Each Caliberi Orodispersible Film 5mg contains 5mg tadalafil.
Each Caliberi Orodispersible Film 20mg contains 20mg tadalafil.
Excipients/Inactive Ingredients: Hydroxypropyl cellulose, Xanthan gum, Glycerin, Polyethylene glycol 400, Mannitol, Simethicone emulsion (30%), Titanium dioxide, Polysorbate 80, Sucralose, Ferric oxide-yellow, Ferric oxide-red, Vanilla flavor and Purified Water.
Pharmacotherapeutic Group: Urologicals, Drugs used in erectile dysfunction. ATC code: G04BE08.
Pharmacology: Pharmacodynamics: Mechanism of action: Tadalafil is a selective, reversible inhibitor of cyclic guanosine monophosphate (cGMP)-specific phosphodiesterase type 5 (PDE5). When sexual stimulation causes the local release of nitric oxide, inhibition of PDE5 by tadalafil produces increased levels of cGMP in the corpus cavernosum. This results in smooth muscle relaxation and inflow of blood into the penile tissues, thereby producing an erection. Tadalafil has no effect in the treatment of erectile dysfunction in the absence of sexual stimulation.
Tadalafil 5 mg - The effect of PDE5 inhibition on cGMP concentration in the corpus cavernosum is also observed in the smooth muscle of the prostate, the bladder and their vascular supply. The resulting vascular relaxation increases blood perfusion which may be the mechanism by which symptoms of benign prostatic hyperplasia are reduced. These vascular effects may be complemented by inhibition of bladder afferent nerve activity and smooth muscle relaxation of the prostate and bladder.
Pharmacodynamic effects: Tadalafil is a selective inhibitor of PDE5. PDE5 is an enzyme found in corpus cavernosum smooth muscle, vascular and visceral smooth muscle, skeletal muscle, platelets, kidney, lung, and cerebellum. The effect of tadalafil is more potent on PDE5 than on other phosphodiesterases. Tadalafil is >10,000-fold more potent for PDE5 than for PDE1, PDE2, and PDE4 enzymes which are found in the heart, brain, blood vessels, liver, and other organs. Tadalafil is >10,000fold more potent for PDE5 than for PDE3, an enzyme found in the heart and blood vessels. This selectivity for PDE5 over PDE3 is important because PDE3 is an enzyme involved in cardiac contractility. Additionally, tadalafil is approximately 700-fold more potent for PDE5 than for PDE6, an enzyme which is found in the retina and is responsible for phototransduction. Tadalafil is also >10,000-fold more potent for PDE5 than for PDE7 through PDE10.
Clinical efficacy and safety: Tadalafil administered to healthy subjects produced no significant difference compared to placebo in supine systolic and diastolic blood pressure (mean maximal decrease of 1.6/0.8mmHg, respectively), in standing systolic and diastolic blood pressure (mean maximal decrease of 0.2/4.6mmHg, respectively), and no significant change in heart rate.
The effects of tadalafil on vision showed no impairment of colour discrimination (blue/green) was detected using the Farnsworth-Munsell 100-hue test. This finding is consistent with the low affinity of tadalafil for PDE6 compared to PDE5. Based on the published studies, reports of changes in colour vision were rare (<0.1%).
Published data observed decreased in sperm count and concentration related to tadalafil treatment of unlikely clinical relevance while assessing the potential effect on spermatogenesis of Tadalafil 10mg (one 6-month study) and 20mg (one 6-month and one 9-month study) administered daily. These effects were not associated with changes in other parameters, such as motility, morphology, and FSH.
Erectile dysfunction: Published studies conducted on 1054 patients in an at-home setting to define the period of responsiveness to tadalafil on demand. Tadalafil demonstrated statistically significant improvement in erectile function and the ability to have successful sexual intercourse up to 36 hours following dosing, as well as patients' ability to attain and maintain erections for successful intercourse compared to placebo as early as 16 minutes following dosing.
In a published study performed in 186 patients (142 tadalafil, 44 placebo) for 12 weeks with erectile dysfunction secondary to spinal cord injury, tadalafil significantly improved the erectile function leading to a mean per subject proportion of successful attempts in patients treated with tadalafil 10 or 20 mg (flexible-dose, on demand) of 48% as compared to 17% with placebo.
Tadalafil at doses of 2 to 100mg has been evaluated in 16 published studies involving 3250 patients, including patients with erectile dysfunction of various severities (mild, moderate, severe), etiologies, ages (range 2186 years), and ethnicities. Most patients reported erectile dysfunction of at least 1 year in duration. In the primary efficacy studies of general populations, 81% of patients reported that tadalafil improved their erections as compared to 35% with placebo. Also, patients with erectile dysfunction in all severity categories reported improved erections whilst taking tadafil (86%, 83%, and 72% for mild, moderate, and severe, respectively, as compared to 45%, 42%, and 19% with placebo). Also, 75% of intercourse attempts were successful in tadafil-treated patients as compared to 32% with placebo.
For once-a-day evaluation of tadalafil at doses of 2.5, 5, and 10 mg published studies conducted on 853 patients of various ages (range 21-82 years) and ethnicities, with erectile dysfunction of various severities (mild, moderate, severe) and etiologies. The mean per-subject proportion of successful intercourse attempts on general population were 57 and 67% on Tadalafil 5mg, 50% on Tadalafil 2.5mg as compared to 31 and 37% with placebo. The mean per subject proportion of successful attempts in patients with erectile dysfunction secondary to diabetes were 41 and 46% on Tadalafil 5mg and 2.5mg, respectively, as compared to 28% with placebo. Most patients in these three studies were responders to previous on-demand treatment with PDE5 inhibitors. In a subsequent published data, 217 patients who were treatment-naive to PDE5 inhibitors were randomised to Tadalafil 5mg once a day vs. placebo. The mean per-subject proportion of successful sexual intercourse attempts was 68% for Tadalafil patients compared to 52% for patients on placebo.
Pharmacokinetics: Absorption: Tadalafil is readily absorbed after oral administration and the mean maximum observed plasma concentration (Cmax) is achieved at a median time of 2 hours after dosing. Absolute bioavailability of tadalafil following oral dosing has not been determined.
The rate and extent of absorption of tadalafil are not influenced by food, thus Caliberi may be taken without food. The time of dosing (morning versus evening) had no clinically relevant effects on the rate and extent of absorption.
Distribution: The mean volume of distribution is approximately 63 l, indicating that tadalafil is distributed into tissues. At therapeutic concentrations, 4% of tadalafil in plasma is bound to proteins. Protein binding is not affected by impaired renal function.
Less than 0.0005% of the administered dose appeared in the semen of healthy subjects.
Biotransformation: Tadalafil is predominantly metabolised by the cytochrome P450 (CYP) 3A4 isoform. The major circulating metabolite is the methylcatechol glucuronide. This metabolite is at least 13,000-fold less potent than tadalafil for PDE5. Consequently, it is not expected to be clinically active at observed metabolite concentrations.
Elimination: The mean oral clearance for tadalafil is 2.5 l/h and the mean half-life is 17.5 hours in healthy subjects. Tadalafil is excreted predominantly as inactive metabolites, mainly in the faeces (approximately 61% of the dose) and to a lesser extent in the urine (approximately 36% of the dose).
Linearity/Non-Linearity: Tadalafil pharmacokinetics in healthy subjects is linear with respect to time and dose. Over a dose range of 2.5 to 20 mg, exposure (AUC) increases proportionally with dose. Steady-state plasma concentrations are attained within 5 days of once daily dosing.
Pharmacokinetics determined with a population approach in patients with erectile dysfunction is similar to pharmacokinetics in subjects without erectile dysfunction.
Special Populations: Elderly: Healthy elderly subjects (65 years or over) had a lower oral clearance of tadalafil, resulting in 25% higher exposure (AUC) relative to healthy subjects aged 19 to 45 years. This effect of age is not clinically significant and does not warrant a dose adjustment.
Renal Insufficiency: Tadalafil exposure (AUC) approximately doubled in subjects with mild (creatinine clearance 51 to 80 ml/min) or moderate (creatinine clearance 31 to 50 ml/min) renal impairment and in subjects with end-stage renal disease on dialysis. In haemodialysis patients, Cmax was 41% higher than that observed in healthy subjects. Haemodialysis contributes negligibly to tadalafil elimination.
Hepatic Insufficiency: Tadalafil exposure (AUC) in subjects with mild and moderate hepatic impairment (Child-Pugh class A and B) is comparable to exposure in healthy subjects when a dose of 10 mg is administered. There is limited published clinical data on the safety of Tadalafil in patients with severe hepatic insufficiency (Child-Pugh class C). If Tadalafil is prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. There are no available published data about the administration of once-a-day dosing of tadalafil to patients with hepatic impairment. If Tadalafil is prescribed once-a-day, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. There are no available published data about the administration of doses higher than 10 mg of tadalafil to patients with hepatic impairment.
Patients with Diabetes: Tadalafil exposure (AUC) in patients with diabetes was approximately 19% lower than the AUC value for healthy subjects. This difference in exposure does not warrant a dose adjustment.
Toxicity: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, and toxicity to reproduction.
There was no evidence of teratogenicity, embryotoxicity, or foetotoxicity in rats or mice that received up to 1000 mg/kg/day tadalafil. In a rat prenatal and postnatal development study, the no observed effect dose was 30 mg/kg/day. In the pregnant rat the AUC for calculated free drug at this dose was approximately 18 times the human AUC at a 20 mg dose.
There was no impairment of fertility in male and female rats. In dogs given tadalafil daily for 6 to 12 months at doses of 25 mg/kg/day (resulting in at least a 3-fold greater exposure [range 3.7-18.6] than seen in humans given a single 20 mg dose) and above, there was regression of the seminiferous tubular epithelium that resulted in a decrease in spermatogenesis in some dogs. See also Pharmacodynamics as previously mentioned.
Caliberi Orodispersible Film (ODF) 5mg and 20mg: Treatment of erectile dysfunction (ED) in adult males.
In order for tadalafil to be effective for the treatment of erectile dysfunction, sexual stimulation is required.
Caliberi Orodispersible Film (ODF) 5mg: Treatment of the signs and symptoms of benign prostatic hyperplasia in adult males.
Caliberi is not indicated for use by women.
Posology: Caliberi Orodispersible Film (ODF) 5mg and 20mg: Erectile dysfunction (ED): Adult men: In general, the recommended dose is 10 mg (2 ODF × 5mg) taken prior to anticipated sexual activity without food.
In those patients in whom tadalafil 10 mg (2 ODF × 5mg) does not produce an adequate effect, 20 mg might be tried. It may be taken at least 30 minutes prior to sexual activity.
The maximum dose frequency is once per day.
Tadalafil 10mg (2 ODF X 5mg) and 20 mg is intended for use prior to anticipated sexual activity and it is not recommended for continuous daily use.
In patients who anticipate a frequent use of Caliberi (i.e., at least twice weekly) a once daily regimen with the lowest doses of Caliberi might be considered suitable, based on patient choice and the physician's judgement.
In these patients the recommended dose is 5 mg taken once a day at approximately the same time of day.
The appropriateness of continued use of the daily regimen should be reassessed periodically.
Caliberi Orodispersible Film (ODF) 5mg: Benign prostatic hyperplasia in adult men: The recommended dose is 5mg taken at approximately the same time every day without food. For adult men being treated for both benign prostatic hyperplasia and erectile dysfunction the recommended dose is also 5mg taken at approximately the same time every day. Patients who are unable to tolerate tadalafil 5mg or the treatment of benign prostatic hyperplasia should consider an alternative therapy.
Special Populations: Elderly patients: Dosage adjustments are not required in elderly patients.
Men with renal impairment: Dose adjustments are not required in patients with mild to moderate renal impairment. For patients with severe renal impairment 10 mg (2 ODF × 5mg) is the maximum recommended dose.
Once-a-day dosing of 5mg tadalafil both for the treatment of erectile dysfunction or benign prostatic hyperplasia is not recommended in patients with severe renal impairment (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Men with hepatic impairment: The recommended dose of Caliberi is 10 mg (2 ODF x 5 mg) taken prior to anticipated sexual activity without food. There is limited clinical data on the safety of Caliberi in patients with severe hepatic impairment (Child-Pugh Class C); if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. There are no available data about the administration of doses higher than 10 mg (2 ODF x 5 mg) of tadalafil to patients with hepatic impairment.
Once-a-day dosing has not been evaluated in patients with hepatic impairment; therefore, if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician (see Precautions and Pharmacology: Pharmacodynamics under Actions).
Men with Diabetes: Dosage adjustments are not required in patients with diabetes.
Pediatric population: There is no relevant use of Caliberi in the paediatric population with regard to the treatment of erectile dysfunction.
Method of administration: 1. Open the sachet from top.
2. Roll down the back side of the sachet. The patient can see a thin film edge after rolling down.
3. Pull the film edge and remove the thin film from the sachet and place it immediately on the tongue. Allow it to dissolve without water.
Single doses of up to 500 mg have been given to healthy subjects, and multiple daily doses up to 100 mg have been given to patients. Adverse events were similar to those seen at lower doses.
In cases of overdose, standard supportive measures should be adopted, as required. Haemodialysis contributes negligibly to tadalafil elimination.
Hypersensitivity to the active substance or to any of the excipients listed in Description.
In published studies, tadalafil was shown to augment the hypotensive effects of nitrates. This is thought to result from the combined effects of nitrates and tadalafil on the nitric oxide/cGMP pathway. Therefore, administration of Caliberi to patients who are using any form of organic nitrate is contraindicated (see Interactions).
Caliberi must not be used in men with cardiac disease for whom sexual activity is inadvisable. Physicians should consider the potential cardiac risk of sexual activity in patients with pre-existing cardiovascular disease.
The following groups of patients with cardiovascular disease were not included in clinical trials and the use of tadalafil is therefore contraindicated: patients with myocardial infarction within the last 90 days, patients with unstable angina or angina occurring during sexual intercourse, patients with New York Heart Association Class 2 or greater heart failure in the last 6 months, patients with uncontrolled arrhythmias, hypotension (<90/50 mm Hg), or uncontrolled hypertension, patients with a stroke within the last 6 months.
Caliberi is contraindicated in patients who have loss of vision in one eye because of non-arteritic anterior ischaemic optic neuropathy (NAION), regardless of whether this episode was in connection or not with previous PDE5 inhibitor exposure (see Precautions).
The co-administration of PDE5 inhibitors, including tadalafil, with guanylate cyclase stimulators, such as riociguat, is contraindicated as it may potentially lead to symptomatic hypotension (see Interactions).
Before treatment with Caliberi: A medical history and physical examination should be undertaken to diagnose erectile dysfunction and determine potential underlying causes, before pharmacological treatment is considered.
Prior to initiating any treatment for erectile dysfunction, physicians should consider the cardiovascular status of their patients, since there is a degree of cardiac risk associated with sexual activity. Tadalafil has vasodilator properties, resulting in mild and transient decreases in blood pressure (see Pharmacology: Pharmacodynamics under Actions) and as such potentiates the hypotensive effect of nitrates (see Contraindications).
The evaluation of erectile dysfunction should include a determination of potential underlying causes and the identification of appropriate treatment following an appropriate medical assessment. It is not known if tadalafil is effective in patients who have undergone pelvic surgery or radical non-nerve-sparing prostatectomy.
Cardiovascular: Serious cardiovascular events, including myocardial infarction, sudden cardiac death, unstable angina pectoris, ventricular arrhythmia, stroke, transient ischaemic attacks, chest pain, palpitations and tachycardia, have been reported either post marketing. Most of the patients in whom these events have been reported had pre-existing cardiovascular risk factors. However, it is not possible to definitively determine whether these events are related directly to these risk factors, to tadalafil, to sexual activity, or to a combination of these or other factors.
In patients who are taking alpha1 blockers, concomitant administration of tadalafil may lead to symptomatic hypotension in some patients (see Interactions). The combination of tadalafil and doxazosin is not recommended.
Vision: Visual defects and cases of NAION have been reported in connection with the intake of tadalafil and other PDE5 inhibitors. Analyses of observational data suggest an increased risk of acute NAION in men with erectile dysfunction following exposure to tadalafil or other PDE5 inhibitors. As this may be relevant for all patients exposed to tadalafil, the patient should be advised that in case of sudden visual defect, he should stop taking tadalafil and consult a physician immediately (see Contraindications).
Decreased or sudden hearing loss: Cases of sudden hearing loss have been reported after the use of tadalafil. Although other risk factors were present in some cases (such as age, diabetes, hypertension and previous hearing loss history) patients should be advised to stop taking tadalafil and seek prompt medical attention in the event of sudden decrease or loss of hearing.
Priapism and anatomical deformation of the penis: Patients who experience erections lasting 4 hours or more should be instructed to seek immediate medical assistance. If priapism is not treated immediately, penile tissue damage and permanent loss of potency may result.
Tadalafil, should be used with caution in patients with anatomical deformation of the penis (such as angulation, cavernosal fibrosis, or Peyronie's disease) or in patients who have conditions which may predispose them to priapism (such as sickle cell anaemia, multiple myeloma or leukaemia).
Use of CYP3A4 inhibitors: Caution should be exercised when prescribing tadalafil to patients using potent CYP3A4 inhibitors (ritonavir, saquinavir, ketoconazole, itraconazole, and erythromycin), as increased tadalafil exposure (AUC) has been observed if the medicinal products are combined (see Interactions).
Caliberi and other treatments for erectile dysfunction: The safety and efficacy of combinations of tadalafil and other PDE5 inhibitors or other treatments for erectile dysfunction have not been studied. The patients should be informed not to take tadalafil in such combinations.
Effects on ability to drive and use machines: Caliberi has negligible influence on the ability to drive or use machines. However, patients should be aware of how they react to Caliberi before driving or using machines.
Hepatic impairment: There is limited published clinical data on the safety of single-dose administration of tadalafil in patients with severe hepatic insufficiency (Child-Pugh Class C). If tadalafil is prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician.
Caliberi is not indicated for use by women.
Pregnancy: There are limited published data from the use of tadalafil in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development, parturition or postnatal development (see Pharmacology: Toxicology: Preclinical safety data under Actions). As a precautionary measure, it is preferable to avoid the use of Caliberi during pregnancy.
Breastfeeding: Available pharmacodynamic/toxicological data in animals have shown excretion of tadalafil in milk. A risk to the suckling child cannot be excluded. Caliberi should not be used during breast feeding.
Fertility: Effects were seen in dogs that might indicate impairment of fertility. However, it is suggested that this effect is unlikely in humans, although a decrease in sperm concentration was seen in some men (see Pharmacology: Pharmacodynamics and Toxicology: Preclinical safety data under Actions).
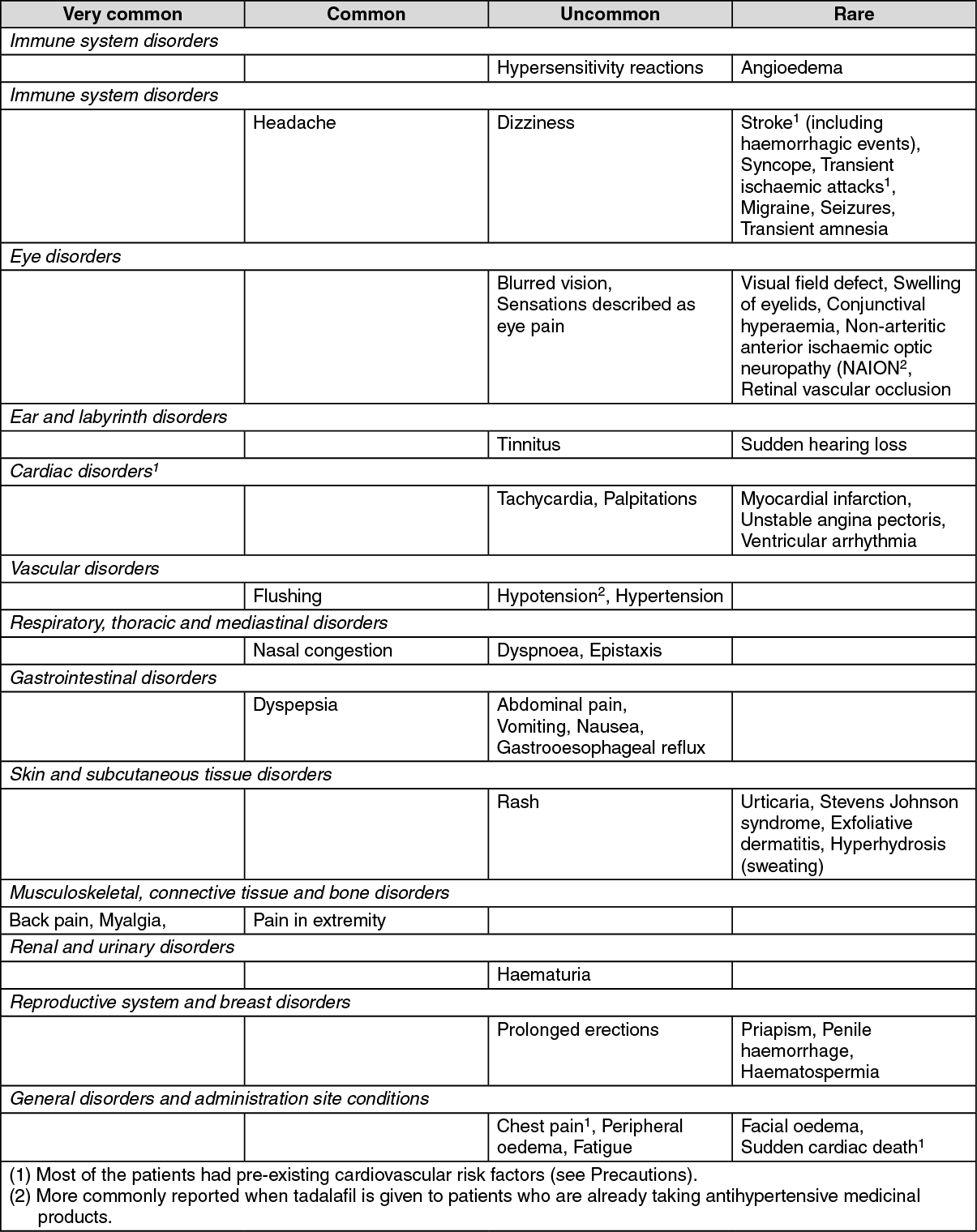
Summary of the safety profile Caliberi: The most commonly reported adverse reactions in patients taking tadalafil for the treatment of erectile dysfunction or benign prostatic hyperplasia were headache, dyspepsia, back pain and myalgia, in which the incidences increase with increasing dose of tadalafil. The adverse reactions reported were transient, and generally mild or moderate. The majority of headaches reported with tadalafil once-a-day dosing are experienced within the first 10 to 30 days of starting treatment.
Tabulated summary of adverse reactions: The table as follows lists the adverse reactions from published data for on-demand and once-a-day treatment of erectile dysfunction and the once-a-day treatment of benign prostatic hyperplasia. (See table.)
 Click on icon to see table/diagram/image
Description of selected adverse reactions:
Click on icon to see table/diagram/image
Description of selected adverse reactions: A slightly higher incidence of ECG abnormalities, primarily sinus bradycardia, has been reported in patients treated with tadalafil once a day as compared with placebo. Most of these ECG abnormalities were not associated with adverse reactions.
Other special populations: Published data showed diarrhoea was reported more frequently in patients over 65 years of age whereas dizziness and diarrhea were reported more frequently in patients over 75 years of age with tadalafil 5mg taken ocnce a day for the treatment of benign prostatic hyperplasia.
Effects of Other Substances on Tadalafil: Cytochrome P450 inhibitors: Tadalafil is principally metabolised by CYP3A4. A selective inhibitor of CYP3A4, ketoconazole (200 mg daily), increased tadalafil (10 mg) exposure (AUC) 2-fold and Cmax by 15%, relative to the AUC and Cmax values for tadalafil alone. Ketoconazole (400 mg daily) increased tadalafil (20 mg) exposure (AUC) 4-fold and Cmax by 22%. Ritonavir, a protease inhibitor (200 mg twice daily), which is an inhibitor of CYP3A4, CYP2C9, CYP2C19, and CYP2D6, increased tadalafil (20 mg) exposure (AUC) 2-fold with no change in Cmax. Although specific interactions have not been studied, other protease inhibitors, such as saquinavir, and other CYP3A4 inhibitors, such as erythromycin, clarithromycin, itraconazole, and grapefruit juice, should be co-administered with caution, as they would be expected to increase plasma concentrations of tadalafil (see Precautions). Consequently, the incidence of the adverse reactions listed in section 4.8 might be increased.
Transporters: The role of transporters (for example, p-glycoprotein) in the disposition of tadalafil is not known. Therefore, there is the potential of drug interactions mediated by inhibition of transporters.
Cytochrome P450 inducers: A CYP3A4 inducer, rifampicin, reduced tadalafil AUC by 88%, relative to the AUC values for tadalafil alone (10 mg). This reduced exposure can be anticipated to decrease the efficacy of tadalafil; the magnitude of decreased efficacy is unknown. Other inducers of CYP3A4, such as phenobarbital, phenytoin, and carbamazepine, may also decrease plasma concentrations of tadalafil.
Effects of Tadalafil on Other Medicinal Products: Nitrates: In published clinical studies, tadalafil (5, 10 and 20 mg) was shown to augment the hypotensive effects of nitrates. Therefore, administration of tadalafil to patients who are using any form of organic nitrate is contraindicated (see Contraindications). Based on the results of a published clinical study in which 150 subjects receiving daily doses of tadalafil 20 mg for 7 days and 0.4 mg sublingual nitroglycerin at various times, this interaction lasted for more than 24 hours and was no longer detectable when 48 hours had elapsed after the last tadalafil dose. Thus, in a patient prescribed any dose of tadalafil (5 mg- 20 mg), where nitrate administration is deemed medically necessary in a life-threatening situation, at least 48 hours should have elapsed after the last dose of tadalafil before nitrate administration is considered. In such circumstances, nitrates should only be administered under close medical supervision with appropriate haemodynamic monitoring.
Anti-hypertensives (including calcium channel blockers): The co-administration of doxazosin (4 and 8 mg daily) and tadalafil (5 mg daily dose and 20 mg as a single dose) increases the blood pressure-lowering effect of this alpha-blocker in a significant manner. This effect lasts at least twelve hours and may be symptomatic, including syncope. Therefore, this combination is not recommended (see Precautions).
There were no reported effects with alfuzosin or tamsulosin. However, caution should be exercised when using tadalafil in patients treated with any alphablockers, and notably in the elderly. Treatments should be initiated at minimal dosage and progressively adjusted.
In clinical pharmacology studies, the potential for tadalafil to augment the hypotensive effects of antihypertensive medicinal products was examined. Tadalafil showed no interaction with major classes of antihypertensive medicinal products were studied, including calcium-channel blockers (amlodipine), angiotensin converting enzyme (ACE) inhibitors (enalapril), beta-adrenergic receptor blockers (metoprolol), thiazide diuretics (bendrofluazide), and angiotensin II receptor blockers (various types and doses, alone or in combination with thiazides, calcium-channel blockers, beta-blockers, and/or alpha-blockers). In another published study, tadalafil (20 mg) was studied in combination with up to 4 classes of antihypertensives. In subjects taking multiple antihypertensives, the ambulatory-blood-pressure changes appeared to relate to the degree of blood pressure control. In this regard, study subjects whose blood pressure was well controlled, the reduction was minimal and similar to that seen in healthy subjects. In study subjects whose blood pressure was not controlled, the reduction was greater, although this reduction was not associated with hypotensive symptoms in the majority of subjects. In patients receiving concomitant antihypertensive medicinal products, tadalafil 20 mg may induce a blood pressure decrease.
There was no difference in adverse events in patients taking tadalafil with or without antihypertensive medicinal products. However, appropriate clinical advice should be given to patients regarding a possible decrease in blood pressure when they are treated with antihypertensive medicinal products.
Riociguat: Preclinical studies showed an additive systemic blood pressure lowering effect when PDE5 inhibitors were combined with riociguat. In clinical studies, riociguat has been shown to augment the hypotensive effects of PDE5 inhibitors. There was no evidence of favourable clinical effect of the combination in the population studied. Concomitant use of riociguat with PDE5 inhibitors, including tadalafil, is contraindicated (see Contraindications).
5-alpha reductase inhibitors: In a published clinical trial that compared tadalafil 5 mg coadministered with finasteride 5 mg to placebo plus finasteride 5 mg in the relief of BPH symptoms, no new adverse reactions were identified. However, as a formal drug-drug interaction study evaluating the effects of tadalafil and 5-alpha reductase inhibitors (5ARIs) has not been performed, caution should be exercised when tadalafil is co-administered with 5ARIs.
CYP1A2 substrates (e.g. theophylline): When tadalafil 10 mg was administered with theophylline (a non-selective phosphodiesterase inhibitor) in a clinical pharmacology study, there was no pharmacokinetic interaction. The only pharmacodynamic effect was a small (3.5 bpm) increase in heart rate. Caution should be exercised when co-administering these medicinal products.
Ethinylestradiol and terbutaline: Tadalafil has been demonstrated to produce an increase in the oral bioavailability of ethinylestradiol; a similar increase may be expected with oral administration of terbutaline, although the clinical consequence of this is uncertain.
Alcohol: Alcohol concentrations (mean maximum blood concentration 0.08%) were not affected by coadministration with tadalafil (10 mg or 20 mg). In addition, no changes in tadalafil concentrations were seen 3 hours after coadministration with alcohol. Alcohol was administered in a manner to maximise the rate of alcohol absorption (overnight fast with no food until 2 hours after alcohol). Tadalafil (20 mg) did not augment the mean blood pressure decrease produced by alcohol (0.7 g/kg or approximately 180 ml of 40% alcohol [vodka] in an 80 kg male) but postural dizziness and orthostatic hypotension were observed. When tadalafil was administered with lower doses of alcohol (0.6 g/kg), hypotension was not observed and dizziness occurred with similar frequency to alcohol alone. The effect of alcohol on cognitive function was not augmented by tadalafil (10 mg).
Cytochrome P450 metabolised medicinal products: Tadalafil is not expected to cause inhibition or induction of the clearance of medicinal products metabolised by CYP450 isoforms as tadalafil does not inhibit or induce CYP450 isoforms, including CYP3A4, CYP1A2, CYP2D6, CYP2E1, CYP2C9 and CYP2C19.
CYP2C9 substrates (e.g. R-warfarin): Tadalafil (10 mg and 20 mg) had no effect on exposure (AUC) to S-warfarin or R-warfarin (CYP2C9 substrate), nor did tadalafil affect changes in prothrombin time induced by warfarin.
Aspirin: Tadalafil (10 mg and 20 mg) did not potentiate the increase in bleeding time caused by acetylsalicylic acid.
Antidiabetic medicinal products: Specific interaction studies with antidiabetic medicinal products were not conducted.
Incompatibilities: Not applicable.
Special precautions for disposal and other handling: No special requirements.
Store in the original package in order to protect from moisture. Store below 30°C.
Shelf life: 3 years.
G04BE08 - tadalafil ; Belongs to the class of drugs used in erectile dysfunction.
Caliberi orodispersible film 20 mg
2 × 1's
Caliberi orodispersible film 5 mg
15 × 1's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
