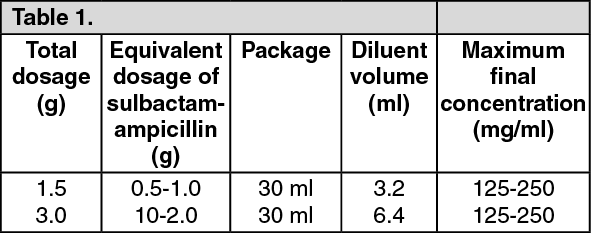
Sulbactam sodium/ampicillin sodium IM/IV can be administered by either intravenous or intramuscular routes. The following dilutions may be used: (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
For intravenous administration, sulbactam sodium/ampicillin sodium IM/IV should be reconstituted with sterile water for injection or any compatible solution. To ensure complete dissolution, allow foaming to dissipate in order to visually inspect. The dose can be given by bolus injection over a minimum of 3 minutes or can be used in greater dilutions as an intravenous infusion over 15-30 minutes.
Sulbactam sodium/ampicillin sodium parenteral may also be administered by deep intramuscular injection; if pain is experienced, 0.5% sterile solution for injection of lignocaine hydrochloride anhydrous may be used for reconstitution of the powder.
Use in Adults: The usual dosage range of sulbactam sodium/ampicillin sodium IM/IV is 1.5g to 12g per day in divided doses every 6 or 8 hours up to a maximum daily dosage of sulbactam of 4g. Less severe infections may be treated on an every 12 hours schedule. (See Table 2.)
Click on icon to see table/diagram/image
More or less frequent dosing may be indicated depending on the severity of the illness and the renal function of the patient. Treatment is usually continued until 48 hours after pyrexia and other abnormal signs have resolved. Treatment is normally given for 5 to 14 days, but the treatment period may be extended or additional ampicillin may be administered in severely ill cases.
In treating patients on restricted sodium intake, it should be noted that 1500mg of sulbactam sodium/ampicillin sodium IM/IV contains approximately 115mg (5mmol) of sodium.
For the prophylaxis of surgical infections, 1.5-3 g of sulbactam sodium/ampicillin sodium IM/IV should be given at induction of anesthesia, which allows sufficient time to achieve effective serum and tissue concentrations during the procedure. The dose may be repeated every 6-8 hours; administration is usually stopped 24 hours after the majority of surgical procedures, unless a therapeutic course of sulbactam sodium/ampicillin sodium IM/IV is indicated. In treatment of uncomplicated gonorrhea, sulbactam sodium/ampicillin sodium IM/IV can be given as a single dose of 1.5g. Concomitant probenecid 1.0g orally should be administered in order to prolong plasma concentrations of sulbactam and ampicillin.
Use in children, infants and neonates: The dosage of sulbactam sodium/ampicillin sodium IM/IV for most infections in children, infants and neonates is 150 mg/kg/day (corresponding to sulbactam 50 mg/kg/day and ampicillin 100 mg/kg/day).
In children, infants and neonates, dosing is usually every 6 to 8 hours in accordance with the usual practice for ampicillin.
In neonates during the first week of life (especially preterms), the recommended dose is 75 mg/kg/day (corresponding to 25 mg/kg/day sulbactam and 50 mg/kg/day ampicillin) in divided doses every 12 hours.
Use in patients with renal impairment: In patients with severe impairment of renal function (creatinine clearance ≤ 30 ml/min), the elimination kinetics of sulbactam and ampicillin are similarly affected and hence the plasma ratio of one to the other will remain constant. The dose of sulbactam sodium/ampicillin sodium IM/IV in such patients should be administered less frequently in accordance with the usual practice for ampicillin.
Directions for Reconstitution:
Intramuscular injection: 1.5 g strength should be reconstituted with 3.2 mL of diluent.
Diluents for Intramuscular Injection: Sterile water for injection, 0.5% Lidocaine Hydrochloride Injection, 2% Lidocaine Hydrochloride Injection.
Intravenous infusion: Primary diluent: Sterile water for injection.
1.5g strength should be reconstituted with 3.2 mL Primary diluent.
Secondary diluents for Intravenous infusion: The previously mentioned solutions are further diluted with one of the following secondary diluent: Sterile water for injection, 0.9% sodium chloride injection, 5% dextrose injection, Lactated Ringer's solution, 5% dextrose in 0.45% saline, 10% invert sugar.
Reconstitute the vial with one the diluents, shake well to get clear solution and use immediately.
Route of Administration: For Intramuscular and Intravenous.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image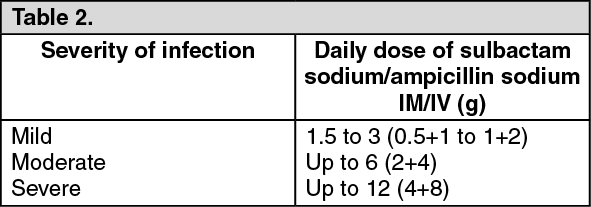 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
