Pharmacology: Pharmacodynamics: Mechanism of Action: Gardasil is a non-infectious recombinant quadrivalent vaccine prepared from the highly purified virus-like particles (VLPs) at the major capsid L1 protein of HPV types 6, 11, 16 and 18. The VLPs contain no viral DNA, they cannot infect cells, reproduce or cause disease. HPV only infects humans, but animal studies with analogous papillomaviruses suggest that the efficacy of L1 VLP vaccines is mediated by the development of a humoral immune response.
Of the HPV types in the vaccine, HPV 16 and 18 are responsible for approximately 70% of high-grade cervical dysplasia (CIN 2/3) and adenocarcinoma
in situ (AIS) cases, and approximately 70% of high-grade vulvar dysplasia (VIN 2/3) cases in young premenopausal females. HPV 16 and 18 are also responsible for a majority of high-grade squamous vaginal lesions (VaIN 2/3). Other HPV types not contained in the vaccine are responsible for 20-30% of remaining cases of CIN 2/3, VIN 2/3 and VaIN 2/3. CIN 3 is an accepted immediate precursor of invasive cervical cancer. VIN 3 is an important risk factor for the development of vulvar cancer in young premenopausal females infected with carcinogenic HPV types.
HPV 6 and 11 are responsible for approximately 90% of genital warts cases.
HPV 6, 11, 16 and 18 are responsible for 35-50% of CIN 1 or low-grade cervical dysplasia.
Clinical Studies: The efficacy of Gardasil was assessed in 4 placebo-controlled, double-blind, randomized phase II and III clinical studies including a total of 20,541 16- to 26-year old women, who were enrolled and vaccinated without pre-screening for the presence of HPV infection.
The primary efficacy endpoints induded HPV 6-, 11-, 16- or 18-related vulvar and vaginal lesions (genital warts, VIN, VaIN) and CIN of any grade (Protocol 013, Future I), HPV 16- or 18-related CIN 2/3 and AIS (Protocol 015, Future II) HPV 6-, 11-, 16- or 18-related persistent infection (Protocol 007), and HPV 16-related persistent infection (Protocol 005).
Cervical intraepithelial neoplasia (CIN) grade 2/3 (moderate- to high-grade dysplasia) was used in the clinical trials as a surrogate marker for cervical cancer.
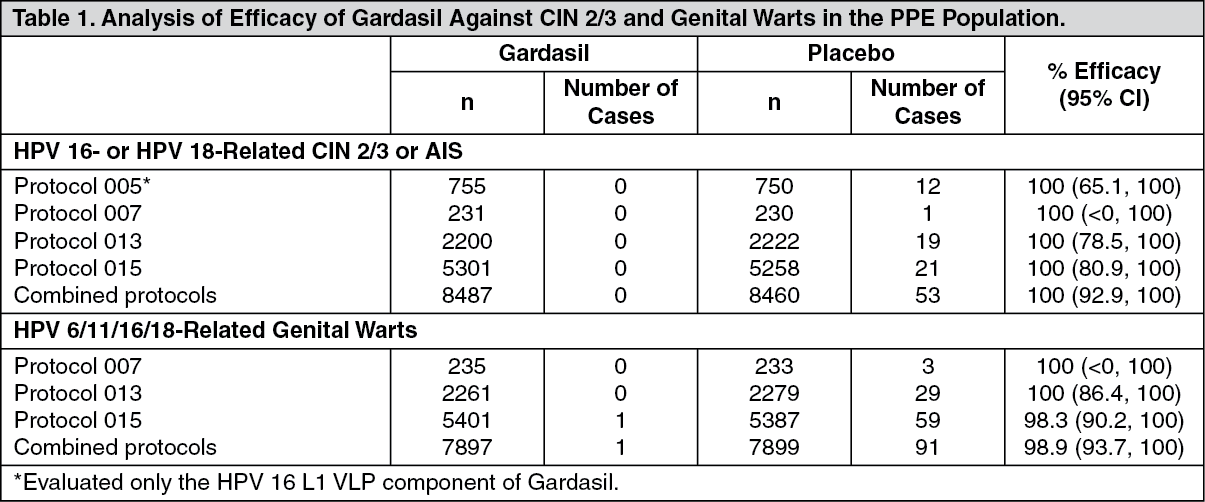
Prophylactic Efficacy: The primary analyses of efficacy were conducted in the per-protocol efficacy (PPE) population (n=all 3 vaccinations within 1 year of enrollment, no major protocol deviations and naive to the relevant HPV type(s) prior to dose 1 and through 1 month post-dose 3 (month 7). Efficacy was measured starting after the month 7 visit. Overall, 73% of subjects were naive (PCR negative and seronegative) to all 4 HPV types at enrollment.
Efficacy in Subjects Naive to the Relevant Vaccine HPV Type(s): The efficacy results for relevant endpoints in the per-protocol population are presented in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The efficacy of Gardasil against HPV 6-, 11-, 16-, 18-related CIN (1, 2, 3) or AIS was 100% (97.5% CI: 87.4, 100) in Protocol 013 where it was the primary endpoint and 95.2% (95% CI: 87.2, 98.7) in the combined protocols.
The efficacy of Gardasil against HPV 6-, 11-, 16-, 18-related CIN 1 was 100% (95% CI: 84.1, 100) in Protocol 013 and in the combined analysis, it was 93.1% (95% CI: 81.4, 98.2).
In the integrated analysis (Protocols 007, 013, 015), the efficacy of Gardasil against high-grade HPV 6-, 11-, 16- or 18-related vulvar lesions (VIN 2/3) was 100% (95% CI: 41.4, 100). Vaccine efficacy against high-grade vaginal lesions (VaIN 2/3) did not reach statistical significance. Altogether, there were 8 cases 1 VIN 2/3 and 5 cases of VaIN 2/3, all occurred in the placebo group.
On the basis of 12-month definition of persistent infection (ie, at least 2 positive specimens over a minimum interval of 12 months), the efficacy against persistent HPV 16 infection was 93.3% (95% CI: 79.1, 98.7) in Protocol 005. In Protocol 007, the efficacy of Gardasil against persistent HPV 16 or HPV 18 infection was 100% (95% CI: 43.3, 100). There were 6 cases of persistent HPV 16 infection, and 2 cases of persistent HPV 18 infection, all in the placebo group.
Efficacy in Subjects With Current or Prior Infection: There was no evidence of protection from disease caused by HPV types for which subjects were PCR positive and/or seropositive at baseline. However, individuals who were already infected with ≥1 vaccine-related HPV types prior to vaccination were protected from clinical disease caused by the remaining vaccine HPV types.
In the modified intention-to-treat (ITT) population, defined as women who received at least 1 vaccination regardless of baseline HPV status at day 1 with case counting starting at 1 month post-dose 1, the results are summarized in Table 2. This population approximates to the general population of women with respect to prevalence of HPV infection and disease at enrollment. (See Table 2.)
Click on icon to see table/diagram/image
The efficacy of Gardasil against HPV 6-, 11-, 18-related CIN (1, 2, 3) or AIS was 46.4% (95% CI: 35.2, 55.7) in this same population.
Overall, 12% of the combined study population had an abnormal Pap test suggestive of CIN at day 1. Among subjects with an abnormal Pap test at day 1 who were naive to the relevant vaccine HPV types at day 1, efficacy of Gardasil remained high. Among subjects with an abnormal Pap test at day 1 who were already infected with the relevant vaccine HPV types at day 1, no vaccine efficacy was observed.
Immunogenicity: Assays to Measure Immune Response: No minimum antibody level associated with protection has been identified for HPV vaccines.
The immunogenicity of Gardasil was assessed in 8915 (Gardasil n=4666; placebo n=4249) women 18-26 years and 3400 female (Gardasil n=1471; placebo n=583) and male (Gardasil n=1071: placebo n=275) adolescents 9-17 years.
Type-specific immunoassays, competitive Luminex-based immunoassay (cLIA), with type-specific standards were used to assess immunogenicity to each vaccine type. This assay measures antibodies against neutralizing epitopes for each HPV type.
Immune Responses to Gardasil: Overall, 99.9%, 99.8%, 99.8% and 99.6% of individuals who received Gardasil became anti-HPV 6, anti-HPV 11, anti-HPV 16 and anti-HPV 18 seropositive, respectively, by 1 month post-dose 3 across all age groups tested. Gardasil induced high anti-HPV Geometric Mean Titres (GMTs) 1 month post-dose 3 in all age group tested.
Anti-HPV levels in placebo subjects who had cleared an HPV infection (seropositive and PCR negative) were substantially lower than those induced by the vaccine. Furthermore, anti-HPV levels in vaccinated subjects remained higher during the long-term follow-up of the phase III studies.
Bridging the Efficacy of Gardasil to Young Adult Women to Young Adolescents: A clinical study (Protocol 016) compared the immunogenicity of Gardasil in 10- to 15-year-old boys and girls to those in 16- to 23-year old adolescent and young women. In the vaccine group, 99.1-100% became seropositive to all vaccine serotypes by 1 month post-dose 3.
Table 3 compares the 1 month post-dose 3 anti-HPV 6, 11, 16 and 18 GMTs in 9- to 15-year old boys and girls with those in 16- to 26-year old young women. (See Table 3.)
Click on icon to see table/diagram/image
Anti-HPV responses at month 7 among 9- to 15-year old girls and boys were non-inferior to anti-HPV responses in 16- to 26-year old young women for whom efficacy was established in the phase III studies. Immunogenicity was related to age and month 7 anti-HPV levels were significantly higher younger individuals <12 years than in those above that age.
On the basis of this immunogenicity bridging, the efficacy of Gardasil in 9- to 15-year old girls is inferred.
Immunogenicity and safety of Gardasil have been demonstrated in 9- to 15-year old boys. Protective efficacy has not been evaluated in males.
Persistence: In Protocol 007, peak anti-HPV 6, 11, 16, 18 GMTs were observed at month 7. The GMTs declined through month 24 and then stabilized until at least month 60. The observation period is currently limited to 2 years in the phase III trials of young women and 18 months in trials of adolescents. The exact duration of immunity following a 3-dose series has not been established.
Evidence of Anamnestic (Immune Memory) Response: Evidence of an anamnestic response was seen in vaccinated individuals who were seropositive to relevant HPV type(s) prior to vaccination. In addition, a subset of vaccinated individuals who received a challenge dose of Gardasil 5 years after the onset of vaccination, exhibited a rapid and strong anamnestic response that exceeded the anti-HPV GMTs observed 1 month post-dose 3.
Pharmacokinetics: Evaluation of pharmacokinetic studies is not required for vaccines.
Toxicology: Preclinical Safety Data: Single-dose and repeated-dose toxicity, and local tolerance studies revealed no special hazard to humans.
Gardasil induced specific antibody responses against HPV types 6, 11, 16 and 18 in pregnant rats, following 1 or multiple IM injections. Antibodies against all 4 HPV types were transferred to the offspring during gestation and possibly during lactation. There were no treatment-related effects on development signs, behavior, reproductive performance or fertility of the offspring.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image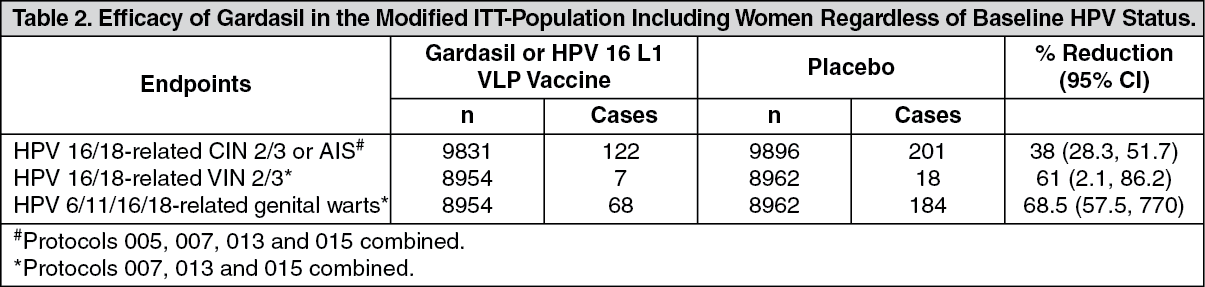 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image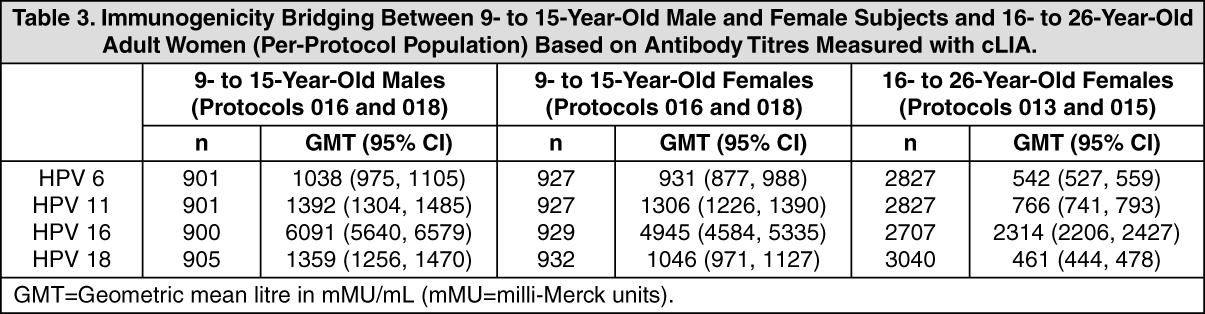 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image7db48ce9-139e-42d3-8d50-af0700df679b.GIF)

 Sign Out
Sign Out
