Summary of the safety profile: In all clinical studies, 4896 subjects (all ages) received STAMARIL PASTEUR. In the most representative study in general population, the most frequently reported reactions (between 12% and 18% of subjects) were cephalalgia, asthenia, injection site pain and myalgia.
In the most representative study in toddler population, the most frequently reported reactions (between 32% and 35% of toddlers) were irritability, crying and appetite loss.
Adverse reactions usually occurred within the first three days following vaccination except fever, which occurred between Day 4 and Day 14.
These reactions usually lasted for not more than 3 days.
Both local and systemic reactions were usually of mild intensity; however at least one severe injection site reaction was reported in 0.8% of subjects in general population and in 0.3% of toddlers and at least one severe systemic reaction was reported in 1.4% of subjects in general population and 4.9% in toddlers.
Cases of serious adverse events such as severe hypersensitivity or anaphylactic reactions, neurotropic or viscerotropic disease (YEL-AND; YEL-AVD) have been reported from post-marketing experience (see Tabulated list of Adverse Reactions and Description of Selected Adverse Reactions as follows).
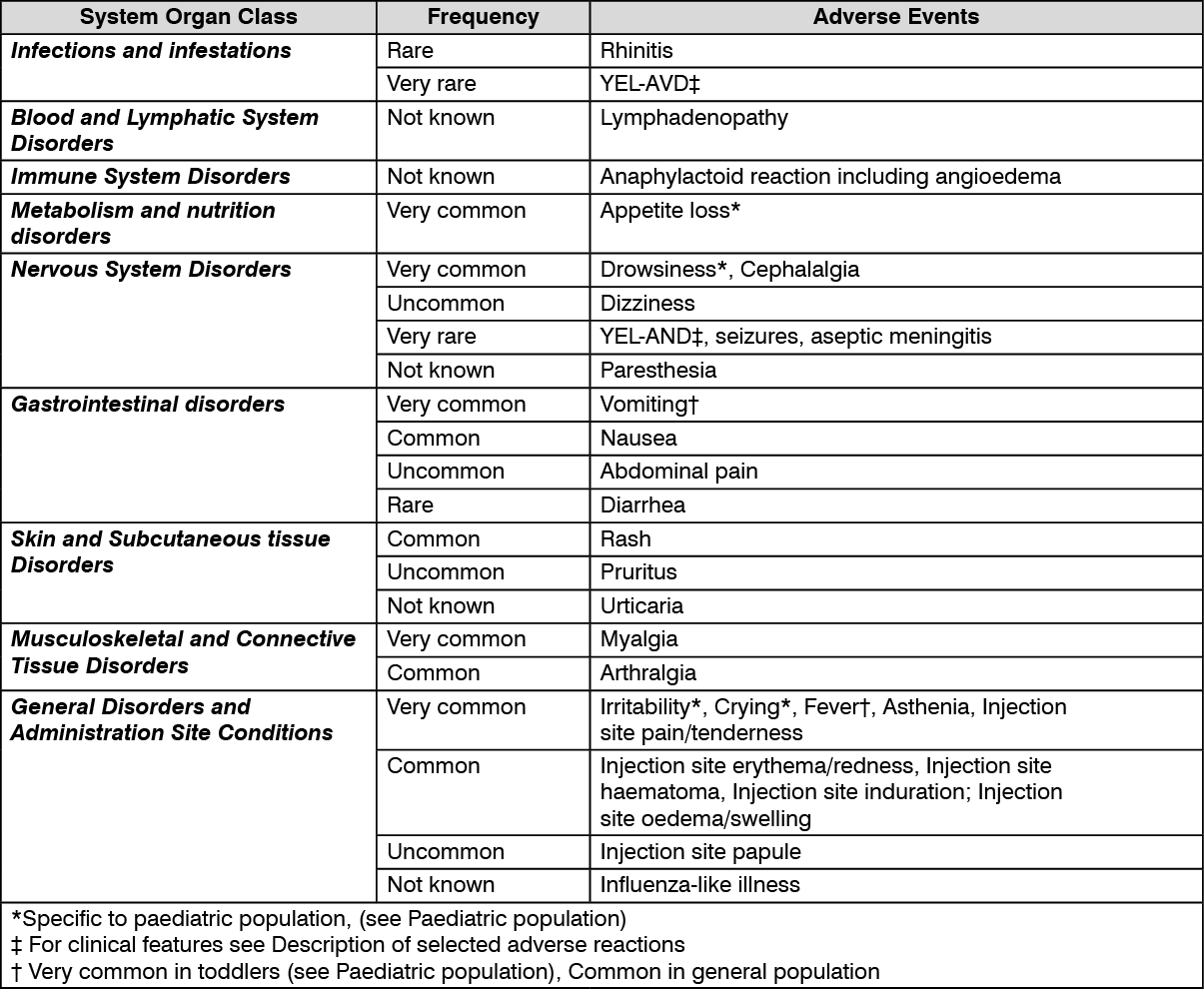
Tabulated List of Adverse Reactions: The table as follows summarises the frequencies of the adverse reactions that were recorded following vaccination with STAMARIL PASTEUR during clinical studies and worldwide post-marketing experience. The adverse reactions are ranked under headings of frequency using the following convention: Very common (>1/10); Common (>1/100 to <1/10); Uncommon (>1/1,000 to <1/100); Rare (>1/10,000 to <1/1,000); Very rare (<1/10,000); Not known (cannot be estimated from available data).
Adverse reactions in each frequency group are presented in the decreasing order of severity. See table.
 Click on icon to see table/diagram/image
Description of Selected Adverse Reactions:
Click on icon to see table/diagram/image
Description of Selected Adverse Reactions: Cases of neurotropic disease (known as YEL-AND), some of which have had a fatal outcome, have been reported to occur within 30 days following vaccination with STAMARIL PASTEUR, and other yellow fever vaccines. YEL-AND may manifest either as an encephalitis (with or without demyelination), or as a neurobiological disease affecting the peripheral nervous system (for example Guillain-Barré syndrome). Encephalitis usually starts with high fever with cephalalgia that may progress to encephalopathy (for example confusion, lethargy, personality change for more than 24h, focal neurological deficits, cerebellar dysfunction or seizures. YEL-AND affecting the peripheral nervous system manifests generally with bilateral weakness of the limbs, or peripheral paresis of the cranial nerves with reduction or disappearance of tendon reflexes (see PRECAUTIONS).
Neurological diseases not fulfilling the YEL-AND criteria have been reported. The manifestations may include cases of aseptic meningitis or seizures not associated with focal neurological signs. These cases are generally of mild or moderate severity and resolve spontaneously.
Cases of viscerotropic disease (known as YEL-AVD and formerly described as "Febrile Multiple Organ-System Failure") have been reported following vaccination with STAMARIL PASTEUR, and other yellow fever vaccines, some of which have been fatal. In the majority of cases reported, the onset of signs and symptoms was within 10 days after the vaccination. Initial signs and symptoms are non-specific and may include fever, myalgia, fatigue, cephalalgia and hypotension, potentially progressing quickly to liver dysfunction with jaundice, muscle cytolysis, thrombocytopenia and acute respiratory and renal failure (see PRECAUTIONS).
Paediatric population: The safety of STAMARIL PASTEUR in paediatric population has been studied through a clinical study performed in 393 toddlers aged 12 to 13 months who received STAMARIL PASTEUR and placebo concomitantly.
The safety profile was assessed during the first 4 weeks following vaccination.
The following most frequently reported adverse reactions specific to the paediatric population were reported as "very common": irritability (34.7%), appetite loss (33.7%), crying (32.1%) and drowsiness (22%).
The other adverse reactions reported in toddlers were also reported from studies in general population: Injection site pain (17.6%), fever (16.5%) and vomiting (17.1%) were reported as "very common" in toddlers. Fever and vomiting were more frequently reported than in general population (see Tabulated summary of adverse reactions as previously mentioned); Injection site erythema (9.8%) and injection site swelling (4.4%) were reported as "common" in toddlers, like in general population, however with significantly higher frequencies compared to general population.
Other Special Population: Congenital or acquired immunodeficiency has been recognised as a potential risk factor for serious adverse events, including YEL-AND (see CONTRAINDICATIONS and PRECAUTIONS).
Age of more than 60 years (see PRECAUTIONS) has been recognized as a potential risk factor for YEL-AVD and YEL-AND.
Age below 9 months (including infants exposed to vaccine through breast-feeding) (see PRECAUTIONS) has been recognised as a potential risk factor for YEL-AND.
A medical history of thymus dysfunction or thymectomy (see CONTRAINDICATIONS and PRECAUTIONS) have been recognised as a predisposing factor for YEL-AVD.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image ≥1000 U_dosef8a2f679-78ac-4726-a13e-a73e0077cdd6.GIF)

 Sign Out
Sign Out
