Sofosbuvir 400 mg film-coated tablets treatment should be initiated and monitored by a physician experienced in the management of patients with CHC.
The recommended dose is one 400 mg tablet, taken orally, once daily with or without food. Sofosbuvir should be used in combination with other medicinal products. Monotherapy of Sofosbuvir is not recommended. The recommended regimen and treatment duration for Sofosbuvir combination therapy are provided in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patients with Genotype 1 HCV Who are Ineligible to Receive an Interferon-Based Regimen: Sofosbuvir in combination with ribavirin for 24 weeks can be considered as a therapeutic option for patients with genotype 1 infection who are ineligible to receive an interferon-based regimen. Treatment decision should be guided by an assessment of the potential benefits and risks for the individual patient.
Dose modification: Dose reduction of Sofosbuvir 400 mg film-coated tablets is not recommended.
If sofosbuvir is used in combination with peginterferon alfa, and a patient has a serious adverse reaction potentially related to this drug, the peginterferon alfa dose should be reduced or discontinued. Refer to the peginterferon alfa Summary of Product Characteristics for additional information about how to reduce and/or discontinue the peginterferon alfa dose.
If a patient has a serious adverse reaction potentially related to ribavirin, the ribavirin dose should be modified or discontinued, if appropriate, until the adverse reaction abates or decreases in severity. Table 2 provides guidelines for dose modifications and discontinuation based on the patient's haemoglobin concentration and cardiac status. (See Table 2.)
Click on icon to see table/diagram/image
Once ribavirin has been withheld due to either a laboratory abnormality or clinical manifestation, an attempt may be made to restart ribavirin at 600 mg daily and further increase the dose to 800 mg daily. However, it is not recommended that ribavirin be increased to the original assigned dose (1,000 mg to 1,200 mg daily).
Discontinuation of dosing: If the other medicinal products used in combination with Sofosbuvir 400 mg film-coated tablets are permanently discontinued, Sofosbuvir 400 mg film-coated tablets should also be discontinued (see Precautions).
Special population: No dose adjustment is warranted for elderly patients (see Pharmacology: Pharmacokinetics under Actions).
Renal impairment: No dose adjustment of Sofosbuvir 400 mg film-coated tablets is required for patients with mild or moderate renal impairment. The safety and appropriate dose of Sofosbuvir 400 mg film-coated tablets have not been established in patients with severe renal impairment (estimated glomerular filtration rate [eGFR] <30 mL/min/1.73 m
2) or end stage renal disease (ESRD) requiring haemodialysis.
Hepatic impairment: No dose adjustment of Sofosbuvir 400 mg film-coated tablets is required for patients with mild, moderate or severe hepatic impairment (Child-Pugh-Turcotte [CPT] class. A, B or C). The safety and efficacy of Sofosbuvir 400 mg film-coated tablets have not been established in patients with decompensated cirrhosis.
Patients awaiting liver transplantation: The duration of administration of Sofosbuvir 400 mg film-coated tablets in patients awaiting liver transplantation should be guided by an assessment of the potential benefits and risks for the individual patient (see Pharmacology: Pharmacodynamics under Actions).
Paediatric population: The safety and efficacy of Sofosbuvir 400 mg film-coated tablets in children and adolescents aged <18 years have not yet been established. No data are available.
Patients with Hepatocellular Carcinoma Awaiting Liver Transplantation: Administer Sofosbuvir in combination with ribavirin for up to 48 weeks or until the time of liver transplantation, whichever occurs first, to prevent post-transplant HCV reinfection.
Method of administration: The film-coated tablet is for oral use. Patients should be instructed to swallow the tablet whole. The film-coated tablet should not be chewed or crushed, due to the bitter taste of the active substance. The tablet should be taken with food (see Pharmacology: Pharmacokinetics under Actions).
Patients should be instructed that if vomiting occurs within 2 hours of dosing an additional tablet should be taken. If vomiting occurs more than 2 hours after dosing, no further dose is needed. These recommendations are based on the absorption kinetics of sofosbuvir and GS-331007 suggesting that the majority of the dose is absorbed within 2 hours after dosing.
If a dose is missed and it is within 18 hours of the normal time, patients should be instructed to take the tablet as soon as possible and then patients should take the next dose at the usual time. If it is after 18 hours then patients should be instructed to wait and take the next dose at the usual time. Patients should be instructed not to take a double dose.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image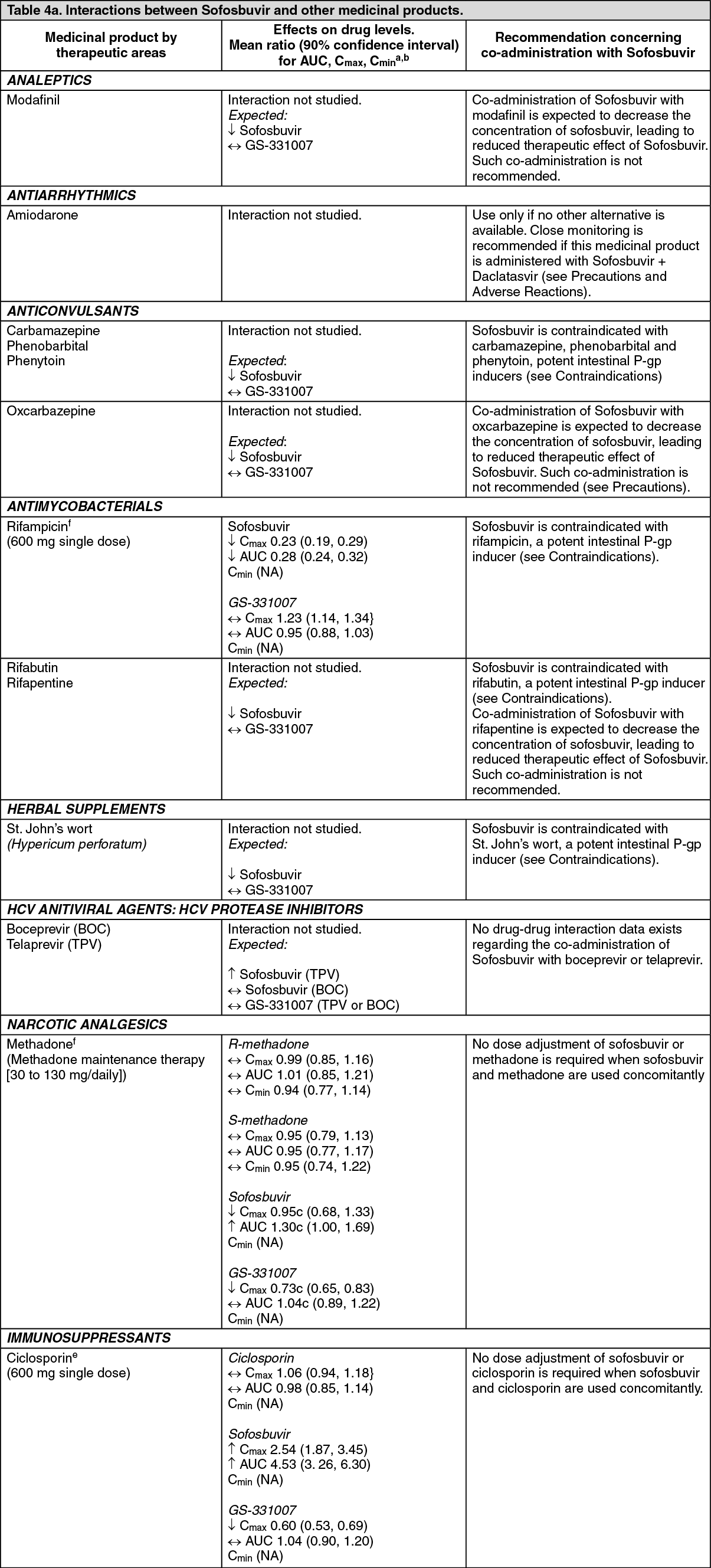 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image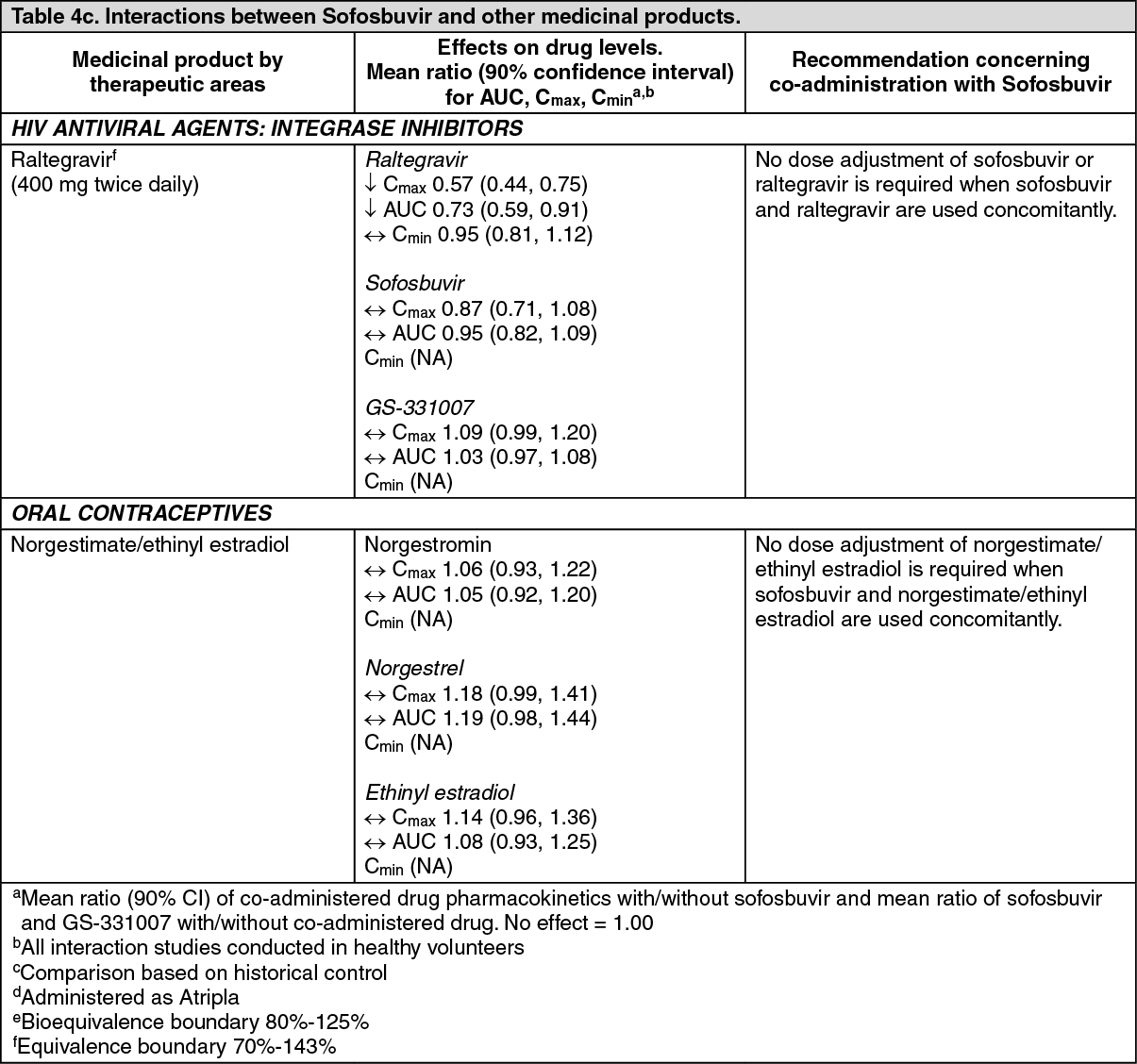 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
