


 Sign Out
Sign Out



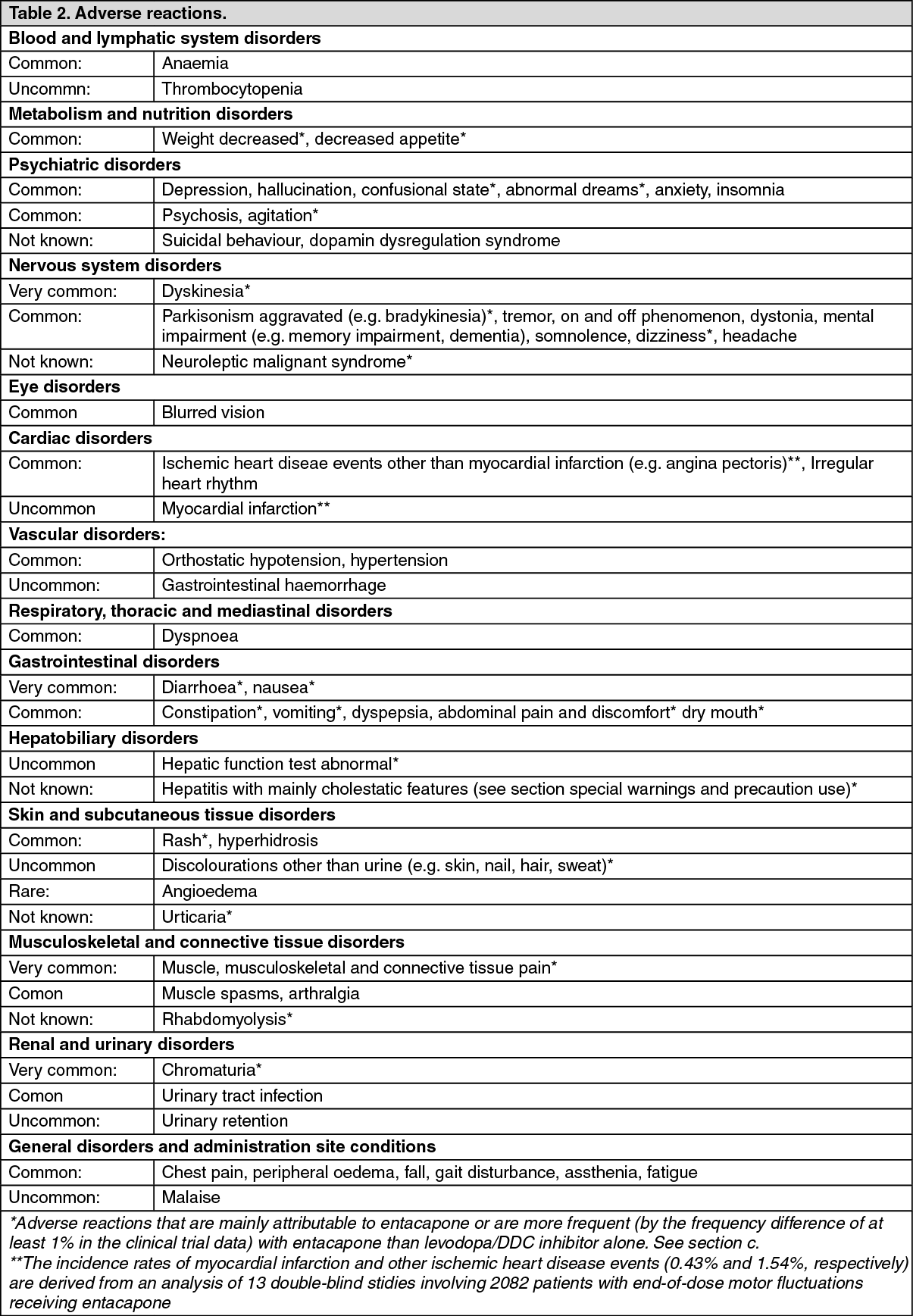
b. Tabulated list of adverse reactions: The following adverse reactions, listed in Table 2, have been accumulated both from a pooled data of eleven double-blind clinical trials consisting of 3230 patients (1810 treated with Stalevo or entacapone combined with levodopa/DDC inhibitor, and 1420 treated with placebo combined with levodopa/DDC inhibitor or cabergoline combined with levodopa/DDC inhibitor), and from the post-marketing data since the introduction of entacapone into the market for the combination use of entacapone with levodopa/DDC inhibitor.
Adverse reactions are ranked under headings of frequency, the most frequent first, using the following convention: Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), not known (cannot be estimated from the available data, since no valid estimate can be derived from clinical trials or epidemiological studies). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagec. Description of selected adverse reactions: Adverse reactions that are mainly attributable to entacapone or are more frequent with entacapone than levodopa/DDC inhibitor alone are indicated with an asterisk in Table 2, under previously mentioned part b. Tabulated list of adverse reactions. Some of these adverse reactions relate to the increased dopaminergic activity (e.g. dyskinesia, nausea and vomiting) and occur most commonly at the beginning of the treatment. Reduction of levodopa dose decreases the severity and frequency of these dopaminergic reactions. Few adverse reactions are known to be directly attributable to the active substance entacapone including diarrhoea and reddish-brown discolouration of urine. Entacapone may in some cases cause also discolouration of e.g. skin, nail, hair and sweat.
Other adverse reactions with an asterisk in Table 2, under previously mentioned part b. Tabulated list of adverse reactions are marked based on either their more frequent occurrence (by the frequency difference of at least 1%) in the clinical trial data with entacapone than levodopa/DDCI alone or the individual case safety reports received after the introduction of entacapone into the market.
Convulsions have occurred rarely with levodopa/carbidopa; however a causal relationship to levodopa/carbidopa therapy has not been established.
Dopamine dysregulation syndrome (DDS) is an addictive disorder seen in some patients treated with levodopa/carbidopa. Affected patients show a compulsive pattern of dopaminergic drug misuse above doses adequate to control motor symptoms, which may in some cases result in severe dyskinesias (see Precautions).
Impulse control disorders: pathological gambling, increased libido, hypersexuality, compulsive spending or buying, binge eating and compulsive eating can occur in patients treated with dopamine agonists and/or other dopaminergic treatments containing levodopa including Stalevo (see Precautions).
Entacapone in association with levodopa has been associated with isolated cases of excessive daytime somnolence and sudden sleep onset episodes.
View ADR Monitoring Form