Pharmacotherapeutic group: Drugs used in diabetes, Glucagon-like peptide-1 (GLP-1) analogues.
ATC code: A10BJ06.
Pharmacology: Pharmacodynamics: Mechanism of action: Semaglutide is a GLP-1 analogue with 94% sequence homology to human GLP-1. Semaglutide acts as a GLP-1 receptor agonist that selectively binds to and activates the GLP-1 receptor, the target for native GLP-1.
GLP-1 is a physiological hormone that has multiple actions in glucose and appetite regulation, and in the cardiovascular system. The glucose and appetite effects are specifically mediated via GLP-1 receptors in the pancreas and the brain.
Semaglutide reduces blood glucose in a glucose dependent manner by stimulating insulin secretion and lowering glucagon secretion when blood glucose is high. The mechanism of blood glucose lowering also involves a minor delay in gastric emptying in the early postprandial phase. During hypoglycaemia, semaglutide diminishes insulin secretion and does not impair glucagon secretion.
Semaglutide reduces body weight and body fat mass through lowered energy intake, involving an overall reduced appetite. In addition, semaglutide reduces the preference for high fat foods.
GLP-1 receptors are also expressed in the heart, vasculature, immune system and kidneys. Semaglutide had a beneficial effect on plasma lipids, lowered systolic blood pressure and reduced inflammation in clinical studies. In animal studies, semaglutide attenuates the development of atherosclerosis by preventing aortic plaque progression and reducing inflammation in the plaque.
Pharmacodynamic effects: All pharmacodynamic evaluations were performed after 12 weeks of treatment (including dose escalation) at steady state with semaglutide 1 mg once weekly.
Fasting and postprandial glucose: Semaglutide reduces fasting and postprandial glucose concentrations. In patients with type 2 diabetes, treatment with semaglutide 1 mg resulted in reductions in glucose in terms of absolute change from baseline (mmol/l) and relative reduction compared to placebo (%) for fasting glucose (1.6 mmol/l; 22% reduction), 2 hour postprandial glucose (4.1 mmol/l; 37% reduction), mean 24 hour glucose concentration (1.7 mmol/l; 22% reduction) and postprandial glucose excursions over 3 meals (0.6-1.1 mmol/l) compared with placebo. Semaglutide lowered fasting glucose after the first dose.
Beta-cell function and insulin secretion: Semaglutide improves beta-cell function. Compared to placebo, semaglutide improved first- and second-phase insulin response with a 3- and 2-fold increase, respectively, and increased maximal beta-cell secretory capacity in patients with type 2 diabetes. In addition, semaglutide treatment increased fasting insulin concentrations compared to placebo.
Glucagon secretion: Semaglutide lowers the fasting and postprandial glucagon concentrations. In patients with type 2 diabetes, semaglutide resulted in the following relative reductions in glucagon compared to placebo: fasting glucagon (8-21%), postprandial glucagon response (14-15%) and mean 24 hour glucagon concentration (12%).
Glucose dependent insulin and glucagon secretion: Semaglutide lowered high blood glucose concentrations by stimulating insulin secretion and lowering glucagon secretion in a glucose dependent manner. With semaglutide, the insulin secretion rate in patients with type 2 diabetes was comparable to that of healthy subjects.
During induced hypoglycaemia, semaglutide compared to placebo did not alter the counter regulatory responses of increased glucagon and did not impair the decrease of C-peptide in patients with type 2 diabetes.
Gastric emptying: Semaglutide caused a minor delay of early postprandial gastric emptying, thereby reducing the rate at which glucose appears in the circulation postprandially.
Appetite, energy intake and food choice: Semaglutide compared to placebo lowered the energy intake of 3 consecutive
ad libitum meals by 18-35%. This was supported by a semaglutide-induced suppression of appetite in the fasting state as well as postprandially, improved control of eating, less food cravings and a relative lower preference for high fat food.
Fasting and postprandial lipids: Semaglutide compared to placebo lowered fasting triglyceride and very low density lipoproteins (VLDL) cholesterol concentrations by 12% and 21%, respectively. The postprandial triglyceride and VLDL cholesterol response to a high fat meal was reduced by >40%.
Cardiac electrophysiology (QTc): The effect of semaglutide on cardiac repolarization was tested in a thorough QTc trial. Semaglutide did not prolong QTc intervals at supra-therapeutic dose levels (up to 1.5 mg at steady state).
Clinical efficacy and safety: Both improvement of glycaemic control and reduction of cardiovascular morbidity and mortality are an integral part of the treatment of type 2 diabetes.
The efficacy and safety of Ozempic 0.5 mg and 1 mg once weekly were evaluated in six randomised controlled phase 3a trials that included 7,215 patients with type 2 diabetes mellitus (4,107 treated with semaglutide). Five trials (SUSTAIN 1-5) had the glycaemic efficacy assessment as the primary objective, while one trial (SUSTAIN 6) had cardiovascular outcome as the primary objective.
An additional trial including 1,201 patients was conducted to compare the efficacy and safety of Ozempic 0.5 mg and 1 mg once weekly to dulaglutide 0.75 mg and 1.5 mg once weekly, respectively.
Treatment with semaglutide demonstrated sustained, statistically superior and clinically meaningful reductions in HbA
1c and body weight for up to 2 years compared to placebo and active control treatment (sitagliptin, insulin glargine, exenatide ER and dulaglutide).
The efficacy of semaglutide was not impacted by age, gender, race, ethnicity, BMI at baseline, body weight (kg) at baseline, diabetes duration and level of renal function impairment.
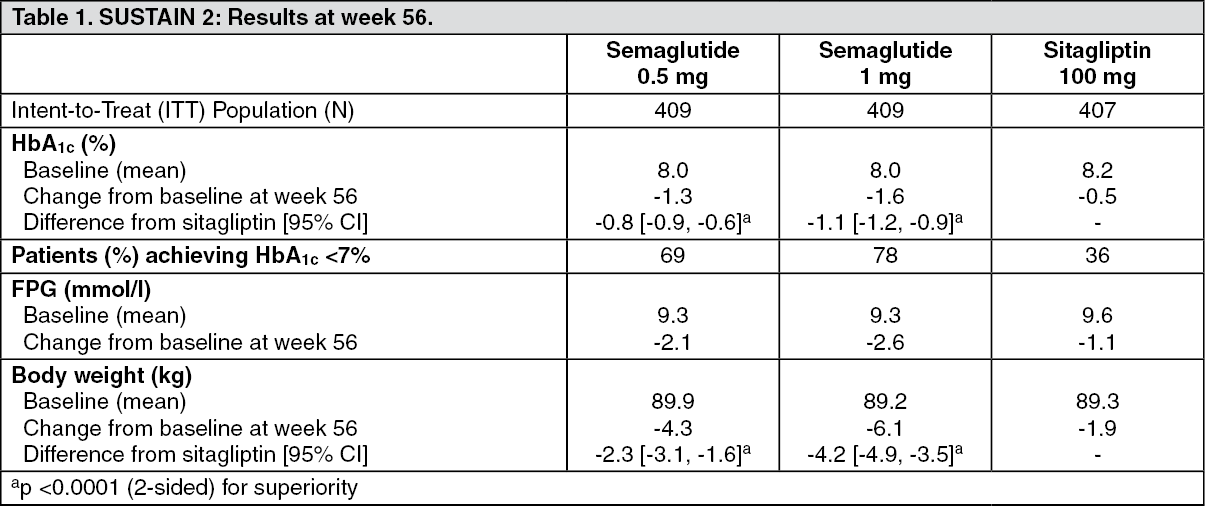
SUSTAIN 2 - Ozempic vs. sitagliptin both in combination with 1-2 oral antidiabetic drugs (metformin and/or thiazolidinediones): In a 56-week active-controlled double-blind trial, 1,231 patients were randomised to Ozempic 0.5 mg once weekly, Ozempic 1 mg once weekly or sitagliptin 100 mg once daily, all in combination with metformin (94%) and/or thiazolidinediones (6%). (See Table 1 and Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
SUSTAIN 7 - Ozempic vs. dulaglutide both in combination with metformin: In a 40-week, open-label trial, 1,201 patients on metformin were randomised 1:1:1:1 to once weekly Ozempic 0.5 mg, dulaglutide 0.75 mg, Ozempic 1 mg or dulaglutide 1.5 mg, respectively.
The trial compared 0.5 mg of Ozempic to 0.75 mg of dulaglutide and 1 mg of Ozempic to 1.5 mg of dulaglutide.
Gastrointestinal disorders were the most frequent adverse events, and occurred in similar proportion of patients receiving Ozempic 0.5 mg (129 patients [43%]), Ozempic 1 mg (133 [44%]), and dulaglutide 1.5 mg (143 [48%]); fewer patients had gastrointestinal disorders with dulaglutide 0.75 mg (100 [33%]).
At week 40, the increase in pulse rate for Ozempic (0.5 mg and 1 mg) and dulaglutide (0.75 mg and 1.5 mg) was 2.4, 4.0, and 1.6, 2.1, beats/min, respectively. (See Table 2 and Figure 2.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
SUSTAIN 3 - Ozempic vs. exenatide ER both in combination with metformin or metformin with sulfonylurea: In a 56-week open-label trial, 813 patients on metformin alone (49%), metformin with sulfonylurea (45%) or other (6%) were randomised to Ozempic 1 mg or exenatide ER 2 mg once weekly. (See Table 3.)
Click on icon to see table/diagram/image
SUSTAIN 4 - Ozempic vs. insulin glargine both in combination with 1-2 oral antidiabetic drugs (metformin or metformin and sulfonylurea): In a 30-week open-label comparator trial 1,089 patients were randomised to Ozempic 0.5 mg once weekly, Ozempic 1 mg once weekly, or insulin glargine once-daily on a background of metformin (48%) or metformin and sulfonylurea (51%). (See Table 4.)
Click on icon to see table/diagram/image
SUSTAIN 5 - Ozempic vs. placebo both in combination with basal insulin: In a 30-week double-blind placebo-controlled trial, 397 patients inadequately controlled with basal insulin with or without metformin were randomised to Ozempic 0.5 mg once weekly, Ozempic 1 mg once weekly or placebo. (See Table 5.)
Click on icon to see table/diagram/image
Combination with sulfonylurea monotherapy: In SUSTAIN 6 (see Cardiovascular disease as follows) 123 patients were on sulfonylurea monotherapy at baseline. HbA
1c at baseline was 8.2%, 8.4% and 8.4% for Ozempic 0.5 mg, Ozempic 1 mg, and placebo, respectively. At week 30, the change in HbA
1c was -1.6%, -1.5% and 0.1% for Ozempic 0.5 mg, Ozempic 1 mg, and placebo, respectively.
Combination with premix insulin ± 1-2 OADs: In SUSTAIN 6 (see Cardiovascular disease as follows) 867 patients were on premix insulin (with or without OAD(s)) at baseline. HbA
1c at baseline was 8.8%, 8.9% and 8.9% for Ozempic 0.5 mg, Ozempic 1 mg, and placebo, respectively. At week 30, the change in HbA
1c was -1.3%, -1.8% and -0.4% for Ozempic 0.5 mg, Ozempic 1 mg, and placebo, respectively.
Cardiovascular disease: In a 104-week double-blind trial (SUSTAIN 6), 3,297 patients with type 2 diabetes mellitus at high cardiovascular risk were randomised to either Ozempic 0.5 mg once weekly, Ozempic 1 mg once weekly or corresponding placebo in addition to standard-of-care hereafter followed for 2 years. In total 98% of the patients completed the trial and the vital status was known at the end of the trial for 99.6% of the patients.
The trial population was distributed by age as: 1,598 patients (48.5%) ≥65 years, 321 (9.7%) ≥75 years, and 20 (0.6%) ≥85 years. There were 2,358 patients with normal or mild renal impairment, 832 with moderate and 107 with severe or end stage renal impairment. There were 61% males, the mean age was 65 years and mean BMI was 33 kg/m
2. The mean duration of diabetes was 13.9 years.
The primary endpoint was time from randomisation to first occurrence of a major adverse cardiovascular event (MACE): cardiovascular death, non-fatal myocardial infarction or non-fatal stroke.
The total number of primary component MACE endpoints was 254, including 108 (6.6%) with semaglutide and 146 (8.9%) with placebo. See Figure 4 for results on primary and secondary cardiovascular endpoints. Treatment with semaglutide resulted in a 26% risk reduction in the primary composite outcome of death from cardiovascular causes, non-fatal myocardial infarction or non-fatal stroke. The total numbers of cardiovascular deaths, non-fatal myocardial infarctions and non-fatal strokes were 90, 111, and 71, respectively, including 44 (2.7%), 47 (2.9%), and 27 (1.6%), respectively, with semaglutide (Figure 4). The risk reduction in the primary composite outcome was mainly driven by decreases in the rate of non-fatal stroke (39%) and non-fatal myocardial infarction (26%) (Figure 3). (See Figure 3 and Figure 4.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
There were 158 events of new or worsening nephropathy. The hazard ratio [95% CI] for time to nephropathy (new onset of persistent macroalbuminuria, persistent doubling of serum creatinine, need for continuous renal replacement therapy and death due to renal disease) was 0.64 [0.46; 0.88] driven by new onset of persistent macroalbuminuria.
Body weight: After one year of treatment, a weight loss of ≥5% and ≥10% was achieved for more subjects with Ozempic 0.5 mg (46% and 13%) and 1 mg (52-62% and 21-24%) compared with the active comparators sitagliptin (18% and 3%) and exenatide ER (17% and 4%).
In the 40-week trial vs. dulaglutide a weight loss of ≥5% and ≥10% was achieved for more subjects with Ozempic 0.5 mg (44% and 14%) compared with dulaglutide 0.75 mg (23% and 3%) and Ozempic 1 mg (up to 63% and 27%) compared with dulaglutide 1.5 mg (30% and 8%).
A significant and sustained reduction in body weight from baseline to week 104 was observed with Ozempic 0.5 mg and 1 mg vs. placebo 0.5 mg and 1 mg, in addition to standard-of-care (-3.6 kg and -4.9 kg vs. -0.7 kg and -0.5 kg , respectively) in SUSTAIN 6.
Blood pressure: Significant reductions in mean systolic blood pressure were observed when Ozempic 0.5 mg (3.5-5.1 mmHg) and 1 mg (5.4-7.3 mmHg) were used in combination with oral antidiabetic medicinal products or basal insulin. For diastolic blood pressure, there were no significant differences between semaglutide and comparators.
Pharmacokinetics: Compared to native GLP-1, semaglutide has a prolonged half-life of around 1 week making it suitable for once weekly subcutaneous administration. The principal mechanism of protraction is albumin binding, which results in decreased renal clearance and protection from metabolic degradation. Furthermore, semaglutide is stabilised against degradation by the DPP-4 enzyme.
Absorption: Maximum concentration was reached 1 to 3 days post dose. Steady state exposure was achieved following 4-5 weeks of once weekly administration. In patients with type 2 diabetes, the mean steady state concentrations following subcutaneous administration of 0.5 mg and 1 mg semaglutide were approximately 16 nmol/l and 30 nmol/l, respectively.
Semaglutide exposure increased in a dose proportional manner for doses of 0.5 mg and 1 mg. Similar exposure was achieved with subcutaneous administration of semaglutide in the abdomen, thigh, or upper arm. Absolute bioavailability of subcutaneous semaglutide was 89%.
Distribution: The mean volume of distribution of semaglutide following subcutaneous administration in patients with type 2 diabetes was approximately 12.5 l. Semaglutide was extensively bound to plasma albumin (>99%).
Metabolism/Biotransformation: Prior to excretion, semaglutide is extensively metabolised through proteolytic cleavage of the peptide backbone and sequential beta-oxidation of the fatty acid sidechain. The enzyme neutral endopeptidase (NEP) is expected to be involved in the metabolism of semaglutide.
Elimination: In a study with a single subcutaneous dose of radiolabelled semaglutide, it was found that the primary excretion routes of semaglutide-related material were via urine and faeces; approximately 2/3 of semaglutide-related material were excreted in urine and approximately 1/3 in faeces. Approximately 3% of the dose was excreted as intact semaglutide via urine. In patients with type 2 diabetes clearance of semaglutide was approximately 0.05 l/h. With an elimination half-life of approximately 1 week, semaglutide will be present in the circulation for about 5 weeks after the last dose.
Special population: Elderly: Age had no effect on the pharmacokinetics of semaglutide based on data from phase 3a studies including patients of 20-86 years of age.
Gender, race and ethnicity: Gender, race (White, Black or African-American, Asian) and ethnicity (Hispanic or Latino, non-Hispanic or -Latino) had no effect on the pharmacokinetics of semaglutide.
Body weight: Body weight has an effect on the exposure of semaglutide. Higher body weight results in lower exposure; a 20% difference in body weight between individuals will result in an approximate 16% difference in exposure. Semaglutide doses of 0.5 mg and 1 mg provide adequate systemic exposure over a body weight range of 40-198 kg.
Renal impairment: Renal impairment did not impact the pharmacokinetics of semaglutide in a clinically relevant manner. This was shown with a single dose of 0.5 mg semaglutide for patients with different degrees of renal impairment (mild, moderate, severe or patients in dialysis) compared with subjects with normal renal function. This was also shown for subjects with type 2 diabetes and with renal impairment based on data from phase 3a studies, although the experience in patients with end-stage renal disease was limited.
Hepatic impairment: Hepatic impairment did not have any impact on the exposure of semaglutide. The pharmacokinetics of semaglutide were evaluated in patients with different degrees of hepatic impairment (mild, moderate, severe) compared with subjects with normal hepatic function in a study with a single-dose of 0.5 mg semaglutide.
Paediatric population: Semaglutide has not been studied in paediatric patients.
Toxicology: Preclinical safety data: Preclinical data reveal no special hazards for humans based on conventional studies of safety pharmacology, repeat-dose toxicity or genotoxicity.
Non-lethal thyroid C-cell tumours observed in rodents are a class effect for GLP-1 receptor agonists. In 2-year carcinogenicity studies in rats and mice, semaglutide caused thyroid C-cell tumours at clinically relevant exposures. No other treatment-related tumours were observed. The rodent C-cell tumours are caused by a non-genotoxic, specific GLP-1 receptor mediated mechanism to which rodents are particularly sensitive. The relevance for humans is considered to be low, but cannot be completely excluded.
In fertility studies in rats, semaglutide did not affect mating performance or male fertility. In female rats, an increase in oestrous cycle length and a small reduction in corpora lutea (ovulations) were observed at doses associated with maternal body weight loss.
In embryo-foetal development studies in rats, semaglutide caused embryotoxicity below clinically relevant exposures. Semaglutide caused marked reductions in maternal body weight and reductions in embryonic survival and growth. In foetuses, major skeletal and visceral malformations were observed, including effects on long bones, ribs, vertebrae, tail, blood vessels and brain ventricles. Mechanistic evaluations indicated that the embryotoxicity involved a GLP-1 receptor mediated impairment of the nutrient supply to the embryo across the rat yolk sac. Due to species differences in yolk sac anatomy and function, and due to lack of GLP-1 receptor expression in the yolk sac of non-human primates, this mechanism is considered unlikely to be of relevance to humans. However, a direct effect of semaglutide on the foetus cannot be excluded.
In developmental toxicity studies in rabbits and cynomolgus monkeys, increased pregnancy loss and slightly increased incidence of foetal abnormalities were observed at clinically relevant exposures. The findings coincided with marked maternal body weight loss of up to 16%. Whether these effects are related to the decreased maternal food consumption as a direct GLP-1 effect is unknown.
Postnatal growth and development were evaluated in cynomolgus monkeys. Infants were slightly smaller at delivery, but recovered during the lactation period.
In juvenile rats, semaglutide caused delayed sexual maturation in both males and females. These delays had no impact upon fertility and reproductive capacity of either sex, or on the ability of the females to maintain pregnancy.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image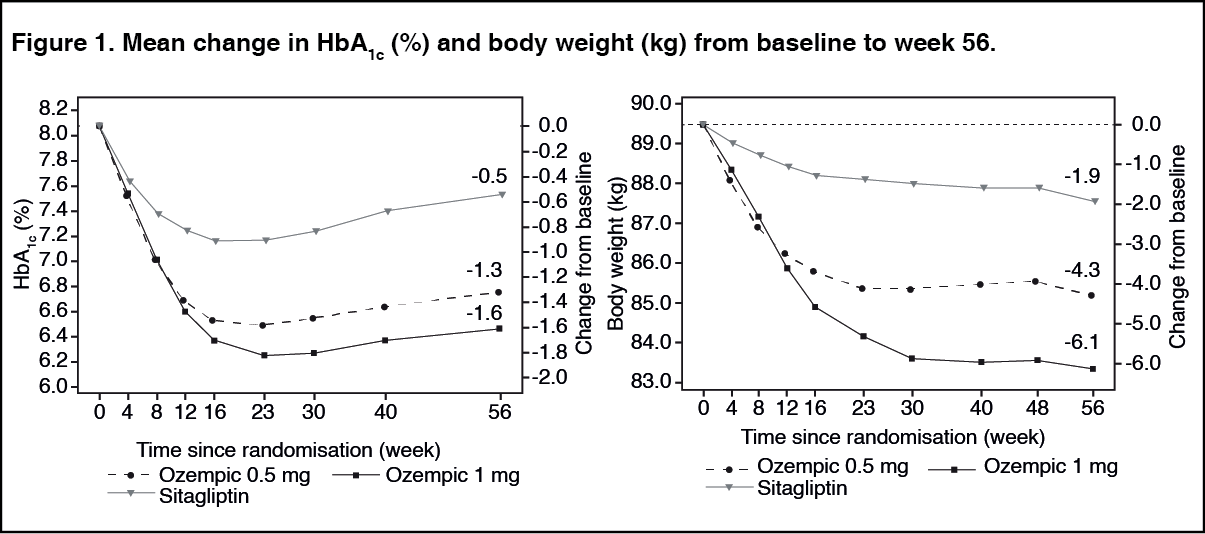 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image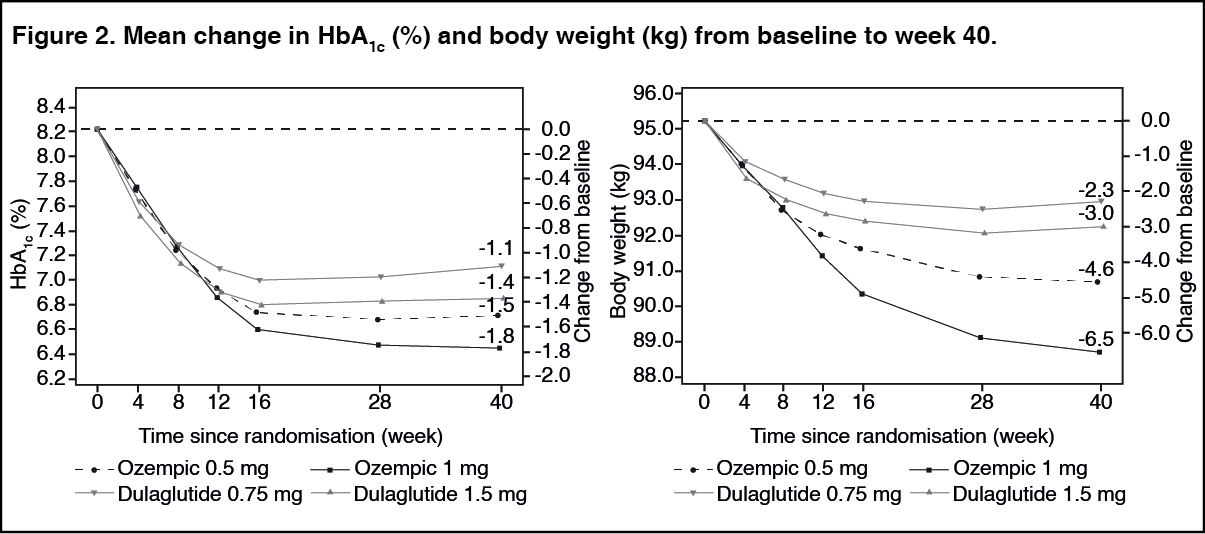 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image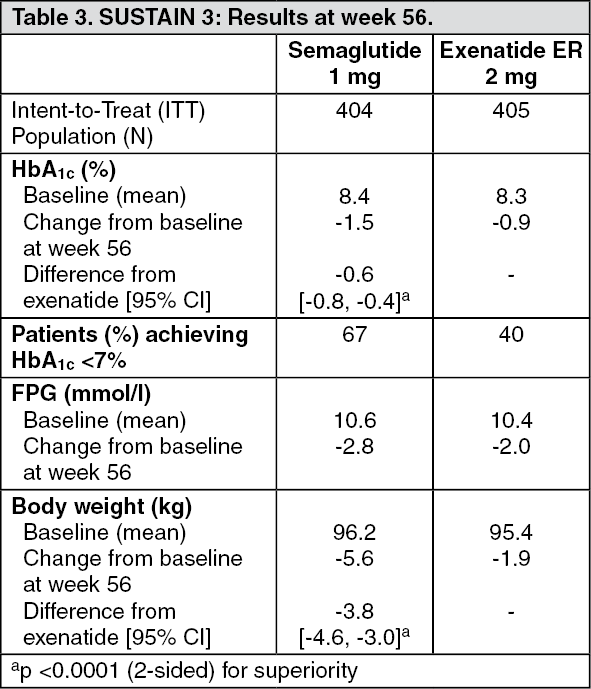 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
