


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Fentanyl is a potent μ-opioid analgesic with rapid onset of analgesia and short duration of action. Fentanyl is approximately 100-fold more potent than morphine as an analgesic. Secondary effects of fentanyl on central nervous system (CNS), respiratory and gastro-intestinal function are typical of opioid analgesics and are considered to be class effects. The analgesic effects of fentanyl are related to the blood level of the active substance; in opioid-naive patients, minimum effective analgesic serum concentrations of fentanyl range from 0.3-1.2 ng/ml, while blood levels of 10-20 ng/ml produce surgical anaesthesia and profound respiratory depression.
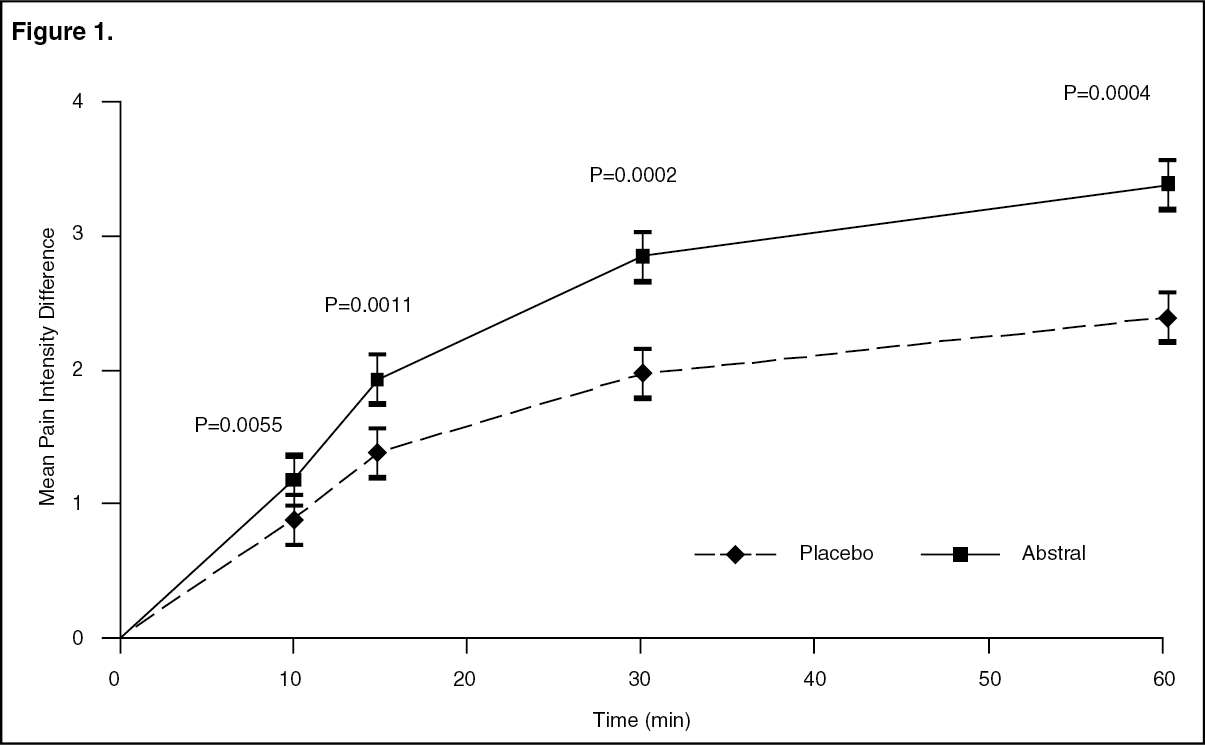
In patients with chronic cancer pain on stable maintenance doses of opioids, statistically significant improvement in pain intensity difference was seen with Abstral versus placebo from 10 minutes after administration onwards (see figure 1 as follows), with a significantly lower need for rescue analgesic therapy.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe safety and efficacy of Abstral have been evaluated in patients taking the drug at the onset of the breakthrough pain episode. Preemptive use of Abstral for predictable pain episodes was not investigated in the clinical trials.
Fentanyl, in common with all μ-opioid receptor agonists, produces dose dependent respiratory depression. This risk is higher in opioid-naive subjects than in patients experiencing severe pain or receiving chronic opioid therapy. Long-term treatment with opioids typically leads to development of tolerance to their secondary effects.
While opioids generally increase the tone of urinary tract smooth muscle, the net effect tends to be variable, in some cases producing urinary urgency, in others, difficulty in urination.
Opioids increase the tone and decrease the propulsive contractions of the smooth muscle of the gastrointestinal tract leading to a prolongation in gastrointestinal transit time, which may be responsible for the constipating effect of fentanyl.
Pharmacokinetics: Fentanyl is a highly lipophilic drug absorbed very rapidly through the oral mucosa and more slowly through the gastrointestinal tract. Orally administered fentanyl undergoes pronounced hepatic and intestinal first pass effects.
Abstral is a quick dissolving sublingual tablet formulation. Rapid absorption of fentanyl occurs over about 30 minutes following administration of Abstral. The absolute bioavailability of Abstral has been calculated to be 54 %. Mean maximal plasma concentrations of fentanyl range from 0.2 to 1.3 ng/ml (after administration of 100 to 800 μg Abstral) and are reached within 22.5 to 240 minutes.
About 80-85% of fentanyl is bound by plasma proteins, mainly α1-glycoprotein and to a lesser extent albumin and lipoprotein. The volume of distribution of fentanyl at steady state is about 3-6 l/kg.
Fentanyl is metabolised primarily via CYP3A4 to a number of pharmacologically inactive metabolites, including norfentanyl. Within 72 hours of intravenous fentanyl administration around 75% of the dose is excreted into the urine, mostly as metabolites, with less than 10% as unchanged drug. About 9% of the dose is recovered in the faeces, primarily as metabolites. Total plasma clearance of fentanyl is about 0.5 l/h/kg. After Abstral administration, the main elimination half-life of fentanyl is about 7 hours (range 3-12.5 hours) and the terminal half-life is about 20 hours (range 11.5-25 hours).
The pharmacokinetics of Abstral have been shown to be dose proportional over the dose range of 100 to 800 μg. Pharmacokinetic studies have shown that multiple tablets are bioequivalent to single tablets of the equivalent dose.
Renal/hepatic impairment: Impaired hepatic or renal function could cause increased serum concentrations. Older, cachectic or generally impaired patients may have a lower fentanyl clearance, which could cause a longer terminal half-life for the compound (see Dosage & Administration and Precautions).
Toxicology: Preclinical safety data: Safety pharmacology and repeated dose toxicity data reveal no special hazard for humans that is not already covered by other sections of this SPC. Animal studies have shown reduced fertility and increased mortality in rat foetuses. Teratogenic effects have, however, not been demonstrated.
Mutagenicity testing in bacteria and in rodents yielded negative results. Like other opioids fentanyl showed mutagenic effects in vitro in mammalian cells. A mutagenic risk with therapeutic use seems unlikely since effects were induced only at very high concentrations.
Carcinogenicity studies (26-week dermal alternative bioassay in Tg.AC transgenic mice; two-year subcutaneous carcinogenicity study in rats) with fentanyl did not reveal any findings indicative of oncogenic potential. Evaluation of brain slides from the carcinogenicity study in rats revealed brain lesions in animals administered high doses of fentanyl citrate. The relevance of these findings to humans is unknown.