The frequency and severity of adverse effects are generally similar between patients receiving paclitaxel for the treatment of ovarian, breast or lung cancer. None of the observed effects appear to be clearly influenced by age. When using alternative dosing regimens, the incidence of adverse reactions may be higher than reported as follows. Unless otherwise mentioned, the combination of paclitaxel with platinum agents did not result in any clinically relevant changes to the safety profile of single agent paclitaxel.
Adverse effects reported were those occurring during or following the first course of therapy, and have, where possible, been grouped by frequency according to the following criteria. Very common; Common; Uncommon; Rare; Very rare.
Cardiovascular: Very common: Hypotension.
Common: Bradycardia; ECG abnormalities (non-specific repolarisation and sinus tachycardia).
Uncommon: ECG abnormalities (premature beats), cardiomyopathy.
Rare: Myocardial infarction; congestive heart failure (typically in patients who have received other chemotherapy, notably anthracyclines).
Six severe cardiovascular events possibly related to paclitaxel administration occurred including asymptomatic ventricular tachycardia, tachycardia with bigeminy, atrioventricular block (2 patients), and syncopal episodes (2 patients - in one associated with severe hypotension and coronary stenosis resulting in death). Severe hypotensive reactions have been associated with serious hypersensitivity reactions and have required intervention. Cardiac failure and sinus bradycardia have also been observed.
Haematological: Very common: Myelosuppression, thrombocytopenia, leucopoenia, fever, bleeding, anaemia; neutropenia. Neutrophil nadirs are reported to occur at a median of 11 days after paclitaxel administration.
Common: Febrile neutropenia (associated with an infectious episode, including UTI and URTI).
Rare: Five septic episodes, which were associated with severe neutropenia attributable to paclitaxel administration had a fatal outcome.
Patients who have received prior radiation or cisplatin therapy exhibit more frequent myelosuppression, which is generally of greater severity (see Precautions and Interactions).
Hepatobiliary: Very common: Elevated alkaline phosphatase; elevated AST; elevated ALT.
Common: Elevated bilirubin.
Rare: Hepatic necrosis (leading to death); hepatic encephalopathy (leading to death).
Hypersensitivity: Very common: Flushing; rash.
Common: Dyspnoea; hypotension; chest pains; tachycardia.
Uncommon: Significant hypersensitivity reactions requiring therapy (e.g. Hypotension, angioneurotic oedema, bronchospasm, respiratory distress, generalised urticaria, oedema, backpains, pain in extremities, chills, diaphoresis).
Infections and Infestation: Very common: Infection.
Uncommon: Septic shock.
Gastrointestinal: Very common: Nausea; vomiting; diarrhoea; mucositis (These manifestations were usually mild to moderate at the recommended dose.)
Rare: Bowel perforation (There have been several cases of bowel perforation associated with patients receiving paclitaxel. Patients receiving paclitaxel who complain of abdominal pain with other signs and symptoms, should have bowel perforation excluded).
Neutropenic enterocolitis has been reported.
Vascular Disorders: Very common: Hypotension.
Uncommon: Hypertension, thrombosis, thrombophlebitis.
Musculoskeletal: Very common: Arthralgia; myalgia (The symptoms were usually transient occurring two to three days after paclitaxel administration and resolving within a few days.)
Neurological: Very common: Peripheral neuropathy (The incidence of peripheral neuropathy is dose dependent; neurologic symptoms may occur following the first course and may worsen in a high proportion of patients with increasing exposure. Severity of symptoms also increases with dose. Peripheral neuropathy has been reported as a cause of discontinuation in some patients taking paclitaxel, though sensory symptoms have usually improved or resolved within several months of paclitaxel discontinuation).
Rare: Optic nerve and/or visual disturbances (scintillating scotomata) particularly in patients who have received higher doses than recommended; these effects generally have been reversible; motor neuropathy with resultant minor distal weakness and autonomic neuropathy resulting in paralytic ileus and orthostatic hypotension.
Skin and Appendages: Very common: Alopecia.
Rare: Nail and skin changes (mild and transient); radiation-recall dermatitis; recall dermatitis.
Local: Phlebitis following intravenous administration has been reported. Extravasation leading to oedema, pain, erythema and induration has been reported. On occasions, extravasation can lead to cellulitis. Skin discolouration may also occur.
General Disorders and Administration Site Conditions: Common: Injection site reactions (including localised oedema, pain, erythema, induration, on occasion extravasation can result in cellulitis).
Injection site reactions, including reactions secondary to extravasation, were usually mild and consisted of erythema, tenderness, skin discolouration, or swelling at the injection site. These reactions have been observed more frequently with the 24 hour infusion than with the 3 hour infusion. Recurrence of skin reactions at a site of previous extravasation following administration of paclitaxel at a different site, i.e., 'recall', has been reported rarely.
Rare reports of more severe events such as phlebitis, cellulitis, induration, skin exfoliation, necrosis and fibrosis have been received as part of the continuing surveillance of paclitaxel safety. In some cases the onset of the injection site reaction either occurred during a prolonged infusion or was delayed by a week to ten days.
A specific treatment for extravasation reactions is unknown at this time. Given the possibility of extravasation, it is advisable to closely monitor the infusion site for possible infiltration during drug administration.
Radiation pneumonitis has been reported in patients receiving concurrent radiotherapy.
Post marketing Experience: The following additional adverse reactions have been identified during post approval use of paclitaxel. Because the reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a casual relationship to drug exposure.
Infections and Infestations: Pneumonia, sepsis.
Cardiac Disorders: Atrial fibrillations, supraventricular tachycardia, reduction of left ventricle ejection fraction, ventricular failure.
Haematological Disorders: Acute myeloid leukaemia, myelodysplastic syndrome.
Immune System Disorders: Anaphylactic reactions (with fatal outcome), anaphylactic shock, cross-hypersensitivity between ANZATAX and other taxanes has been reported.
Metabolism and Nutritional Disorders: Anorexia, tumour lysis syndrome.
Psychiatric Disorders: Confusion state.
Vascular Disorders: Shock.
Respiratory, Thoracic and Mediastinal Disorders: Dyspnoea, pleural effusion, respiratory failure, interstitial pneumonia, lung fibrosis, pulmonary embolism, cough.
Gastrointestinal Disorders: Bowel obstruction, bowel perforation, ischemic colitis, pancreatitis, mesenteric thrombosis, pseudomembranous, colitis, oesophagitis, constipation, ascites.
Neurological Disorders: Autonomic neuropathy (resulting in paralytic ileus and orthostatic hypotension), grand mal seizures, convulsions, encephalopathy, dizziness, headache, ataxia, paresthesia, hyperesthesia.
Eye Disorders: Photopsia, visual floaters cystoid macular oedema, macular oedema.
Ear and Labyrinth Disorders: Hearing loss, tinnitus, vertigo, ototoxicity.
Skin and Subcutaneous Tissue Disorders: Stevens-Johnson syndrome, epidermal necrolysis, erythema multiforme, exfoliative dermatitis, urticaria, onycholysis (patients on therapy should wear sun protection on hands and feet), pruritus, rash, erythema, phlebitis, cellulitis, skin exfoliation, necrosis, fibrosis, palmar-plantar erythrodysesthesia syndrome.
Musculoskeletal and Connective Tissue Disorders: Systemic lupus erythematosus, scleroderma.
Investigations: Increase in blood creatinine.
General Disorders and Administration Site Conditions: Asthenia, malaise, pyrexia, dehydration, oedema.


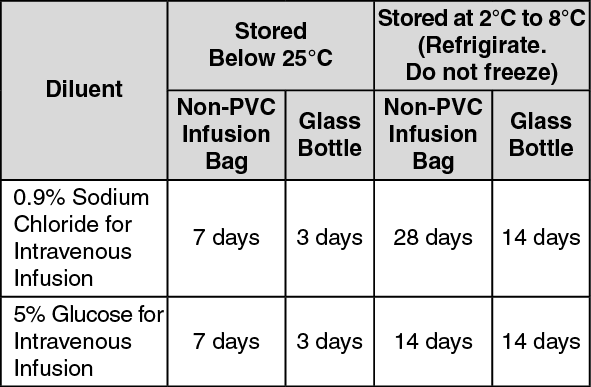 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
