Alprostadil 20 micrograms. When reconstituted, each 1 ml delivers a dose of 20 micrograms of alprostadil.
Excipient with known effect: Each 1 ml of reconstituted solution contains 8.4 mg of benzyl alcohol, equivalent to 8.4 mg/ml.
Pharmaceutical form after reconstitution: injectable solution.
Way of administration: intracavernosal.
Excipients/Inactive Ingredients: lactose monohydrate, sodium citrate, α-cyclodextrine, hydrochloric acid for pH adjustment, sodium hydroxide for pH adjustment.
Pharmacotherapeutic group: Drugs used in erectile dysfunction. ATC code: G04B E01.
Pharmacology: Pharmacodynamics: Alprostadil is present in various mammalian tissues and fluids. It has a diverse pharmacologic profile, among which some of its more important effects are vasodilation, inhibition of platelet aggregation, inhibition of gastric secretion, and stimulation of intestinal and uterine smooth muscle. The pharmacologic effect of alprostadil in the treatment of erectile dysfunction is presumed to be mediated by inhibition of alpha1- adrenergic activity in penile tissue and by its relaxing effect on cavernosal smooth muscle.
Pharmacokinetics: Following intracavernous injection of 20 micrograms of alprostadil, mean peripheral levels of alprostadil at 30 and 60 minutes after injection are not significantly greater than baseline levels of endogenous PGE1. Peripheral levels of the major circulating metabolite, 15-oxo-13,14-dihydro-PGE1, increase to reach a peak 30 minutes after injection and return to pre-dose levels by 60 minutes after injection. Any alprostadil entering the systemic circulation from the corpus cavernosum will be rapidly metabolized. Following intravenous administration, approximately 80% of the circulating alprostadil is metabolized in one pass through the lungs, primarily by beta- and omega-oxidation. The metabolites are excreted primarily by the kidney and excretion is essentially complete within 24 hours. There is no evidence of tissue retention of alprostadil or its metabolites following intravenous administration.
Toxicology: Preclinical Safety Data: No relevant information additional to that already contained in this monograph.
Alprostadil is indicated for the treatment of erectile dysfunction in adult males due to neurogenic, vasculogenic, psychogenic or mixed aetiology.
Alprostadil may be a useful adjunct to other diagnostic tests in the diagnosis of erectile dysfunction.
Alprostadil is administered by direct intracavernous injection. A half inch, 27 to 30 gauge needle is generally recommended. The dose of alprostadil should be individualised for each patient by careful titration under supervision by a physician.
The intracavernosal injection must be done under sterile conditions. The site of injection is usually along the dorsolateral aspect of the proximal third of the penis. Visible veins should be avoided. Both the side of the penis that is injected and the site of injection must be alternated; prior to the injection, the injection site must be cleansed with an alcohol swab.
To reconstitute alprostadil using the pre-filled diluent syringe: flip off the plastic cap from the vial, and use one of the swabs to wipe the rubber cap. Fit the 22 gauge needle to the syringe.
Inject the 1 ml of diluent into the vial, and shake to dissolve the powder entirely. Withdraw slightly more than the required dose of alprostadil solution, remove the 22 gauge needle, and fit the 30 gauge needle. Adjust volume to the required dose for injection. Following administration, any unused contents of the vial or syringe should be discarded.
A. As an aid to aetiologic diagnosis.
i) Subjects without evidence of neurological dysfunction; 20 micrograms alprostadil to be injected into the corpus cavernosum and massaged through the penis. Should an ensuing erection persist for more than one hour detumescent therapy (see Overdosage) should be employed prior to the subject leaving the clinic to prevent a risk of priapism.
Over 80% of subjects may be expected to respond to a single 20 micrograms dose of alprostadil. At the time of discharge from the clinic, the erection should have subsided entirely and the penis must be in a completely flaccid state.
ii) Subjects with evidence of neurological dysfunction; these patients can be expected to respond to lower doses of alprostadil. In subjects with erectile dysfunction caused by neurologic disease/trauma the dose for diagnostic testing must not exceed 10 micrograms and an initial dose of 5 micrograms is likely to be appropriate. Should an ensuing erection persist for more than one hour detumescent therapy (see Overdosage) should be employed prior to the subject leaving the clinic to prevent a risk of priapism. At the time of discharge from the clinic, the erection should have subsided entirely and the penis must be in a completely flaccid state.
B. Treatment: The initial dose of alprostadil in patients with erectile dysfunction of neurogenic origin secondary to spinal cord injury is 1.25 micrograms, with a second dose of 2.5 micrograms, a third of 5 micrograms, and subsequent incremental increases of 5 micrograms until an optimal dose is achieved. For erectile dysfunction of vasculogenic, psychogenic, or mixed aetiology, the initial dose is 2.5 micrograms. The second dose should be 5 micrograms if there is a partial response, and 7.5 micrograms if there is no response. Subsequent incremental increases of 5-10 micrograms should be given until an optimal dose is achieved. If there is no response to the administered dose, then the next higher dose may be given within 1 hour. If there is a response, there should be at least a 1-day interval before the next dose is given. The usual maximum recommended frequency of injection is no more than once daily and no more than three times weekly.
The first injections of alprostadil must be done by medically trained personnel. After proper training and instruction, alprostadil may be injected at home. If self-administration is planned, the physician should make an assessment of the patient's skill and competence with the procedure. It is recommended that patients are regularly monitored (e.g. every 3 months) particularly in the initial stages of self injection therapy when dose adjustments may be needed.
The dose that is selected for self-injection treatment should provide the patient with an erection that is satisfactory for sexual intercourse. It is recommended that the dose administered produces a duration of the erection not exceeding one hour. If the duration is longer, the dose should be reduced. The majority of patients achieve a satisfactory response with doses in the range of 5 to 20 micrograms. Doses of greater than 60 micrograms of alprostadil are not recommended. The lowest effective dose should be used.
The pharmacotoxic signs of alprostadil are similar in all animal species and include depression, soft stools or diarrhoea and rapid breathing. In animals, the lowest acute LD50 was 12 mg/kg which is 12,000 times greater than the maximum recommended human dose of 60 micrograms.
In man, prolonged erection and/or priapism are known to occur following intracavernous administration of vasoactive substances, including alprostadil. Patients should be instructed to report to a physician any erection lasting for a prolonged time period, such as 4 hours or longer.
Overdosage was not observed in clinical trials with alprostadil. If intracavernous overdose of alprostadil occurs, the patient should be placed under medical supervision until any systemic effects have resolved and/or until penile detumescence has occurred. Symptomatic treatment of any systemic symptoms would be appropriate.
The treatment of priapism (prolonged erection) should not be delayed more than 6 hours. Initial therapy should be by penile aspiration. Using aseptic technique, insert a 19-21 gauge butterfly needle into the corpus cavernosum and aspirate 20-50 ml of blood. This may detumesce the penis. If necessary, the procedure may be repeated on the opposite side of the penis until a total of up to 100 ml blood has been aspirated. If still unsuccessful, intracavernous injection of alpha-adrenergic medication is recommended. Although the usual contra-indication to intrapenile administration of a vasoconstrictor does not apply in the treatment of priapism, caution is advised when this option is exercised. Blood pressure and pulse should be continuously monitored during the procedure. Extreme caution is required in patients with coronary heart disease, uncontrolled hypertension, cerebral ischaemia, and in subjects taking monoamine oxidase inhibitors. In the latter case, facilities should be available to manage a hypertensive crisis. A 200 microgram/ml solution of phenylephrine should be prepared, and 0.5 to 1.0 ml of the solution injected every 5 to 10 minutes. Alternatively, a 20 microgram/ml solution of adrenaline should be used. If necessary, this may be followed by further aspiration of blood through the same butterfly needle. The maximum dose of phenylephrine should be 1 mg, or adrenaline 100 micrograms (5 ml of the solution). As an alternative metaraminol may be used, but it should be noted that fatal hypertensive crises have been reported. If this still fails to resolve the priapism, urgent surgical referral for further management, which may include a shunt procedure, is required.
Alprostadil should not be used in patients who have a known hypersensitivity to any of the constituents of the product; in patients who have conditions that might predispose them to priapism, such as sickle cell anaemia or trait, multiple myeloma, or leukaemia; or in patients with anatomical deformation of the penis, such as angulation, cavernosal fibrosis, or Peyronie's disease. Patients with penile implants should not be treated with alprostadil.
Alprostadil should not be used in men for whom sexual activity is inadvisable or contraindicated.
Prolonged erection and/or priapism may occur following intracavernosal administration of alprostadil. To minimize the risk, select the lowest effective dose. Patients should be instructed to report immediately to a physician, or if unavailable to seek immediate medical assistance for any erection lasting for a prolonged time period, such as 4 hours. Treatment of priapism should not be delayed more than 6 hours (see Overdosage) and should be according to established medical practice.
Painful erection is more likely to occur in patients with anatomical deformations of the penis, such as angulation, phimosis, cavernosal fibrosis, Peyronie's disease or plaques. Penile fibrosis, including angulation, cavernosal fibrosis, fibrotic nodules and Peyronie's disease may occur following the intracavernosal administration of alprostadil. The occurrence of fibrosis may increase with increased duration of use. Regular follow-up of patients, with careful examination of the penis, is strongly recommended to detect signs of penile fibrosis or Peyronie's disease. Treatment with alprostadil should be discontinued in patients who develop penile angulation, cavernosal fibrosis, or Peyronie's disease.
Patients on anticoagulants such as warfarin or heparin may have increased propensity for bleeding after the intracavernosal injection.
Underlying treatable medical causes of erectile dysfunction should be diagnosed and treated prior to initiation of therapy with alprostadil.
Use of intracavernosal alprostadil offers no protection from the transmission of sexually transmitted diseases. Individuals who use alprostadil should be counselled about the protective measures that are necessary to guard against the spread of sexually transmitted diseases, including the human immunodeficiency virus (HIV). In some patients, injection of alprostadil can induce a small amount of bleeding at the site of injection. In patients infected with blood-borne diseases, this could increase the transmission of such diseases to their partner.
Alprostadil should be used with caution in patients with cardiovascular and cerebrovascular risk factors. Alprostadil should be used with caution in patients who have experienced transient ischaemic attacks or those with unstable cardiovascular disorders.
Sexual stimulation and intercourse can lead to cardiac and pulmonary events in patients with coronary heart disease, congestive heart failure or pulmonary disease. These patients when using alprostadil should engage in sexual activity with caution.
Alprostadil is not intended for co-administration with any other agent for the treatment of erectile dysfunction (see Interactions).
The potential for abuse of alprostadil should be considered in patients with a history of psychiatric disorder or addiction.
Alprostadil uses a superfine needle for administration. As with all superfine needles, the possibility of needle breakage exists.
Needle breakage, with a portion of the needle remaining in the penis, has been reported and, in some cases, required hospitalisation and surgical removal.
Careful patient instruction in proper handling and injection techniques may minimise the potential for needle breakage.
The patient should be instructed that, if the needle is bent, it must not be used; they should also not attempt to straighten a bent needle. They should remove the needle from the syringe, discard it, and attach a new, unused sterile needle to the syringe.
Reconstituted solutions of alprostadil are intended for single use only, they should be used immediately and not stored. The syringe and any remaining solution should be properly discarded.
Excipient information: Benzyl alcohol: Caverject contains benzyl alcohol, which may cause hypersensitivity reactions.
The combined daily metabolic load of benzyl alcohol from all sources should be considered, especially in patients with liver or kidney impairment because of the risk of accumulation and toxicity (metabolic acidosis).
This medicine is only indicated for intracavernosal injection. Intravenous administration of the preservative benzyl alcohol has been associated with serious adverse events and death in paediatric patients including neonates ("gasping syndrome"). The minimum amount of benzyl alcohol at which toxicity may occur is not known.
Premature and low-birth weight infants may be more likely to develop toxicity. Caverject is not indicated for paediatric use.
Sodium: This medicinal product contains less than 1 mmol sodium (23 mg) per dose, that is to say essentially 'sodium free'.
Effects on Ability to Drive and Use Machines: Alprostadil would not be expected to have an influence on the ability to drive or operate machines.
Fertility, Pregnancy and Lactation: Not applicable.
(High doses of alprostadil (0.5 to 2.0 mg/kg subcutaneously) had an adverse effect on the reproductive potential of male rats, although this was not seen with lower doses (0.05 to 0.2 mg/kg). Alprostadil did not affect rat spermatogenesis at doses 200 times greater than the proposed human intrapenile dose.)
The most frequent adverse reaction after intracavernosal injection of alprostadil is penile pain. Thirty percent of the patients reported penile pain at least once; however, this event was associated with only 11% of the administered injections. In the majority of the cases, penile pain was rated mild or moderate in intensity. 3% of patients discontinued treatment because of penile pain.
Prolonged erection (defined as an erection that lasts for 4 to 6 hours) after intracavernosal administration of alprostadil was reported in 4% of patients. The frequency of priapism (defined as an erection that lasts 6 hours or longer) was 0.4%. In the majority of cases, spontaneous detumescence occurred.
Penile fibrosis, including angulation, fibrotic nodules and Peyronie's disease was reported in 3% of clinical trial patients overall, however, in one self-injection study in which the duration of use was up to 18 months, the incidence of penile fibrosis was higher, approximately 8%.
Haematoma and ecchymosis at the site of injection, which is related to the injection technique rather than to the effects of alprostadil, occurred in 3% and 2% of patients, respectively. Penile oedema or rash was reported by 1% of alprostadil treated patients.
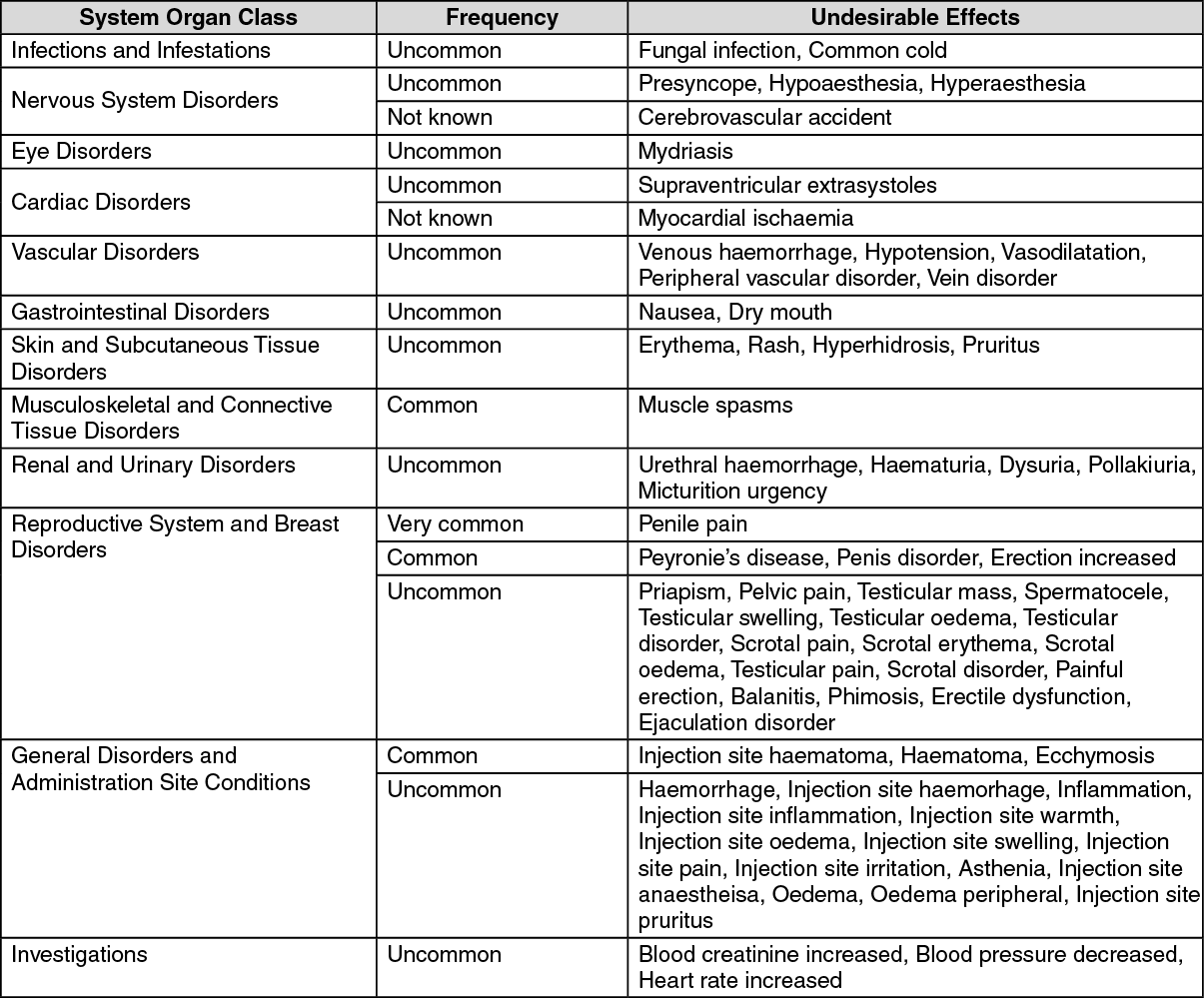
Adverse drug reactions reported during clinical trials and post-marketing experience are presented in the table as follows, frequencies are very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); not known (cannot be estimated from the available data). The adverse drug reactions are listed in order of decreasing medical seriousness within each frequency category and system organ class. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The effects of combinations of alprostadil with other treatments for erectile dysfunction (e.g. sildenafil) or other drugs inducing erection (e.g. papaverine) have not been formally studied. Such agents should not be used in combination with alprostadil due to the potential for inducing prolonged erections.
Sympathomimetics may reduce the effect of alprostadil. Alprostadil may enhance the effects of antihypertensives, vasodilative agents, anticoagulants and platelet aggregation inhibitors.
Incompatibilities: Alprostadil is not intended to be mixed or co-administered with any other products.
The presence of benzyl alcohol in the reconstitution vehicle decreases the degree of binding to package surfaces. Therefore, a more consistent product/delivery is produced when bacteriostatic water for injection containing benzyl alcohol is used.
Use immediately after reconstitution.
Instructions for Use and Handling: Always take this medicine exactly as described in this monograph or as your doctor, pharmacist or nurse has told you. Check with your doctor, pharmacist or nurse if you are not sure. A doctor or nurse will show you how to do the injection for at least the first time. Do not try to do it yourself until you have learnt the correct way or if you can't remember what to do, see your trainer again. These instructions are a reminder only. Keep the antiseptic swab away from the eyes.
How much Alprostadil should you inject: Different people need different amounts of alprostadil to treat erectile dysfunction. Your doctor will advise on the right dose for you and monitor you regularly to check how it is working. The starting dose is 1.25 - 2.5 micrograms.
Most men find that a dose of 5 - 20 micrograms is right for them, however, some men may require a higher dose. To minimise the risk of prolonged painful erection, your doctor will select the lowest effective dose. You should never use more than 60 micrograms. If alprostadil is being used to find the reason for your erectile dysfunction, the dose will be 5 - 20 micrograms.
If the dose that has been prescribed for you does not work well enough, tell your doctor. Do not change your dose unless your doctor tells you to. If you forget how much to use, read the label on the pack or speak to your doctor.
You and your partner: You may like your partner to be involved in preparing and/or giving the injection. If so, you should speak to your doctor about training for your partner. Wash your hands. Dry them on a clean towel. If your partner wishes to be involved in preparing or giving the injection, they should wash their hands too.
1. Check your pack: Make sure that the vial is the correct strength and the expiry date is still valid. The vial, syringe and needles all have protective covers. The flip-off cap on the vial can rotate; this is normal. Check that all the covers are on firmly and if they are not on properly, do not use them - take the whole pack back to your pharmacist. There are two needles in the pack: The larger 22 gauge needle with the grey end is used to mix the solution and alprostadil Powder; The smaller and finer 30 gauge needle with the yellow end is used to inject the mixture into your penis.
If a needle is bent do not use it.
2. To prepare the vial: Flip the plastic cap off the vial. Wipe the rubbery top with one of the wet antiseptic pads
3. Fitting the needle to the syringe: Hold the syringe and twist the white tamper evident cap to break the seal. Take the foil off the larger needle, (22 gauge) with the grey end, keeping the cover on. Join the needle to the syringe by turning the needle clockwise tightly onto the syringe, then remove the needle cover by pushing it away from the syringe with your thumb and forefinger.
4. Mixing the solution with the powder: Push the needle through the rubbery middle of the vial top. Press the plunger down firmly to squirt all the solution onto the powder. Gently swirl the vial until all the powder has dissolved. If the mixture is cloudy or does not dissolve completely, do not use it. Never use tap water or any liquid other than the one supplied in the syringe.
5. Filling the syringe: With the needle still inserted, turn the vial upside down. The needle should support the vial unaided. Make sure the needle tip is underneath the level of the liquid. Gently pull the plunger to draw all the mixture into the syringe. Pull the needle out of the vial.
6. Changing to the injecting needle: Gently twist the larger needle anticlockwise off the syringe. Remove the smaller injecting needle, (30 gauge) with the yellow end from its package, keeping the cover on. Twist the needle clockwise tightly onto the syringe, then remove the needle cover by pushing it away from the syringe with your thumb and forefinger.
7. Setting the dose: Tap the syringe gently to send any air bubbles to the top, then push the plunger to squeeze the air bubbles out, ensuring that at least one drop of solution comes out of the needle. Continue pushing until the plunger is exactly at the right mark for your dose. Your doctor will have shown you where this is.
How do you do the injection: Get undressed and make yourself comfortable. Take some time to relax yourself. If your prescriber has recommended use of the second antiseptic pad, open it now.
Make sure that the injection needle is not bent. A bent and re-straightened needle is more likely to break. Needle breakage, with a portion of the needle remaining in the penis, has been reported and, in some cases, required hospitalisation and surgical removal. If the needle is bent, do not use it and throw it away. Do not attempt to straighten it out. Attach a new, unused sterile needle to the syringe.
Take hold of the penis from the front, with the first two fingers underneath close to the testicles and the thumb on top. Gently squeeze the penis between your thumb and finger so that the injection site bulges out. If there is a foreskin on the penis, make sure it is stretched. The injection will go into the part of the penis.
If recommended by your prescriber wipe the skin over this area with the second pad and let it dry.
Keeping a firm grip on the penis and taking the syringe in your free hand, push the needle straight through the skin all the way into the bulgy part avoiding veins or other obvious blood vessels. Push the plunger firmly and if the alprostadil does not come out fairly easily, move the needle slightly and try again. Do not force the alprostadil liquid from the syringe.
Pull the needle out. On the needle mark, press gently with the pad or your thumb, as recommended by your prescriber. Massage the penis to help the alprostadil spread through it.
Do not keep any mixture in the syringe to use for a second injection.
How to throw away the syringe and needle safely: Ensure that the syringe, vial and needles are disposed of in a closed, puncture-resistant container, such as a sharps bin. Ask your doctor or pharmacist for instructions on how to properly dispose of the container after use if you are at all unsure.
How often can you use Alprostadil: Do not use alprostadil more than once in 24 hours or more than three times in a week. Change the exact place and side of the penis that you inject alprostadil each time you use it.
Your erection after injecting Alprostadil: It will take a little while for your erection to come on after the injection. With the right dose of alprostadil, your erection should be strong enough for you and your partner to enjoy lovemaking. Usually, your erection should not last longer than an hour. If you would like it to last longer, talk to your doctor. If your erection lasts longer than four hours you should seek medical advice (see Adverse Reactions).
What if you use too much Alprostadil: Tell your doctor straight away as you may need treatment, particularly if you experience an erection that lasts for longer than four hours.
If you have any further questions on the use of this medicine, ask your doctor, pharmacist or nurse.
G04BE01 - alprostadil ; Belongs to the class of drugs used in erectile dysfunction.
Caverject powd for inj 20 mcg
1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
