


 Sign Out
Sign Out



Primary prevention of venous thromboembolic events in adult patients who have undergone elective total hip replacement surgery or total knee replacement surgery: Adults: VTE prevention following knee replacement surgery: Treatment with PRADAXA should be initiated orally within 1 - 4 hours of completed surgery with a single capsule (110 mg) and continuing with 2 capsules once daily thereafter for a total of 10 days. If haemostasis is not secured, initiation of treatment should be delayed. If treatment is not started on the day of surgery then treatment should be initiated with 2 capsules once daily.
VTE prevention following hip replacement surgery: Treatment with PRADAXA should be initiated orally within 1 - 4 hours of completed surgery with a single capsule (110 mg) and continuing with 2 capsules once daily thereafter for a total of 28 - 35 days. If haemostasis is not secured, initiation of treatment should be delayed. If treatment is not started on the day of surgery then treatment should be initiated with 2 capsules once daily.
Children: PRADAXA has not been investigated in patients <18 years of age. Treatment of children with PRADAXA is not recommended.
Hepatic impairment: Patients with moderate and severe hepatic impairment (Child-Pugh classification B and C) or liver disease expected to have any impact on survival or with elevated liver enzymes > 2 Upper Limit Normal (ULN) were excluded in clinical trials. Therefore the use of dabigatran etexilate is not recommended in this population.
Renal impairment: Renal function should be assessed by calculating the creatinine clearance (CrCl) prior to initiation of treatment with PRADAXA to exclude patients for treatment with severe renal impairment (i.e. CrCl < 30ml/min). There are no data to support use in patients with severe renal impairment (< 30 mL/min creatinine clearance); treatment in this population with PRADAXA is not recommended (See Contraindications).
While on treatment renal function should be assessed in certain clinical situations when it is suspected that the renal function could decline or deteriorate (such as hypovolemia, dehydration, and with certain comedications, etc).
After i.v. application 85 % of dabigatran in plasma is cleared through the kidneys. Patients with moderate renal impairment (30-50 ml/min creatinine clearance) appear to be at higher risk of bleeding. Dosing should be reduced to 150 mg PRADAXA taken once daily as 2 capsules of 75 mg in patients with moderate renal impairment.
Regular assessment of renal status is required in these patients (see Contraindications and Renal under Precautions). A coagulation test, such as aPTT (see Monitoring and Laboratory Tests under Precautions), may help to identify patients with an increased bleeding risk caused by excessive dabigatran exposure.
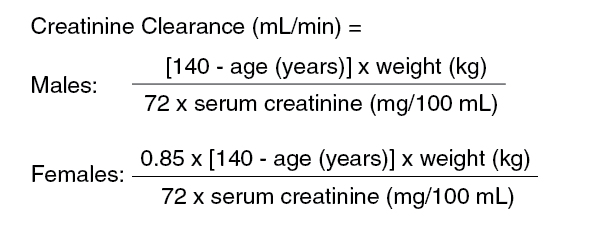
Creatinine clearance can be estimated using the Cockroft-Gault formula as follows:
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageElderly: Pharmacokinetic studies in older subjects demonstrate an increase in drug exposure in those patients with age-related decline of renal function. See also dose and administration in renal impairment.
As renal impairment may be frequent in the elderly (>75 years), renal function should be assessed by calculating the creatinine clearance (CrCl) prior to initiation of treatment with PRADAXA to exclude patients for treatment with severe renal impairment (i.e. CrCl < 30ml/min ). The renal function should also be assessed in certain clinical situations when it is suspected that the renal function could decline or deteriorate (such as hypovolemia, dehydration, and with certain comedications, etc).
The clinical studies have been conducted in patient population with a mean age > 65 years. In general patients should be treated with 220 mg dabigatran etexilate daily.
Weight: Population PK modelling shows that patients with a body weight of 120 kg have about 20% lower drug exposure and patients with a body weight of 48 kg have about 25% higher drug exposure compared to patients with an average weight (BISTRO II). Since there was no difference in efficacy and bleeding rates, no dose adjustment is necessary.
Concomitant use of PRADAXA with strong P-glycoprotein inhibitors, i.e. amiodarone, quinidine or verapamil: Dosing should be reduced to PRADAXA 150 mg taken once daily as 2 capsules of 75 mg in patients who concomitantly receive PRADAXA and amiodarone, quinidine or verapamil (see Interactions).
Treatment initiation with verapamil should be avoided in patients who have undergone elective total hip replacement surgery or total knee replacement surgery who are already treated with PRADAXA. Simultaneous initiation of treatment with PRADAXA and verapamil should also be avoided.
Switching from PRADAXA treatment to parenteral anticoagulant: Wait 24 hours after the last dose before switching from PRADAXA to a parenteral anticoagulant.
Switching from parenteral anticoagulants treatment to PRADAXA: No data are available, therefore it is not recommended to start the administration of dabigatran etexilate before the next scheduled dose of the parenteral anticoagulant would have been due.
Missed dose: Continue with your remaining daily doses of PRADAXA at the same time of the next day.
Do not take a double dose to make up for missed individual doses.
Prevention of stroke and systemic embolism in patients with atrial fibrillation with at least one additional risk factor for stroke (i.e., previous ischemic stroke, transient ischemic attack [TIA], or systemic embolism; left ventricular dysfunction): Adults : The recommended daily dose of PRADAXA is 300 mg taken orally as 150 mg hard capsules twice daily. Therapy should be continued life-long. In case of intolerability, patients should be instructed to contact their doctor.
Children: PRADAXA has not been investigated in patients <18 years of age. Treatment of children with PRADAXA is not recommended.
Hepatic impairment: Patients with moderate and severe hepatic impairment (Child-Pugh classification B and C) or liver disease expected to have any impact on survival or with elevated liver enzymes > 2 Upper Limit Normal (ULN) were excluded in clinical trials. Therefore the use of dabigatran etexilate is not recommended in this population.
Renal impairment: Renal function should be assessed by calculating the creatinine clearance (CrCl) prior to initiation of treatment with PRADAXA to exclude patients for treatment with severe renal impairment (i.e. CrCl < 30ml/min). There are no data to support use in patients with severe renal impairment (< 30 mL/min creatinine clearance); treatment in this population with PRADAXA is not recommended (See Contraindications).
While on treatment renal function should be assessed in certain clinical situations when it is suspected that the renal function could decline or deteriorate (such as hypovolemia, dehydration, and with certain comedications, etc).
In patients with moderate renal impairment (CrCl 30-50 ml/min) the renal function should be assessed at least once a year.
No dose adjustment necessary, patients with moderate renal impairment (CrCl 30-50 ml/min) should be treated with a daily dose of 300 mg taken orally as 150 mg hard capsules twice daily, with caution.
Regular assessment of renal status is required in these patients (see Contraindications and Renal under Precautions). A coagulation test, such as aPTT (see Monitoring and Laboratory Tests under Precautions), may help to identify patients with an increased bleeding risk caused by excessive dabigatran exposure. Creatinine clearance can be estimated using the Cockroft-Gault formula as follows:
Click on icon to see table/diagram/imageElderly: Pharmacokinetic studies in older subjects demonstrate an increase in drug exposure in those patients with age-related decline of renal function. See also dose and administration in renal impairment.
As renal impairment may be frequent in the elderly (>75 years), renal function should be assessed by calculating the creatinine clearance (CrCl) prior to initiation of treatment with PRADAXA to exclude patients for treatment with severe renal impairment (i.e. CrCl < 30ml/min ). The renal function should also be assessed at least once a year in patients treated with PRADAXA or more frequently as needed in certain clinical situations when it is suspected that the renal function could decline or deteriorate (such as hypovolemia, dehydration, and with certain comedications, etc).
Patients aged 80 years or above should be treated with a daily dose of 220 mg, taken orally as 110 mg hard capsules twice daily.
Weight: Population PK modelling shows that patients with a body weight of 120 kg have about 20% lower drug exposure and patients with a body weight of 48 kg have about 25% higher drug exposure compared to patients with an average weight (BISTRO II). Since there was no difference in efficacy and bleeding rates, no dose adjustment is necessary.
Concomitant use of PRADAXA with strong P-glycoprotein inhibitors, i.e. amiodarone, quinidine or verapamil: No dose adjustment necessary, patients should be treated with a daily dose of 300 mg taken orally as 150 mg hard capsules twice daily.
Patients at risk of bleeding: The presence of the following factors may increase the risk of bleeding, e.g. age ≥ 75 years, moderate renal impairment (30-50 ml CrCL/min), concomitant treatment with strong P-gp inhibitors (see Pharmacology: Pharmacokinetics: Special Population under Actions), antiplatelets or previous gastro-intestinal bleed (see Precautions). For patients with one or more than one of these risk factors, a reduced daily dose of 220 mg given as 110 mg twice daily may be considered at the discretion of physician.
Switching from PRADAXA treatment to parenteral anticoagulant: Wait 12 hours after the last dose before switching from PRADAXA to a parenteral anticoagulant.
Switching from parenteral anticoagulants treatment to PRADAXA: No data are available, therefore it is not recommended to start the administration of dabigatran etexilate before the next scheduled dose of the parenteral anticoagulant would have been due.
Switching from Vit. K antagonists to PRADAXA: The Vit. K antagonist should be stopped. PRADAXA can be given as soon as the INR is < 2.0.
Switching from PRADAXA to Vit. K antagonists: The starting time of the Warfarin should be adjusted according to the patient's Creatinine Clearance as follows: CrCL ≥ 50 ml/min, start Warfarin 3 days before discontinuing dabigatran etexilate;
CrCL ≥ 30-< 50 ml/min, start Warfarin 2 days before discontinuing dabigatran etexilate.
Cardioversion: Patients can stay on PRADAXA while being cardioverted.
Missed dose: A forgotten PRADAXA dose may still be taken up to 6 hours prior to the next scheduled dose. From 6 hours prior to the next scheduled dose on, the missed dose should be omitted.
Do not take a double dose to make up for missed individual doses.
Treatment of acute deep vein thrombosis (DVT) and/or pulmonary embolism (PE): The recommended daily dose of PRADAXA is 300 mg taken orally as 150 mg hard capsules twice daily following treatment with a parenteral anticoagulant for at least 5 days. Therapy should be continued for up to 6 months.
Children: The safety and efficacy in children has not yet been established. Treatment of children with PRADAXA is therefore not recommended.
Renal impairment: Renal function should be assessed by calculating the creatinine clearance (CrCl) prior to initiation of treatment with PRADAXA to exclude patients for treatment with severe renal impairment (i.e. CrCl < 30 mL/min).There are no data to support use in patients with severe renal impairment (< 30 mL/min CrCl); treatment in this population with PRADAXA is not recommended (see Contraindications).
While on treatment renal function should be assessed in certain clinical situations when it is suspected that the renal function could decline or deteriorate (such as hypovolemia, dehydration, and with certain comedications, etc).
Dabigatran can be dialysed; there is limited clinical experience to demonstrate the utility of this approach in clinical studies.
No dose adjustment necessary in patients with renal function over CrCl 30 mL/min. Patients should be treated with a daily dose of 300 mg taken orally as 150 mg hard capsules twice daily.
Elderly: As renal impairment may be frequent in the elderly (>75 years), renal function should be assessed by calculating the creatinine clearance (CrCl) prior to initiation of treatment with PRADAXA to exclude patients for treatment with severe renal impairment (i.e. CrCl < 30 mL/min ). The renal function should also be assessed in patients treated with PRADAXA as needed in certain clinical situations when it is suspected that the renal function could decline or deteriorate (such as hypovolemia, dehydration, and with certain comedications, etc).
No dose adjustment necessary, patients should be treated with a daily dose of 300 mg taken orally as 150 mg hard capsules twice daily.
Pharmacokinetic studies in older subjects demonstrate an increase in drug exposure in those patients with age-related decline of renal function.
See also dose and administration in renal impairment.
Weight: No dose adjustment is necessary.
Concomitant use of PRADAXA with strong P-glycoprotein inhibitors, i.e. amiodarone, quinidine or verapamil: No dose adjustment necessary, patients should be treated with a daily dose of 300 mg taken orally as 150 mg hard capsules twice daily.
Patients at risk of bleeding: The presence of the following factors may increase the risk of bleeding: e.g. age ≥ 75 years, moderate renal impairment (30-50 mL/min CrCl) or previous gastro-intestinal bleed (see Precautions).
No dose adjustment is necessary for patients with single risk factors.
Limited clinical data are available for patients with multiple risk factors.
In these patients, PRADAXA should only be given if the expected benefit outweighs bleeding risks.
Switching from PRADAXA treatment to parenteral anticoagulant: Wait 12 hours after the last dose before switching from PRADAXA to a parenteral anticoagulant.
Switching from parenteral anticoagulants treatment to PRADAXA: PRADAXA should be given 0-2 hours prior to the time that the next dose of the alternate therapy would be due, or at the time of discontinuation in case of continuous treatment (e.g. intravenous UFH).
Switching from Vit. K antagonists to PRADAXA: The Vit. K antagonist should be stopped. PRADAXA can be given as soon as the INR is < 2.0.
Switching from PRADAXA to Vit. K antagonists: The starting time of the Warfarin should be adjusted according to the patient's Creatinine Clearance as follows: CrCL ≥ 50 ml/min, start Warfarin 3 days before discontinuing dabigatran etexilate;
CrCL ≥ 30-< 50 ml/min, start Warfarin 2 days before discontinuing dabigatran etexilate.
Missed dose: A forgotten PRADAXA dose may still be taken up to 6 hours prior to the next scheduled dose. From 6 hours prior to the next scheduled dose on, the missed dose should be omitted.
Do not take a double dose to make up for missed individual doses.