


 Sign Out
Sign Out

The use of CHCs is associated with an increased risk of various serious diseases such as myocardial infarction, thrombo-embolism, stroke, or hepatic neoplasms. Other risk factors such as hypertension, hyperlipidaemia, obesity and diabetes distinctly increase the morbidity and mortality risk.
If any of the conditions or risk factors mentioned as follows is present, the suitability of Belara should be discussed with the woman.
In the event of aggravation, or first appearance of any of these conditions or risk factors, the woman should be advised to contact the doctor to determine whether the use of Belara should be discontinued.
Thrombo-embolism and other vascular diseases: Results from epidemiological studies show that there is a connection between the administration of hormonal contraceptives and an increased risk of venous or arterial thrombo-embolic diseases, e.g. myocardial infarction, apoplexy, deep-vein thrombosis and pulmonary embolism. These events are rare. Extremely rarely, thrombosis has been reported to occur in CHC users in other blood vessels, e.g. hepatic, mesenteric, renal or retinal veins and arteries.
Risk of venous thromboembolism (VTE): The use of any combined hormonal contraceptive (CHC) increases the risk of venous thromboembolism (VTE) compared with no use. Products that contain levonorgestrel, norgestimate or norethisterone are associated with the lowest risk of VTE. It is not yet known how the risk with Belara compares with these lower risk products. The decision to use any product other than one known to have the lowest VTE risk should be taken only after a discussion with the woman to ensure that the patient understands the risk of VTE with Belara, how the current risk factors influence this risk, and that the VTE risk is highest in the first ever year of use. There is also some evidence that the risk is increased when a CHC is re-started after a break in use of 4 weeks or more.
In women who do not use a CHC and are not pregnant about 2 out of 10,000 will develop a VTE over the period of one year. However, in any individual woman the risk may be far higher, depending on the underlying risk factors (see as follows).
Epidemiological studies in women who use low dose combined hormonal contraceptives (<50 μg ethinylestradiol) have found that out of 10,000 women between about 6 and 12 will develop a VTE in one year.
Out of 10,000 women who use a levonorgestrel-containing CHC about 61 will develop a VTE in one year.
It is not yet known how the risk with chlormadinone-containing CHCs compares with the risk with levonorgestrel-containing CHCs.
The number of VTEs per year with low dose CHCs is fewer than the numbers expected in women during pregnancy or in the postpartum period.
VTE may be fatal in 1-2% of cases.
1 Mid-point of range of 5-7 per 10,000 WY, based on a relative risk for CHCs containing levonorgestrel versus non-use of approximately 2.3 to 3.6.
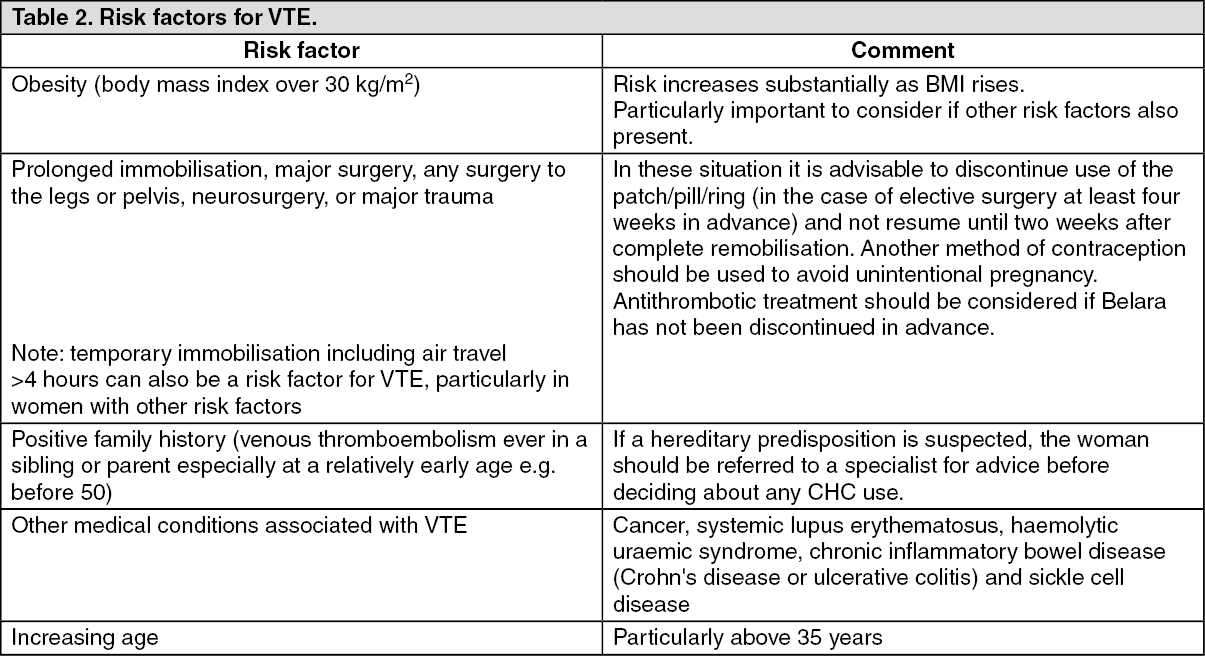
Risk factors for VTE: The risk for venous thromboembolic complications in CHC users may increase substantially in a women with additional risk factors, particularly if there are multiple risk factors (see Table 2).
Belara is contraindicated if a woman has multiple risk factors that put the patient at high risk of venous thrombosis (see Contraindications). If a woman has more than one risk factor, it is possible that the increase in risk is greater than the sum of the individual factors - in this case the total risk of VTE should be considered. If the balance of benefits and risks is considered to be negative a CHC should not be prescribed (see Contraindications). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThere is no consensus about the possible role of varicose veins and superficial thrombophlebitis in the onset or progression of venous thrombosis.
The increased risk of thromboembolism in pregnancy, and particularly the 6 week period of the puerperium, must be considered (for information on "Fertility, pregnancy and lactation" see Use in Pregnancy & Lactation).
Symptoms of VTE (deep vein thrombosis and pulmonary embolism): In the event of symptoms women should be advised to seek urgent medical attention and to inform the healthcare professional that the patient is taking a CHC.
Symptoms of deep vein thrombosis (DVT) can include: unilateral swelling of the leg and/or foot or along a vein in the leg; pain or tenderness in the leg which may be felt only when standing or walking; increased warmth in the affected leg; red or discoloured skin on the leg.
Symptoms of pulmonary embolism (PE) can include: sudden onset of unexplained shortness of breath or rapid breathing; sudden coughing which may be associated with haemoptysis; sharp chest pain; severe light headedness or dizziness; rapid or irregular heartbeat.
Some of these symptoms (e.g. "shortness of breath", "coughing") are non-specific and might be misinterpreted as more common or less severe events (e.g. respiratory tract infections).
Other signs of vascular occlusion can include: sudden pain, swelling and slight blue discoloration of an extremity.
If the occlusion occurs in the eye symptoms can range from painless blurring of vision which can progress to loss of vision. Sometimes loss of vision can occur almost immediately.
Risk of arterial thromboembolism (ATE): Epidemiological studies have associated the use of CHCs with an increased risk for arterial thromboembolism (myocardial infarction) or for cerebrovascular accident (e.g. transient ischaemic attack, stroke). Arterial thromboembolic events may be fatal.
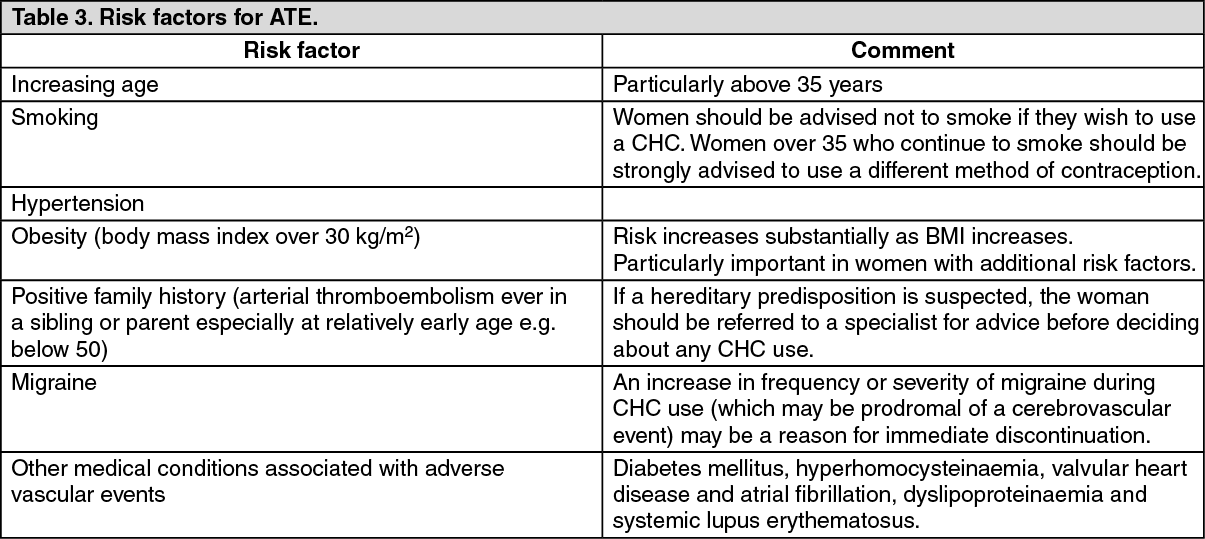
Risk factors for ATE: The risk of arterial thromboembolic complications or of a cerebrovascular accident in CHC users increases in women with risk factors (see Table 3). Belara is contraindicated if a woman has one serious or multiple risk factors for ATE that puts the patient at high risk of arterial thrombosis (see Contraindications). If a woman has more than one risk factor, it is possible that the increase in risk is greater than the sum of the individual factors - in this case the total risk should be considered. If the balance of benefits and risks is considered to be negative a CHC should not be prescribed (see Contraindications). (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSymptoms of ATE: In the event of symptoms women should be advised to seek urgent medical attention and to inform the healthcare professional that the patient is taking a CHC.
Symptoms of a cerebrovascular accident can include: sudden numbness or weakness of the face, arm or leg, especially on one side of the body; sudden trouble walking, dizziness, loss of balance or coordination; sudden confusion, trouble speaking or understanding; sudden trouble seeing in one or both eyes; sudden, severe or prolonged headache with no known cause; loss of consciousness or fainting with or without seizure.
Temporary symptoms suggest the event is a transient ischaemic attack (TIA).
Symptoms of myocardial infarction (MI) can include: pain, discomfort, pressure, heaviness, sensation of squeezing or fullness in the chest, arm, or below the breastbone; discomfort radiating to the back, jaw, throat, arm, stomach; feeling of being full, having indigestion or choking; sweating, nausea, vomiting or dizziness; extreme weakness, anxiety, or shortness of breath; rapid or irregular heartbeats.
CHC users must be informed that they must consult their physician in the event of presenting possible symptoms of thrombosis. Belara must be discontinued on suspicion or confirmation of thrombosis.
Tumours: Some epidemiological studies indicate that the long-term use of hormonal contraceptives is a risk factor for the development of cervical cancer in women infected with the human papilloma virus (HPV).
However, there is still controversy about the extent to which this finding is influenced by interfering factors (e.g. differences in the number of sexual partners or the use of mechanical contraceptive measures) (see also "Medical examination/consultation" as follows).
A meta-analysis from 54 epidemiological studies reported a slight increase of relative risk (RR = 1.24) of having breast cancer diagnosed in users of CHCs. The excess risk is transient, and disappears gradually during the course of 10 years after cessation of CHC use. These studies do not provide evidence for causation. The observed pattern of increased risk may be due to an earlier diagnosis of breast cancer in CHC users, the biological effects of CHCs or a combination of both.
In rare cases benign, and in even fewer cases malignant, liver tumours have been reported during the administration of hormonal contraceptives. In isolated cases these tumours have led to life-threatening intraabdominal haemorrhage. In the event of severe abdominal pain that does not recede spontaneously, hepatomegaly or signs of intra-abdominal haemorrhage the possibility of a liver tumour must be considered and Belara must be discontinued.
Other Diseases: Depressed mood and depression are well-known undesirable effects of hormonal contraceptive use (see Adverse Reactions). Depression can be serious and is a well-known risk factor for suicidal behaviour and suicide. Women should be advised to contact their physician in case of mood changes and depressive symptoms, including shortly after initiating the treatment.
Many women taking hormonal contraceptives had a slight increase in blood pressure; however a clinically significant increase is rare. The connection between the administration of hormonal contraceptives and clinically manifest hypertension has so far not been confirmed.
If there is a clinically significant increase in blood pressure during the administration of Belara, the use of the medicinal product must be discontinued and the hypertension must be treated. Belara can be continued as soon as blood pressure values have returned to normal on antihypertensive therapy.
Exogenous estrogens may induce or exacerbate symptoms of hereditary and acquired angioedema.
In women with a history of herpes gestationis there may be a recurrence during CHC administration.
In women with a history or familial history of hypertriglyceridaemia, the risk of pancreatitis is increased during CHC administration.
Acute or chronic disturbances of liver function may necessitate discontinuation of CHC use until the liver function values return to normal. Recurrence of cholestatic jaundice that occurred first during pregnancy or during previous use of sex hormones necessitates discontinuation of CHCs.
CHCs may affect peripheral insulin resistance or glucose tolerance. Therefore diabetics should be monitored carefully whilst taking hormonal contraceptives.
Uncommonly, chloasma may occur, particularly in women with a history of chloasma gravidarum.
Women with a tendency to develop chloasma should avoid exposure to the sun and ultraviolet radiation during the administration of hormonal contraceptives.
Precautions: The administration of estrogen or estrogen/progestogen combinations may have negative effects on certain diseases and/or conditions. Special medical supervision is necessary in: epilepsy; multiple sclerosis; tetany; migraine (see also Contraindications); asthma; cardiac or renal insufficiency; chorea minor; diabetes mellitus (see also Contraindications); liver diseases (see also Contraindications); dyslipoproteinaemia (see also Contraindications); auto-immune diseases (including systemic lupus erythematosus); obesity; hypertension (see also Contraindications); endometriosis; varicosis; phlebitis (see also Contraindications); blood coagulation disorders (see also Contraindications); mastopathy; uterine myoma; herpes gestationis; depression (see also Contraindications); chronic inflammatory bowel disease (Crohn's disease, ulcerative colitis; see also Adverse Reactions).
Medical examination/consultation: Prior to the initiation or reinstitution of Belara a complete medical history (including family history) should be taken and pregnancy must be ruled out. Blood pressure should be measured and a physical examination should be performed, guided by the contraindications (see Contraindications) and warnings (see previously mentioned).
It is important to draw a woman's attention to the information on venous and arterial thrombosis, including the risk of Belara compared with other CHCs, the symptoms of VTE and ATE, the known risk factors and what to do in the event of a suspected thrombosis.
The woman should also be instructed to carefully read the user leaflet and to adhere to the advice given. The frequency and nature of examinations should be based on established practice guidelines and be adapted to the individual woman.
Women should be advised that hormonal contraceptives do not protect against HIV infection (AIDS) and other sexually transmitted diseases.
Impaired efficacy: Failing to take a film-coated tablet (see "Irregular tablet administration" under Dosage & Administration), vomiting or intestinal disorders including diarrhoea, the long-term concomitant administration of certain medicinal products (see Interactions) or in very rare cases metabolic disorders may impair contraceptive efficacy.
The effect of the medicinal product on cycle control: Breakthrough bleeding and spotting: All hormonal contraceptives may cause irregular vaginal bleeding (breakthrough bleeding/spotting) particularly in the first few administration cycles. Therefore, a medical assessment of irregular cycles should only be made after an adjustment period of about three cycles. If during the administration of Belara breakthrough bleeding persists or occurs after previously regular cycles, an examination should be carried out to rule out pregnancy or an organ disorder. After pregnancy and an organ disorder have been ruled out, Belara may be continued or a switch may be made to another medicinal product.
Intracyclic bleeding may be a sign of impaired contraceptive efficacy (see "Irregular tablet administration", "Instructions in case of vomiting" under Dosage & Administration and Interactions).
Absence of withdrawal bleeding: After 21 days of administration withdrawal bleeding usually occurs. Occasionally and particularly in the first few months of administration withdrawal bleeding may be absent. However, this absence is not an indication of a reduced contraceptive effect. If bleeding is not present after one administration cycle during which a film-coated tablet was not forgotten, the tablet-free period of seven days was not extended, no other medicines were taken concomitantly, and there was no vomiting or diarrhoea, conception is unlikely and the administration of Belara can be continued. If Belara was not taken according to the instructions before the first absence of withdrawal bleeding or withdrawal bleeding does not occur in two consecutive cycles, pregnancy must be ruled out before continuing administration.
Herbal medicines containing St John's wort (Hypericum perforatum) should not be taken together with Belara (see Interactions).
ALT elevations: During clinical trials with patients treated for hepatitis C virus infections (HCV) with the medicinal products containing ombitasvir/paritaprevir/ritonavir and dasabuvir with or without ribavirin, transaminase (ALT) elevations higher than 5 times the upper limit of normal (ULN) occurred significantly more frequent in women using ethinylestradiol-containing medications such as combined hormonal contraceptives (CHCs). Additionally, also in patients treated with glecaprevir/pibrentasvir, ALT elevations were observed in women using ethinylestradiol-containing medications such as CHCs. Patients who are taking ethinylestradiol-containing medicinal products must switch to an alternative method of contraception (e.g. progestin only contraception or non-hormonal methods) prior to initiating ombitasvir/paritaprevir/ritonavir and dasubuvir therapy or glecaprevir/pibrentasvir (see Contraindications and Interactions).
This medicinal product contains lactose (as 69.5 mg lactose monohydrate per tablet).
Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Effects on ability to drive and use machines: Combined hormonal contraceptives are not known to have negative effects on the ability to drive or to operate machines.