


 Sign Out
Sign Out


REMIKAF is for IV use only. Continuous infusions of REMIKAF should be administered only by an infusion device. The injection site should be close to the venous cannula and all IV tubing should be cleared at the time of discontinuation of infusion.
REMIKAF should not be administered without dilution.
Consider an alternative to REMIKAF for patients taking mixed agonist/antagonist and partial agonist opioid analgesics due to reduced analgesic effect or potential withdrawal symptoms. If concomitant use is warranted, carefully observe the patient, particularly during treatment initiation and dose adjustment. Discontinue REMIKAF if patient is not responding appropriately to treatment.
General Anesthesia: REMIKAF is not recommended as the sole agent in general anesthesia because loss of consciousness cannot be assured and because of a high incidence of apnea, muscle rigidity, and tachycardia. REMIKAF is synergistic with other anesthetics; therefore, clinicians may need to reduce doses of thiopental, propofol, isoflurane, and midazolam by up to 75% with the coadministration of REMIKAF. The administration of REMIKAF must be individualized based on the patient's response.
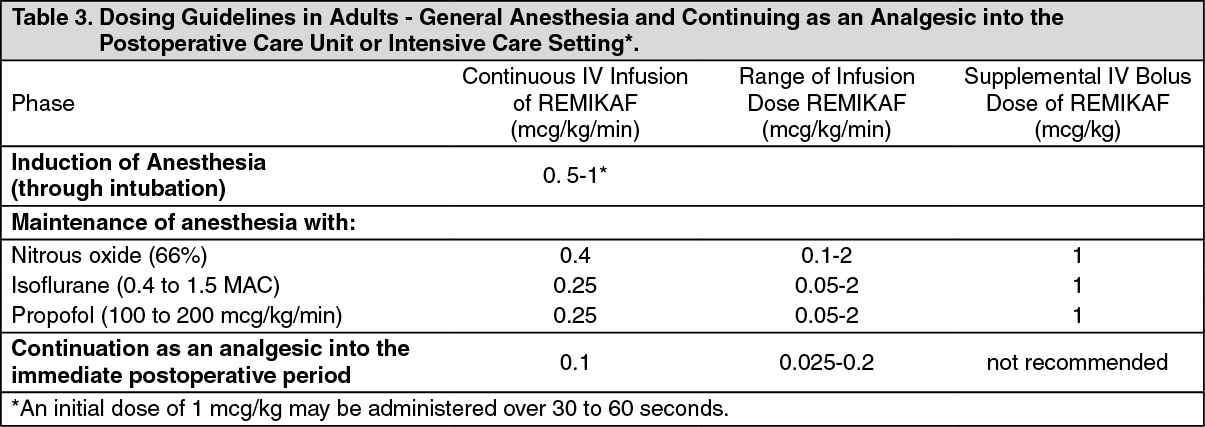
Induction Of Anesthesia: REMIKAF should be administered at an infusion rate of 0.5 to 1 mcg/kg/min with a hypnotic or volatile agent for the induction of anesthesia. If endotracheal intubation is to occur less than 8 minutes after the start of the infusion of REMIKAF, then an initial dose of 1 mcg/kg may be administered over 30 to 60 seconds.
REMIKAF should not be used as a sole agent for induction of anesthesia because loss of consciousness cannot be assured and because of a high incidence of apnea, muscle rigidity, and tachycardia.
Maintenance Of Anesthesia: After endotracheal intubation, the infusion rate of REMIKAF should be decreased in accordance with the dosing guidelines in Table 3 (adults, predominately ASA physical status I, II, or III) and 4 (pediatric patients).
Due to the fast onset and short duration of action of REMIKAF, the rate of administration during anesthesia can be titrated upward in 25% to 100% increments in adult patients or up to 50% increments in pediatric patients, or downward in 25% to 50% decrements every 2 to 5 minutes to attain the desired level of μ-opioid effect.
In response to light anesthesia or transient episodes of intense surgical stress, supplemental bolus doses of 1 mcg/kg may be administered every 2 to 5 minutes.
At infusion rates > 1 mcg/kg/min, increases in the concomitant anesthetic agents should be considered to increase the depth of anesthesia. [See PHARMACOLOGY: Pharmacokinetics: Specific Populations: Pediatric Population under Actions and Table 4 as follows]. (See Table 3.)
 Click on icon to see table/diagram/image
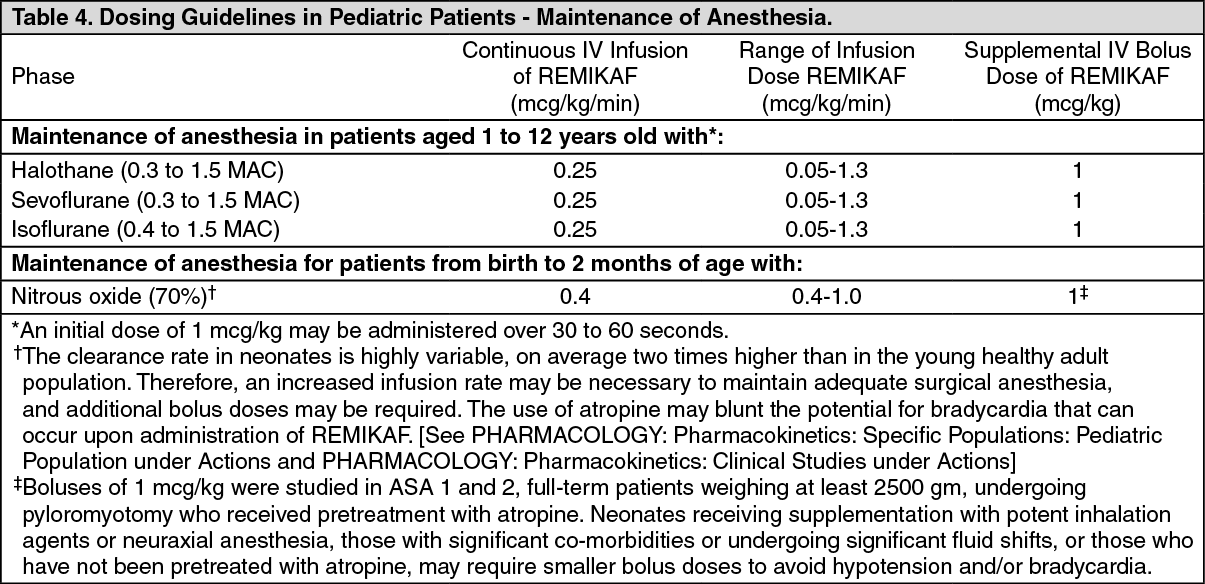
Click on icon to see table/diagram/imageTable 4 summarizes the recommended doses in pediatric patients, predominantly ASA physical status I, II, or III. In pediatric patients, remifentanil was administered with nitrous oxide or nitrous oxide in combination with halothane, sevoflurane, or isoflurane. The use of atropine may blunt the potential for bradycardia that can occur upon administration of REMIKAF. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageContinuation As An Analgesic Into The Immediate Postoperative Period Under The Direct Supervision Of An Anesthesia Practitioner: Infusions of REMIKAF may be continued into the immediate postoperative period for select patients for whom later transition to longer acting analgesics may be desired.
REMIKAF has not been studied in pediatric patients for use in the immediate postoperative period.
The use of bolus injections of REMIKAF to treat pain during the postoperative period is not recommended.
When used as an IV analgesic in the immediate postoperative period, REMIKAF should be initially administered by continuous infusion at a rate of 0.1 mcg/kg/min.
The infusion rate may be adjusted every 5 minutes in 0.025 mcg/kg/min increments to balance the patient's level of analgesia and respiratory rate.
Infusion rates greater than 0.2 mcg/kg/min are associated with respiratory depression (respiratory rate less than 8 breaths/min).
Due to the rapid offset of action of REMIKAF, no residual analgesic activity will be present within 5 to 10 minutes after discontinuation. For patients undergoing surgical procedures where postoperative pain is generally anticipated, alternative analgesics should be administered prior to discontinuation of REMIKAF. The choice of analgesic should be appropriate for the patient's surgical procedure and the level of follow-up care [see Pharmacology: Pharmacokinetics: Clinical Studies under Actions].
Analgesic Component Of Monitored Anesthesia Care: It is strongly recommended that supplemental oxygen be supplied to the patient whenever REMIKAF is administered.
REMIKAF has not been studied for use in children in monitored anesthesia care.
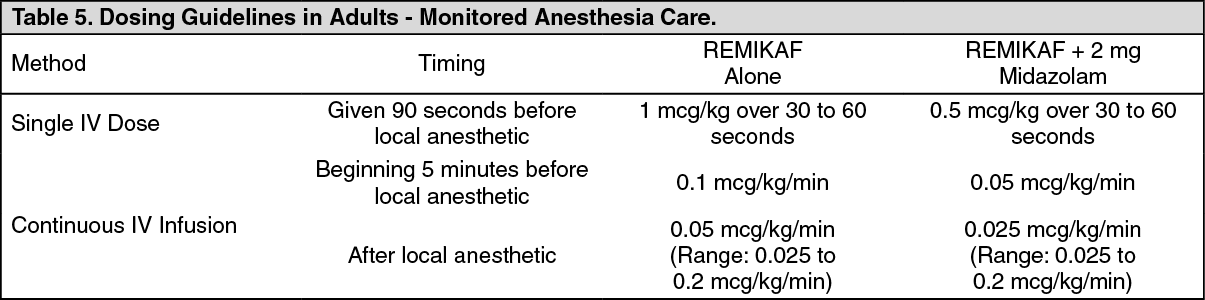
Single Dose: A single IV dose of 0.5 to 1 mcg/kg over 30 to 60 seconds of REMIKAF may be given 90 seconds before the placement of the local or regional anesthetic block [see PRECAUTIONS].
Continuous Infusion: When used alone as an IV analgesic component of monitored anesthesia care, REMIKAF should be initially administered by continuous infusion at a rate of 0.1 mcg/kg/min beginning 5 minutes before placement of the local or regional anesthetic block.
Because of the risk for hypoventilation, the infusion rate of REMIKAF should be decreased to 0.05 mcg/kg/min following placement of the block.
Thereafter, rate adjustments of 0.025 mcg/kg/min at 5 minute intervals may be used to balance the patient's level of analgesia and respiratory rate.
Rates greater than 0.2 mcg/kg/min are generally associated with respiratory depression (respiratory rates less than 8 breaths/min).
Bolus doses of REMIKAF administered simultaneously with a continuous infusion of REMIKAF to spontaneously breathing patients are not recommended.
Table 5 summarizes the recommended doses for monitored anesthesia care in adult patients, predominately ASA physical status I, II, or III. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDiscontinuation: Upon discontinuation of REMIKAF, the IV tubing should be cleared to prevent the inadvertent administration of REMIKAF at a later time. For patients undergoing surgical procedures where postoperative pain is generally anticipated, alternative analgesics should be administered prior to discontinuation of REMIKAF. The choice of analgesic should be appropriate for the patient's surgical procedure and the level of follow-up care [see Pharmacology: Pharmacokinetics: Clinical Studies under Actions].
Dosage Modifications In Geriatric Patients: The starting doses of REMIKAF should be decreased by 50% in elderly patients ( > 65 years). REMIKAF should then be cautiously titrated to effect [see Use in Elderly under Precautions].
Dosage Modifications In Pediatric Patients: See Table 4 for dosing recommendations for use of REMIKAF in pediatric patients from birth to 12 years of age for maintenance of anesthesia. [See PHARMACOLOGY: Pharmacokinetics: Specific Populations: Pediatric Population and Table 4 and Maintenance of Anesthesia as previously mentioned].
REMIKAF has not been studied in pediatric patients for use in the immediate postoperative period or for use as a component of monitored anesthesia care.
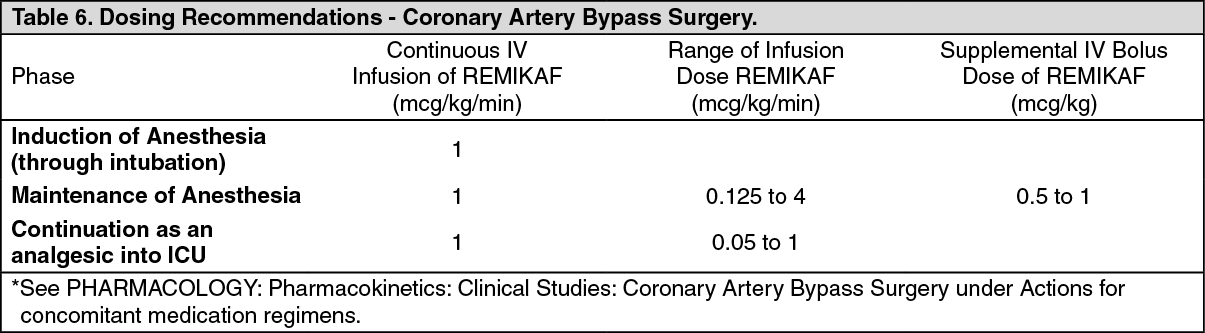
Dosage Modifications In Coronary Artery Bypass Surgery: Table 6 summarizes the recommended doses for induction, maintenance, and continuation as an analgesic into the ICU in adult patients, predominantly ASA physical status III or IV. To avoid hypotension during the induction phase, it is important to consider the concomitant medication regimens. [See Pharmacology: Pharmacokinetics: Clinical Studies: Coronary Artery Bypass Surgery under Actions]. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDosage Modifications In Obese Patients: The starting doses of REMIKAF should be based on ideal body weight (IBW) in obese patients (greater than 30% over their IBW) [see Use in Specific Populations under Precautions].
Dosage Modifications In Preanesthetic Medication: The need for premedication and the choice of anesthetic agents must be individualized. In clinical studies, patients who received REMIKAF frequently received a benzodiazepine premedication.
Preparation For Administration: To reconstitute solution, add 1 mL of diluent per mg of remifentanil. Shake well to dissolve. When reconstituted as directed, the solution contains approximately 1 mg of remifentanil activity per 1 mL.
REMIKAF should be diluted to a recommended final concentration of 20, 25, 50, or 250 mcg/mL prior to administration (see Table 7). REMIKAF should not be administered without dilution. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageContinuous IV infusions of REMIKAF should be administered only by an infusion device. Infusion rates of REMIKAF can be individualized for each patient using Table 8: See Table 8.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageWhen REMIKAF is used as an analgesic component of monitored analgesia care, a final concentration of 25 mcg/mL is recommended. When REMIKAF is used for pediatric patients 1 year of age and older, a final concentration of 20 or 25 mcg/mL is recommended. Table 9 is a guideline for milliliter-per-hour delivery for a solution of 20 mcg/mL with an infusion device. (See Table 9.)
 Click on icon to see table/diagram/image
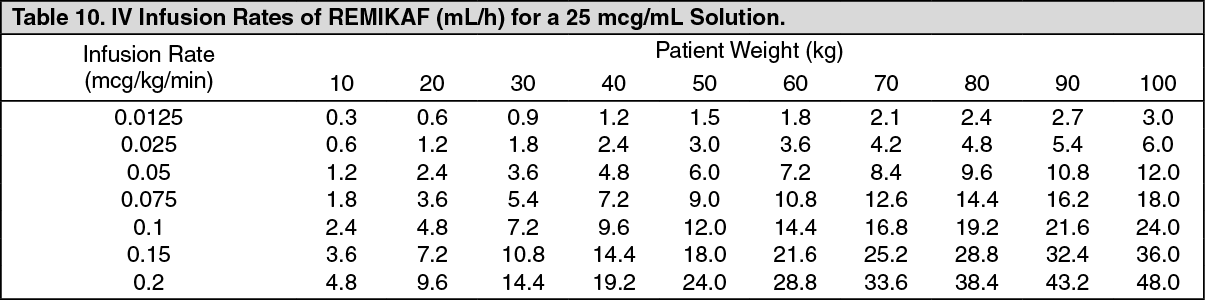
Click on icon to see table/diagram/imageTable 10 is a guideline for milliliter-per-hour delivery for a solution of 25 mcg/mL with an infusion device. (See Table 10.)
 Click on icon to see table/diagram/image
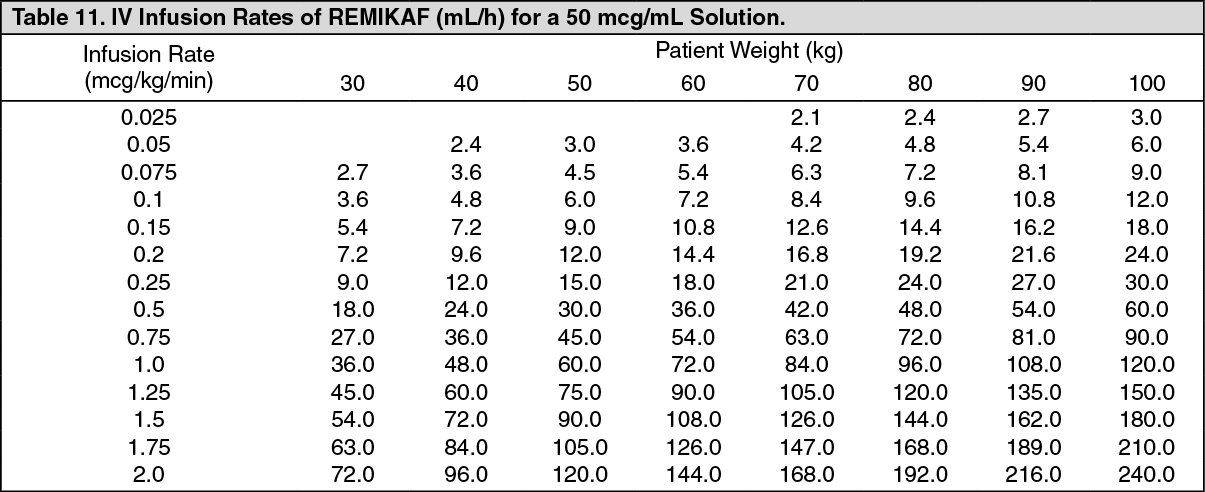
Click on icon to see table/diagram/imageTable 11 is a guideline for milliliter-per-hour delivery for a solution of 50 mcg/mL with an infusion device.(See Table 11.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTable 12 is a guideline for milliliter-per-hour delivery for a solution of 250 mcg/mL with an infusion device.(See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCompatibility And Stability: Reconstitution And Dilution Prior To Administration: REMIKAF is stable for 24 hours at room temperature after reconstitution and further dilution to concentrations of 20 to 250 mcg/mL with the IV fluids listed as follows: Sterile Water for Injection, 5% Dextrose Injection, 5% Dextrose and 0.9% Sodium Chloride Injection, 0.9% Sodium Chloride Injection, 0.45% Sodium Chloride Injection, Lactated Ringer's and 5% Dextrose Injection.
REMIKAF is stable for 4 hours at room temperature after reconstitution and further dilution to concentrations of 20 to 250 mcg/mL with Lactated Ringer's Injection.
REMIKAF has been shown to be compatible with these IV fluids when coadministered into a running IV administration set.
Compatibility With Other Therapeutic Agents: REMIKAF has been shown to be compatible with Diprivan (propofol) Injection when coadministered into a running IV administration set. The compatibility of REMIKAF with other therapeutic agents has not been evaluated.
Incompatibilities: Nonspecific esterases in blood products may lead to the hydrolysis of remifentanil to its carboxylic acid metabolite. Therefore, administration of REMIKAF into the same IV tubing with blood is not recommended.
Note: Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration whenever solution and container permit. Product should be a clear, colorless liquid after reconstitution and free of visible particulate matter.
REMIKAF does not contain any antimicrobial preservative and thus care must be taken to assure the sterility of prepared solutions.