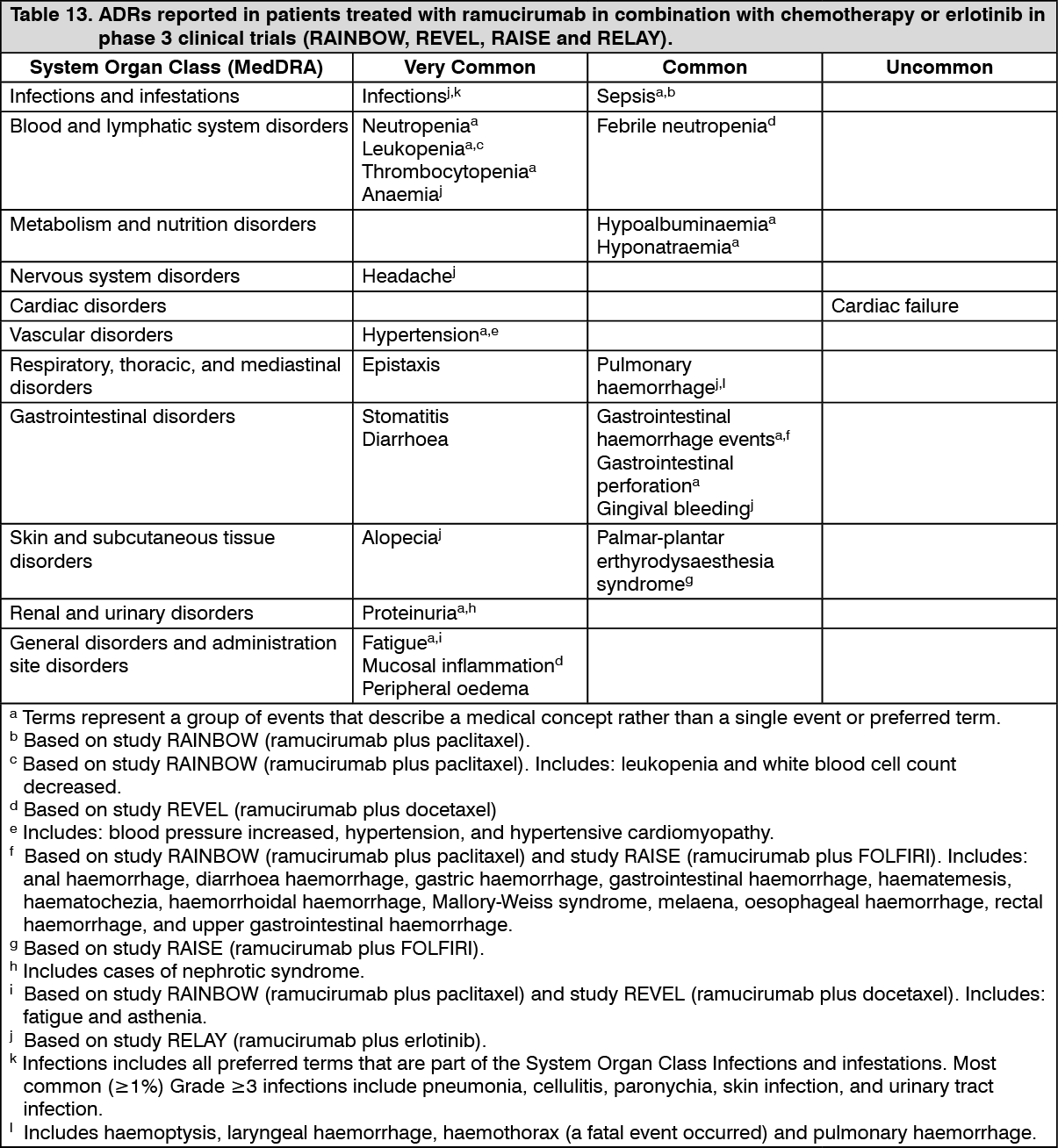 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageClinically relevant reactions (including Grade ≥3) associated with antiangiogenic therapy observed in ramucirumab-treated patients across clinical studies were: gastrointestinal perforations, infusion-related reactions and proteinuria (see Dosage & Administration and Precautions).
Colorectal cancer: Ramucirumab in combination with FOLFIRI: In the RAISE study, in mCRC patients treated with ramucirumab plus FOLFIRI, the most frequent (≥1%) ADR that led to the discontinuation of ramucirumab was proteinuria (1.5%). The most frequent (≥1%) ADRs leading to discontinuation of one or more components of FOLFIRI were: neutropenia (12.5%), thrombocytopenia (4.2%), diarrhoea (2.3%) and stomatitis (2.3%). The most frequent component of FOLFIRI to be discontinued was the 5-FU bolus.
Adverse reactions from other sources: (see Table 14).
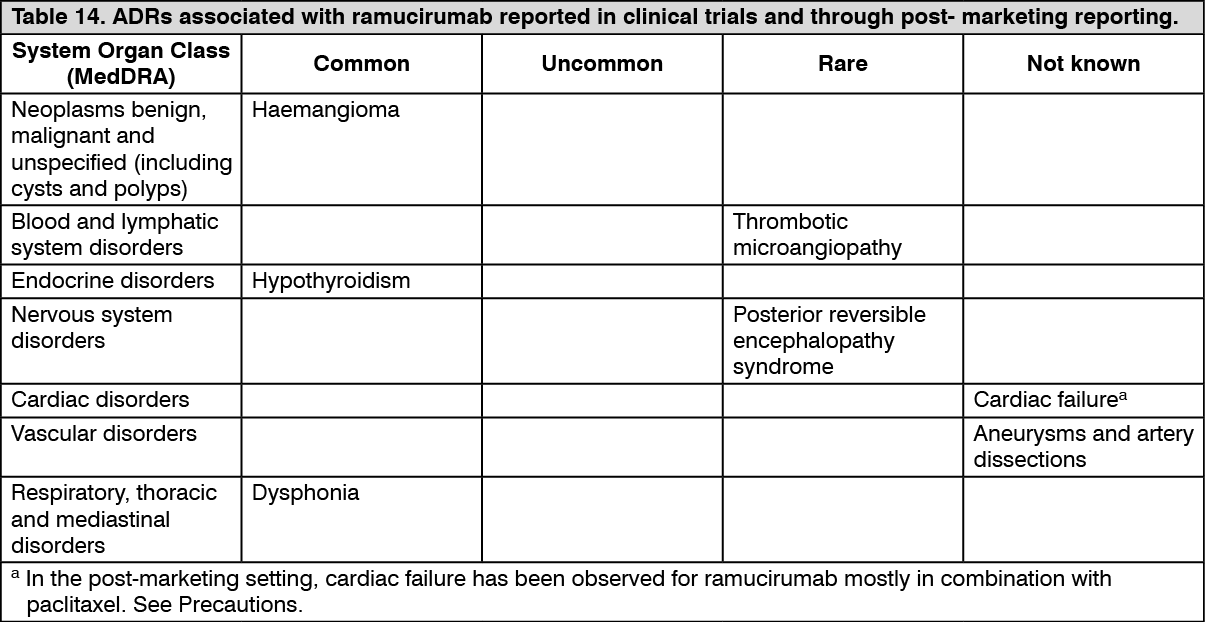 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePaediatric population: No new safety concerns were identified based on the limited number of paediatric patients treated with ramucirumab monotherapy in study I4T-MC-JVDA (see Pharmacology: Pharmacodynamics under Actions). One patient in this study had progressive widening of distal femoral growth plate. The impact of this finding on growth is not known.
View ADR Monitoring Form