Pharmacotherapeutic group: Antineoplastic agents-Protein-tyrosine kinase inhibitors.
ATC code: L01XE31.
Pharmacology: Mechanism of action: Nintedanib is a small molecule tyrosine kinase inhibitor including the receptors platelet-derived growth factor receptor (PDGFR) α and β, fibroblast growth factor receptor (FGFR) 1-3, and vascular endothelial growth factor receptor (VEGFR) 1-3. Nintedanib binds competitively to the ATP binding pocket of these receptors and blocks the intracellular signalling which is crucial for the proliferation, migration and transformation of fibroblasts representing essential mechanisms of the IPF pathology. In addition nintedanib inhibits Flt-3, Lck, Lyn and Src kinases.
Pharmacodynamic effects: Activation of FGFR and PDGFR signalling cascades is critically involved in proliferation and migration of lung fibroblasts/myofibroblasts, the hallmark cells in the pathology of idiopathic pulmonary fibrosis. The potential impact of VEGFR inhibition on IPF pathology is currently not fully elucidated. On the molecular level, nintedanib is thought to inhibit the FGFR and PDGFR signalling cascades mediating lung fibroblast proliferation and migration by binding to the adenosine triphosphate (ATP) binding pocket of the intracellular receptor kinase domain, thus interfering with cross-activation via auto-phosphorylation of the receptor homodimers. In vitro, the target receptors are inhibited by nintedanib in low nanomolar concentrations. In human lung fibroblasts from patients with IPF nintedanib inhibited PDGF-, FGF-, and VEGF-stimulated cell proliferation with EC
50 values of 11 nmol/L, 5.5 nmol/L and less than 1 nmol/L, respectively. At concentrations between 100 and 1000 nmol/L nintedanib also inhibited PDGF-, FGF-, and VEGF-stimulated fibroblast migration and TGF-β2-induced fibroblasts to myofibroblast transformation. In addition, the anti-inflammatory activity of nintedanib is thought to limit fibrotic stimulation by reduction of profibrotic mediators like IL-lβ and IL-6. The contribution of the anti-angiogenic activity of nintedanib to its mechanism of action in fibrotic lung diseases is currently not clarified. In in vivo studies, nintedanib was shown to have anti-fibrotic and anti-inflammatory activity.
Clinical Trials: The clinical efficacy of nintedanib has been studied in patients with IPF in two phase 3, randomised, double-blind, placebo-controlled studies with identical design (INPULSIS-1 and INPULSIS-2). Patients were randomized in a 3:2 ratio to treatment with Ofev 150 mg or placebo twice daily for 52 weeks.
The primary endpoint was the annual rate of decline in Forced Vital Capacity (FVC). The key secondary endpoints were change from baseline in Saint George's Respiratory Questionnaire (SGRQ) total score at 52 weeks and time to first acute IPF exacerbation.
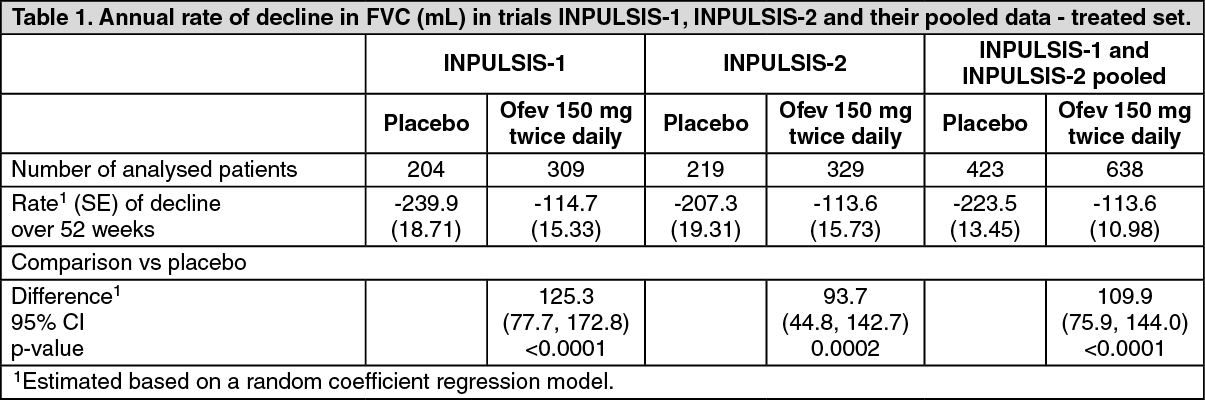
Annual rate of decline in FVC: The annual rate of decline of FVC (in mL) was significantly reduced in patients receiving nintedanib compared to patients receiving placebo. The treatment effect was consistent in both trials. See Table 1 for individual and pooled study results.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The robustness of the effect of nintedanib in reducing the annual rate of decline in FVC was confirmed in all pre-specified sensitivity analyses.
In addition, similar effects were observed on other lung function endpoints e.g. change from baseline in FVC at week 52 and FVC responder analyses providing further substantiation of the effects of nintedanib on slowing disease progression. See Figure for the evolution of change from baseline over time in both treatment groups, based on the pooled analysis of studies INPULSIS-1 and INPULSIS-2.
Click on icon to see table/diagram/image
FVC responder analysis: In both INPULSIS trials, the proportion of FVC responders, defined as patients with an absolute decline in FVC % predicted no greater than 5% (a threshold indicative of the increasing risk of mortality in IPF), was significantly higher in the nintedanib group as compared to placebo. Similar results were observed in analyses using a conservative threshold of 10%. See Table 2 for individual and pooled study results.
Click on icon to see table/diagram/image
Time to progression (≥10% absolute decline of FVC % predicted or death). In both INPULSIS trials, the risk of progression was statistically significantly reduced for patients treated with nintedanib compared with placebo. In the pooled analysis, the HR was 0.60 indicating a 40% reduction in the risk of progression for patients treated with nintedanib compared with placebo, see Table 3.
Click on icon to see table/diagram/image
Change from baseline in SGRQ total score at week 52: St. George's Respiratory Questionnaire (SGRQ) total score measuring health related quality of life (HRQoL) was analysed at 52 weeks. In INPULSIS-2, patients receiving placebo had a larger increase from baseline SGRQ total score as compared to patients receiving nintedanib 150 mg bid. The deterioration of HRQoL was smaller in the nintedanib group; the difference between the treatment groups was statistically significant (-2.69; 95% CI: -4.95, -0.43; p=0.0197).
In INPULSIS-1, the increase from baseline in SGRQ total score at week 52 was comparable between nintedanib and placebo (difference between treatment groups: -0.05; 95% CI: -2.50, 2.40; p=0.9657). In the pooled analysis of the INPULSIS trials, the estimated mean change from baseline to week 52 in SGRQ total score was smaller in the nintedanib group (3.53) than in the placebo group (4.96), with a difference between the treatment groups of -1.43 (95% CI: -3.09, 0.23; p=0.0923). Overall, the effect of nintedanib on health-related quality of life as measured by the SGRQ total score is modest, indicating less worsening compared to placebo.
Time to first acute IPF exacerbation: In the INPULSIS-2 trial, the risk of first acute IPF exacerbation over 52 weeks was significantly reduced in patients receiving nintedanib compared to placebo, in the INPULSIS-1 trial there was no difference in between the treatment groups. In the pooled analysis of the INPULSIS trials, a numerically lower risk of first acute exacerbation was observed in patients receiving nintedanib compared to placebo. See Table 4 for individual and pooled study results.
Click on icon to see table/diagram/image
All adverse events of acute IPF exacerbation reported by the investigator were adjudicated by a blinded adjudication committee. A pre-specified sensitivity analysis of the time to first 'suspected' adjudicated acute IPF exacerbation was performed on the pooled data. The frequency of patients with at least 1 adjudicated exacerbation occurring within 52 weeks was lower in the nintedanib group (1.9% of patients) than in the placebo group (5.7% of patients). Time to event analysis of the adjudicated exacerbation events using pooled data yielded an HR of 0.32 (95% CI 0.16, 0.65; p=0.0010).This indicates that the risk of having a first acute IPF exacerbation was statistically significantly lower in the nintedanib group than in the placebo group at any time point.
Survival analysis: In the pre-specified pooled analysis of survival data of the INPULSIS trials, overall mortality over 52 weeks was lower in the nintedanib group (5.5%) compared with the placebo group (7.8%). The analysis of time to death resulted in a HR of 0.70 (95% CI 0.43, 1.12; p=0.1399). The results of all survival endpoints (such as on-treatment mortality and respiratory mortality) showed a consistent numerical difference in favour of nintedanib (see Table 5).
Click on icon to see table/diagram/image
Supportive evidence from the phase II trial (1199.30) Ofev 150 mg twice daily results: Additional evidence of efficacy is provided by the randomised, double-blind, placebo-controlled, dose finding phase II trial including a nintedanib 150 mg bid dose group.
The primary endpoint, rate of decline in FVC over 52 weeks was lower in the nintedanib arm (-0.060 L/year, N=84) than the placebo arm (-0.190 L/year, N=83). The estimated difference between the treatment groups was 0.131 L/year (95% CI 0.027, 0.235). The difference between the treatment groups reached nominal statistical significance (p=0.0136).
The estimated mean change from baseline in SGRQ total score at 52 weeks was 5.46 for placebo, indicating worsening of the health-related quality of life and -0.66 for nintedanib, indicating stable health-related quality of life. The estimated mean difference for nintedanib compared with placebo was -6.12 (95% CI: -10.57, -1.67; p=0.0071).
The number of patients with acute IPF exacerbations over 52 weeks was lower in the nintedanib group (2.3%, N=86) compared to placebo (13.8%, N=87). The estimated hazard ratio of nintedanib versus placebo was 0.16 (95% CI 0.04, 0.71; p=0.0054).
QT interval: In a dedicated study in renal cell cancer patients, QT/QTc measurements were recorded and showed that a single oral dose of 200 mg nintedanib as well as multiple oral doses of 200 mg nintedanib administered twice daily for 15 days did not prolong the QTcF interval.
Paediatric population: The European Medicines Agency has waived the obligation to submit the results of studies with Ofev in all studies of the paedriatic population in IPF.
Pharmacokinetics: The pharmacokinetics (PK) of nintedanib can be considered linear with respect to time (i.e. single-dose data can be extrapolated to multiple-dose data). Accumulation upon multiple administrations was 1.04-fold for C
max and 1.38-fold for AUC
T. Nintedanib trough concentrations remained stable for more than one year.
Absorption: Nintedanib reached maximum plasma concentrations approximately 2-4 hours after oral administration as soft gelatin capsule under fed conditions (range 0.5-8 hours;). The absolute bioavailability of a 100 mg dose was 4.69 % (90 % CI: 3.615-6.078) in healthy volunteers. Absorption and bioavailability are decreased by transporter effects and substantial first-pass metabolism.
Dose proportionality was shown by increase of nintedanib exposure (dose range 50-450 mg once daily and 150-300 mg twice daily). Steady state plasma concentrations were achieved within one week of dosing at the latest.
After food intake, nintedanib exposure increased by approximately 20 % compared to administration under fasted conditions (CI: 95.3-152.5 %) and absorption was delayed (median t
max fasted: 2.00 hours; fed: 3.98 h).
Distribution: Nintedanib follows at least bi-phasic disposition kinetics. After intravenous infusion, a high volume of distribution (V
ss: 1050 L, 45.0 % gCV) was observed.
The
in vitro protein binding of nintedanib in human plasma was high, with a bound fraction of 97.8 %. Serum albumin is considered to be the major binding protein. Nintedanib is preferentially distributed in plasma with a blood to plasma ratio of 0.869.
Metabolism: The prevalent metabolic reaction for nintedanib is hydrolytic cleavage by esterases resulting in the free acid moiety BIBF 1202. BIBF 1202 is subsequently glucuronidated by UGT enzymes, namely UGT 1A1, UGT 1A7, UGT 1A8, and UGT 1A1O to BIBF 1202 glucuronide.
Only a minor extent of the biotransformation of nintedanib consisted of CYP pathways, with CYP 3A4 being the predominant enzyme involved. The major CYP-dependent metabolite could not be detected in plasma in the human ADME study.
In vitro, CYP-dependent metabolism accounted for about 5 % compared to about 25 % ester cleavage.
Elimination: Total plasma clearance after intravenous infusion was high (CL: 1390 mL/min, 28.8 % gCV). Urinary excretion of the unchanged active substance within 48 hours was about 0.05 % of dose (31.5 % gCV) after oral and about 1.4 % of the dose (24.2 % gCV) after intravenous administration; the renal clearance was 20 mL/min (32.6 % gCV). The major route of elimination of drug related radioactivity after oral administration of [
14C] nintedanib was via faecal/biliary excretion (93.4 % of dose, 2.61 % gCV). The contribution of renal excretion to the total clearance was low (0.649 % of dose, 26.3 % gCV). The overall recovery was considered complete (above 90 %) within 4 days after dosing. The terminal half-life of nintedanib was between 10 and 15 h (gCV % approximately 50 %;).
Exposure-response relationship: Exposure-response analyses indicated an E
max-like relationship between exposure in the range observed in Phase II and III and the annual rate of decline in FVC with an EC
5O of around 3-5 ng/mL (relative standard errors: 54-67%).
With respect to safety, there seemed to be a weak relationship between nintedanib plasma exposure and ALT and/or AST elevations. Actual administered dose might be the better predictor for the risk of developing diarrhea of any intensity, even if plasma exposure as risk determining factor could not be ruled out. (see Precautions).
Intrinsic and Extrinsic Factors; Special Populations: The PK properties of nintedanib were similar in healthy volunteers, patients with IPF, and cancer patients. Based on results of Population PK (PopPK) analyses and descriptive investigations, exposure to nintedanib was not influenced by sex (body weight corrected), mild and moderate renal impairment (estimated by creatinine clearance), liver metastases, ECOG performance score, alcohol consumption, or P-gp genotype. Population PK analyses indicated moderate effects on exposure to nintedanib depending on the following intrinsic and extrinsic factors. Based on the high inter-individual variability of exposure observed in the clinical trials these effects are not considered clinically relevant. (see Precautions).
Age: Exposure to nintedanib increased linearly with age. AUC
τ,ss decreased by 16 % for a 45-year old patient (5
th percentile) and increased by 13 % for a 76-year old patient (95
th percentile) relative to a patient with the median age of 62 years. The age range covered by the analysis was 29 to 85 years; approximately 5 % of the population was older than 75 years.
Studies in paediatric populations have not been performed.
Body weight: An inverse correlation between body weight and exposure to nintedanib was observed. AUC
τ,ss increased by 25 % for a 50 kg patient (5
th percentile) and decreased by 19 % for a 100 kg patient (95
th percentile) relative to a patient with the median weight of 71.5 kg.
Race: The geometric mean exposure to nintedanib was 33 % higher in Chinese, Taiwanese, and Indian patients while it was 22 % lower in Koreans compared to Caucasians (body weight corrected).
Data from Black individuals was very limited but in the same range as for Caucasians.
Hepatic impairment: In a dedicated single dose phase I study and compared to healthy subjects, exposure to nintedanib based on Cmax and AUC was 2.2-fold higher in volunteers with mild hepatic impairment (Child Pugh A; 90% CI 1.3-3.7 for Cmax and 1.2-3.8 for AUC, respectively). In volunteers with moderate hepatic impairment (Child Pugh B), exposure was 7.6-fold higher based on Cmax (90% CI 4.4-13.2) and 8.7-fold higher (90% CI 5.7-13.1) based on AUC, respectively, compared to healthy volunteers.
Subjects with severe hepatic impairment (Child Pugh C) have not been studied.
Concomitant treatment with pirfenidone: Concomitant treatment of nintedanib with pirfenidone was investigated in a parallel group design study in Japanese patients with IPF. Twenty four patients were treated for 28 days with 150 mg nintedanib bid. In 13 patients, nintedanib was added to chronic treatment with standard doses of pirfenidone. Eleven patients received nintedanib monotherapy. The exposure to nintedanib tended to be lower when nintedanib was administered on top of pirfenidone compared to administration of nintedanib alone. Nintedanib had no effect on the PK of pirfenidone. Due to the short duration of concomitant exposure and low number of patients no conclusion on the safety and efficacy of the combination can be drawn.
Drug-Drug Interaction Potential: Metabolism: Drug-drug interactions between nintedanib and CYP substrates, CYP inhibitors, or CYP inducers are not expected, since nintedanib, BIBF 1202, and BIBF 1202 glucuronide did not inhibit or induce CYP enzymes preclinically nor was nintedanib metabolized by CYP enzymes to a relevant extent.
Transport: Nintedanib is a substrate of P-gp. For the interaction potential of nintedanib with this transporter, see Interactions. Nintedanib was shown to be not a substrate or inhibitor of OATP-1B1, OATP-1B3, OATP-2B1, OCT-2 or MRP-2
in vitro. Nintedanib was also not a substrate of BCRP. Only a weak inhibitory potential on OCT-1, BCRP, and P-gp was observed
in vitro which is considered to be of low clinical relevance. The same applies for nintedanib being a substrate of OCT-1.
Toxicology: General toxicology: Single dose toxicity studies in rats and mice indicated a low acute toxic potential of nintedanib. In repeat dose toxicology studies in rats, adverse effects (e.g. thickening of epiphyseal plates, lesions of the incisors) were mostly related to the mechanism of action (i.e. VEGFR-2 inhibition) of nintedanib. These changes are known from other VEGFR-2 inhibitors and can be considered class effects.
Diarrhoea and vomiting accompanied by reduced food consumption and loss of body weight were observed in toxicity studies in non-rodents.
There was no evidence of liver enzyme increases in rats, dogs, and Cynomolgus monkeys. Mild liver enzyme increases which were not due to serious adverse effects such as diarrhoea were only observed in Rhesus monkeys.
Reproduction toxicity: A study of male fertility and early embryonic development up to implantation in rats did not reveal effects on the male reproductive tract and male fertility.
In rats, embryo-foetal lethality and teratogenic effects were observed at exposure levels below human exposure at the maximum recommended human dose (MRHD) of 150 mg twice daily. Effects on the development of the axial skeleton and on the development of the great arteries were also noted at subtherapeutic exposure levels.
In rabbits, embryofoetal lethality and teratogenic effects comparable to those in rats were observed at an exposure slightly higher than in rats
In rats, small amounts of radiolabelled nintedanib and/or its metabolites were excreted into the milk (≤0.5 % of the administered dose).
From the 2-year carcinogenicity studies in mice and rats, there was no evidence for a carcinogenic potential of nintedanib.
Genotoxicity studies indicated no mutagenic potential for nintedanib.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image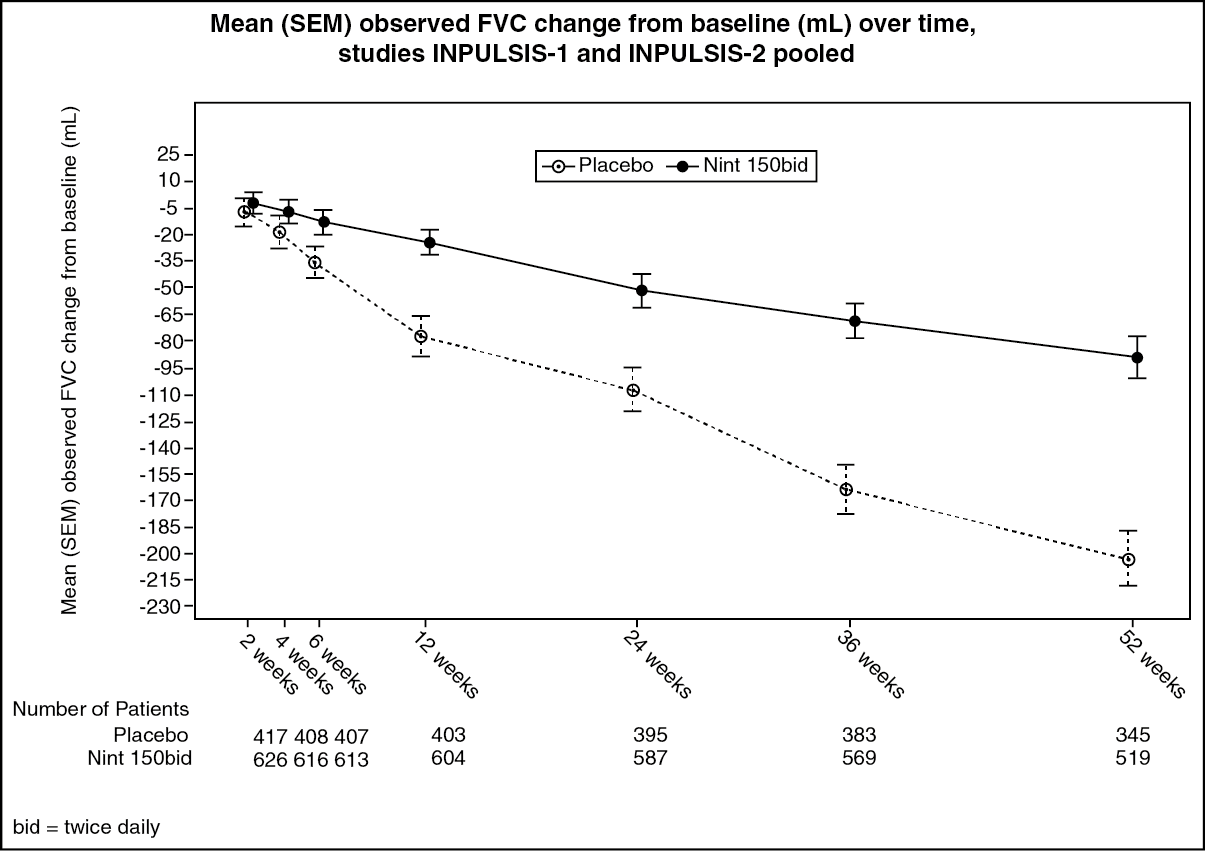 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image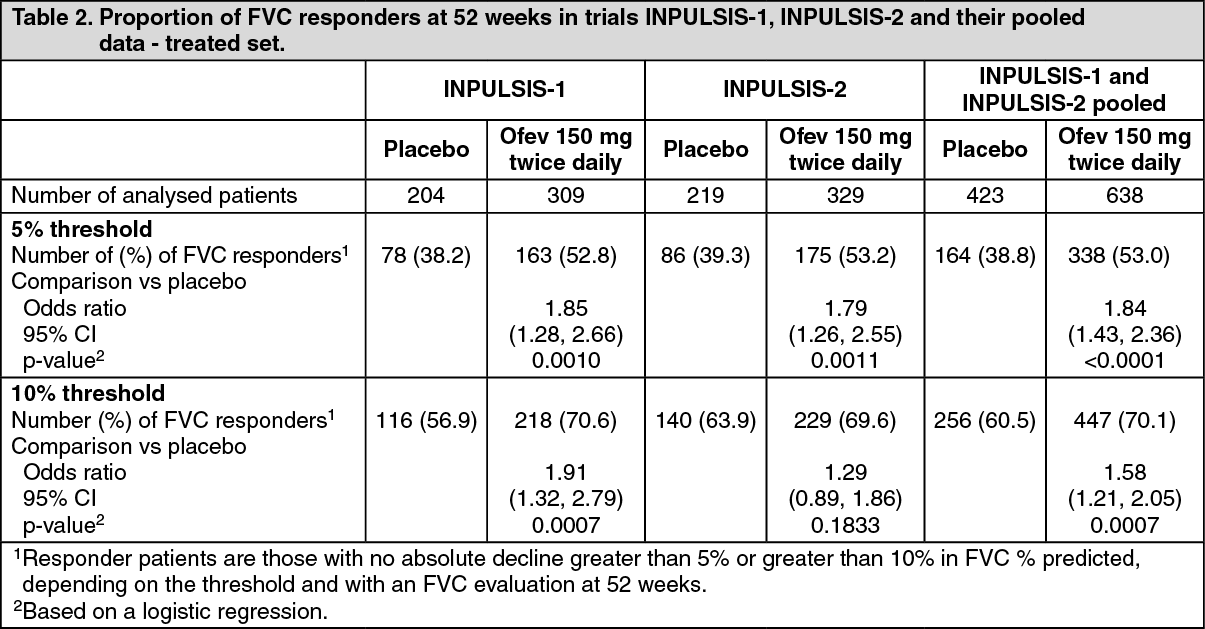 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image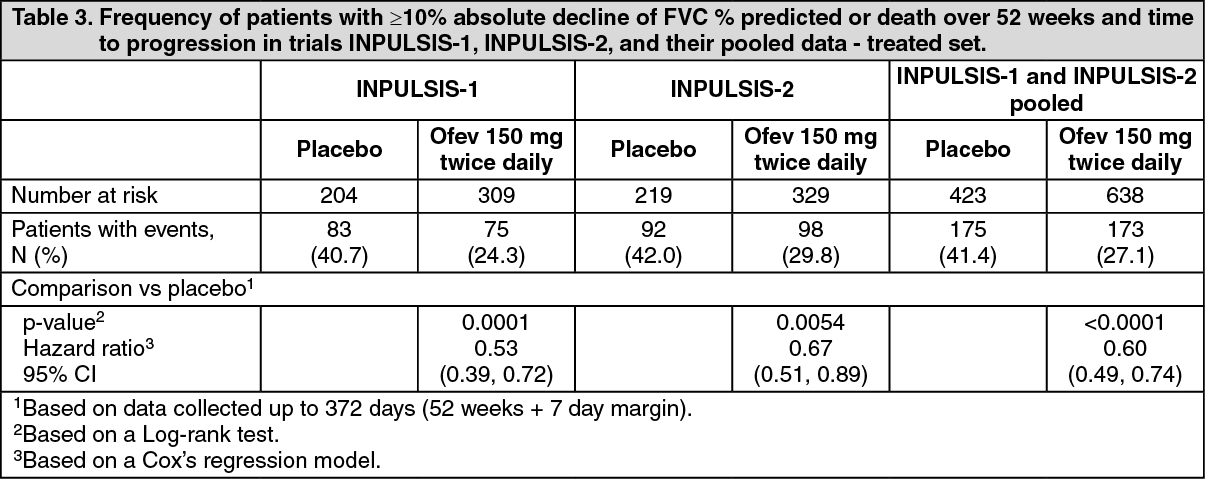 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image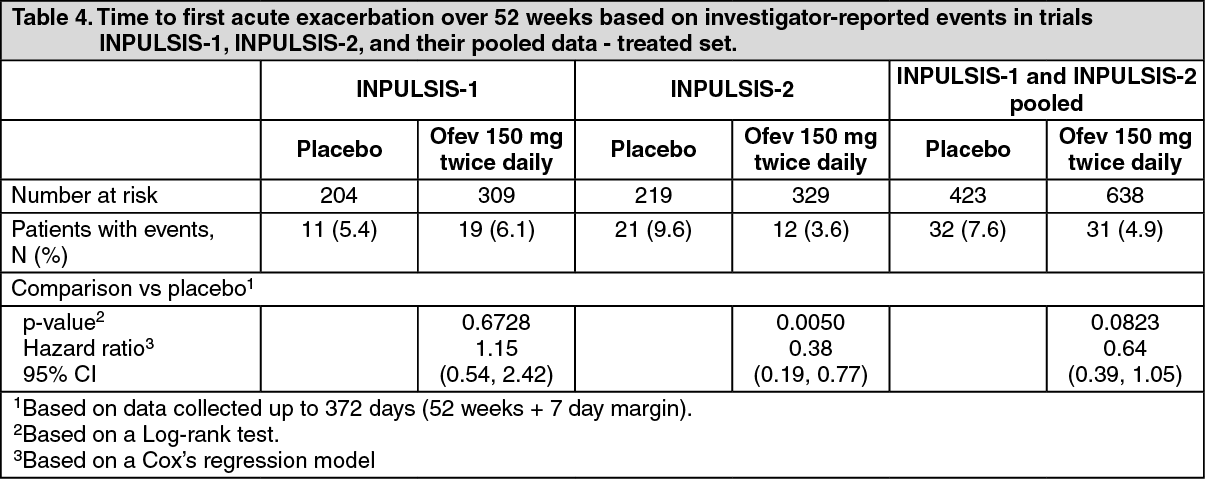 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image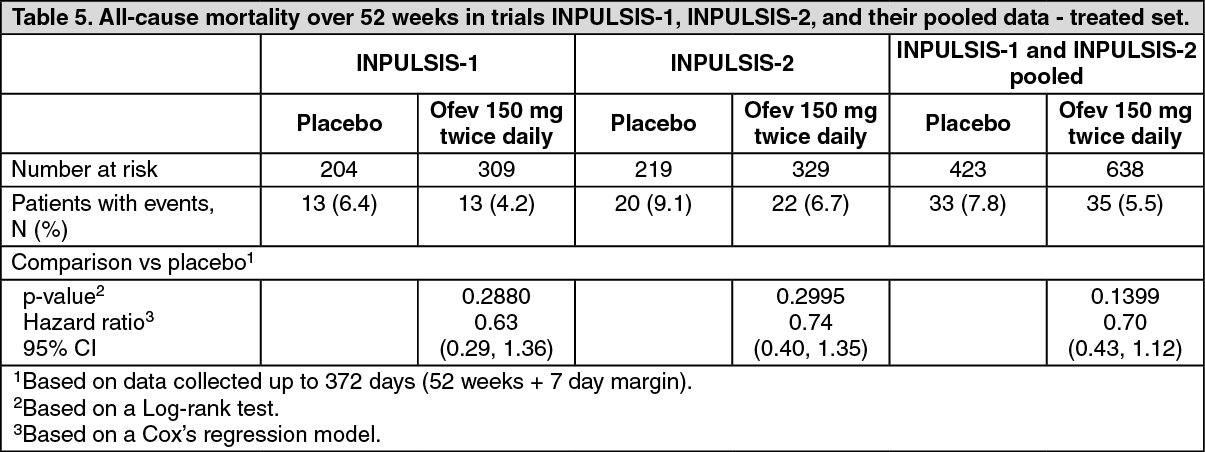 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
