


 Sign Out
Sign Out



The primary assessment of safety and tolerability was conducted in a pre-specified pooled analysis of 13 short-term (up to 24 weeks) placebo-controlled studies, with 2,360 subjects treated with dapagliflozin 10 mg and 2,295 treated with placebo.
In the dapagliflozin cardiovascular outcomes study in type 2 diabetes mellitus (DECLARE study, see Pharmacology: Pharmacodynamics under Actions), 8,574 patients received dapagliflozin 10 mg and 8,569 received placebo for a median exposure time of 48 months. In total, there were 30,623 patient-years of exposure to dapagliflozin.
The most frequently reported adverse reactions across the clinical studies were genital infections.
Heart failure: In the dapagliflozin cardiovascular outcome study in patients with heart failure with reduced ejection fraction (DAPA-HF study), 2,368 patients were treated with dapagliflozin 10 mg and 2,368 patients with placebo for a median exposure time of 18 months. The patient population included patients with type2 diabetes mellitus and without diabetes, and patients with eGFR≥30mL/min/1.73m2.
The overall safety profile of dapagliflozin inpatients with heart failure was consistent with the known safety profile of dapagliflozin.
Chronic kidney disease: In the dapagliflozin renal outcome study in patients with chronic kidney disease (DAPA-CKD), 2,149 patients were treated with dapagliflozin 10 mg and 2,149 patients with placebo for a median exposure time of 27 months. The patient population included patients with type 2 diabetes mellitus and without diabetes, with eGFR ≥ 25 to ≤ 75 mL/min/1.73 m2, and albuminuria (urine albumin creatinine ratio [UACR] ≥ 200 and ≤ 5000 mg/g). Treatment was continued if eGFR fell to levels below 25 mL/min/1.73 m2.
The overall safety profile of dapagliflozin in patients with chronic kidney disease was consistent with the known safety profile of dapagliflozin.
Tabulated list of adverse reactions: The following adverse reactions have been identified in the placebo-controlled clinical studies and postmarketing. None were found to be dose-related. Adverse reactions listed as follows are classified according to frequency and system organ class (SOC). Frequency categories are defined according to the following convention: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000), not known (cannot be estimated from the available data). (See Table 8.)
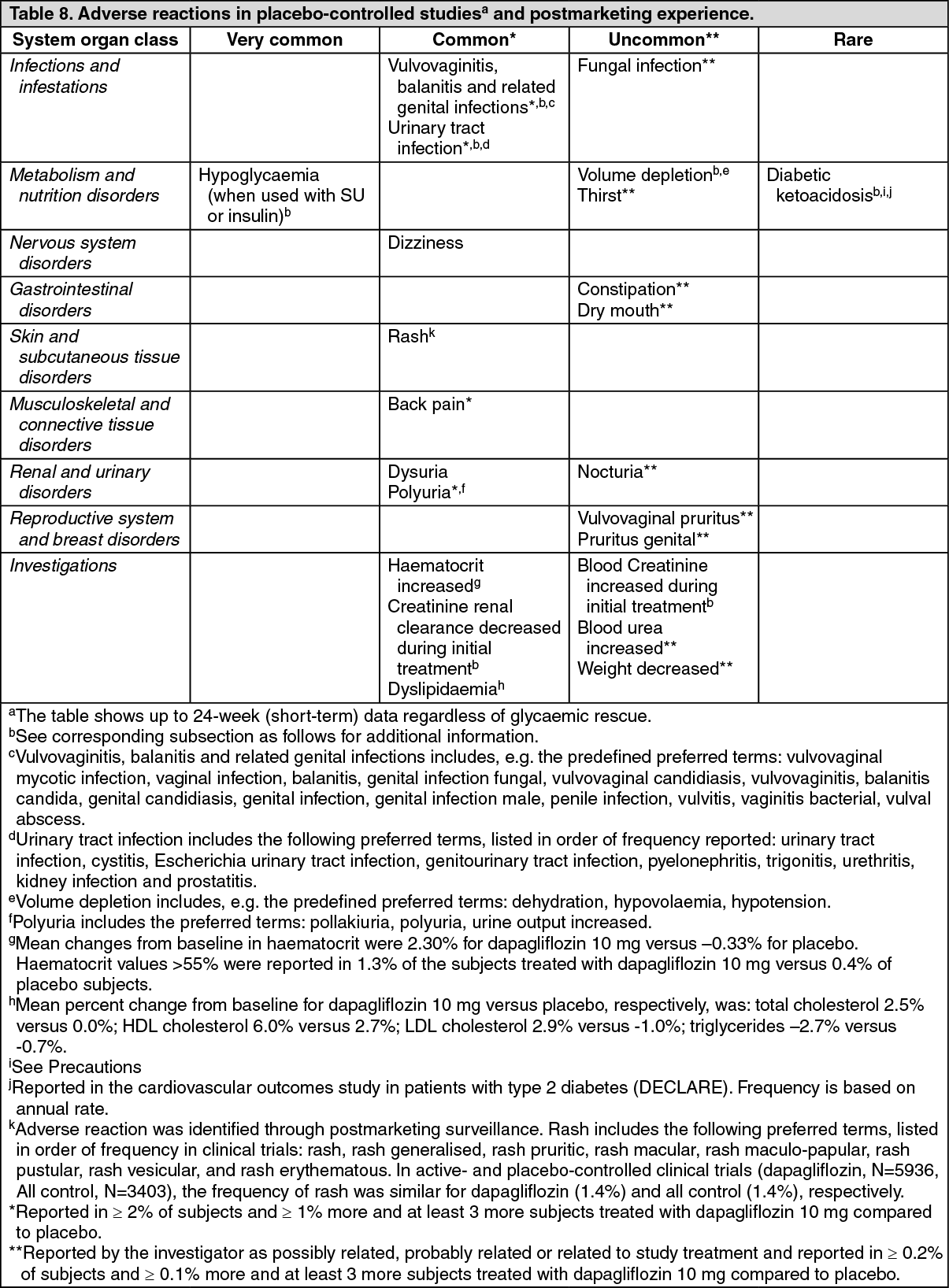 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional adverse reactions in ≥5% of patients treated with dapagliflozin 10 mg, ≥1% more than patients in placebo/comparator, and reported in at least three or more patients treated with dapagliflozin 10 mg, and regardless of relationship to dapagliflozin as reported by investigator, are described as follows by treatment regimen.
In add-on to metformin studies: headache (5.3% dapagliflozin 10 mg and 3.1% placebo).
In an add-on to thiazolidinedione study: nasopharyngitis (7.9% dapagliflozin 10 mg and 3.6% placebo), diarrhea (6.4% dapagliflozin 10 mg and 4.3% placebo).
Description of selected adverse reactions: Hypoglycaemia: The frequency of hypoglycaemia depended on the type of background therapy used in the clinical studies in diabetes mellitus.
For studies of dapagliflozin as add-on to metformin, add-on to pioglitazone or as add-on to sitagliptin (with metformin or without metformin), the frequency of minor episodes of hypoglycaemia was similar (< 5%) between treatment groups, including placebo up to 102 weeks of treatment. Across all studies, major events of hypoglycaemia were uncommon and comparable between the groups treated with dapagliflozin or placebo. Studies with add-on sulphonylurea and add on insulin therapies had higher rates of hypoglycaemia (see Interactions).
In an add-on to glimepiride study, at weeks 24 and 48, minor episodes of hypoglycaemia were reported more frequently in the group treated with dapagliflozin 10 mg plus glimepiride (6.0% and 7.9%, respectively) than in the placebo plus glimepiride group (2.1% and 2.1%, respectively).
In an add-on to metformin and a sulphonylurea study, up to 24 weeks, no episodes of major hypoglycaemia were reported. Minor episodes of hypoglycaemia were reported in 12.8% of subjects who received dapagliflozin 10 mg plus metformin and a sulphonylurea and in 3.7% of subjects who received placebo plus metformin and a sulphonylurea.
In an add-on to insulin study, episodes of major hypoglycaemia were reported in 0.5% and 1.0% of subjects treated with dapagliflozin 10 mg plus insulin at Weeks 24 and 104, respectively, and in 0.5% of subjects treated with placebo plus insulin groups at Weeks 24 and 104. At Weeks 24 and 104, minor episodes of hypoglycaemia were reported, respectively, in 40.3% and 53.1% of subjects who received dapagliflozin 10 mg plus insulin and in 34.0% and 41.6% of the subjects who received placebo plus insulin.
In the DECLARE study, no increased risk of major hypoglycaemia was observed with dapagliflozin therapy compared with placebo. Major events of hypoglycaemia were reported in 58 patients (0.7%) treated with dapagliflozin and 83 (1.0%) patients treated with placebo.
In the DAPA-HF study, major events of hypoglycaemia were reported in 4 (0.2%) patients in both the dapagliflozin and placebo treatment groups and observed only in patients with type 2 diabetes mellitus.
In the DAPA-CKD study, major events of hypoglycaemia were reported in 14 (0.7%) patients in the dapagliflozin group and 28 (1.3%) patients in the placebo group and observed only in patients with type 2 diabetes mellitus.
Volume depletion: Reactions related to volume depletion (including, reports of dehydration, hypovolaemia or hypotension) were reported in 1.1% and 0.7% of subjects who received dapagliflozin 10 mg and placebo, respectively; serious reactions occurred in < 0.2% of subjects balanced between dapagliflozin 10 mg and placebo (see Precautions).
In the dapagliflozin DECLARE study, the numbers of patients with events suggestive of volume depletion were balanced between treatment groups: 213 (2.5%) and 207 (2.4%) in the dapagliflozin and placebo groups, respectively. Serious adverse events were reported in 81 (0.9%) and 70 (0.8%) in the dapagliflozin and placebo group, respectively. Events were generally balanced between treatment groups across subgroups of age, diuretic use, blood pressure and angiotensin-converting enzyme inhibitor/angiotensin receptor blocker use. In patients with eGFR < 60 mL/min/1.73 m2 at baseline, there were 19 events of serious adverse events suggestive of volume depletion in the dapagliflozin group and 13 events in the placebo group.
In the DAPA-HF study, the numbers of patients with events suggestive of volume depletion were 170 (7.2%) in the dapagliflozin group and 153 (6.5%) in the placebo group. There were fewer patients with serious events of symptoms suggestive of volume depletion in the dapagliflozin group (23 [1.0%]) compared with the placebo group (38 [1.6%]). Results were similar irrespective of presence of diabetes at baseline and baseline eGFR.
In the DAPA-CKD study, the numbers of patients with events suggestive of volume depletion were 120 (5.6%) in the dapagliflozin group and 84 (3.9%) in the placebo group. There were 16 (0.7%) patients with serious events of symptoms suggestive of volume depletion in the dapagliflozin group and 15 (0.7%) patients in the placebo group.
Diabetic ketoacidosis in type 2 diabetes mellitus: In the DECLARE study, with a median exposure time of 48 months, events of DKA were reported in 27 patients in the dapagliflozin 10 mg group and 12 patients in the placebo group. The events occurred evenly distributed over the study period. Of the 27 patients with DKA events in the dapagliflozin group, 22 had concomitant insulin treatment at the time of the event. Precipitating factors for DKA were as expected in a type 2 diabetes mellitus population (see Precautions).
In the DAPA-HF study, events of DKA were reported in 3 patients with type 2 diabetes mellitus in the dapagliflozin group and none in the placebo group.
In the DAPA-CKD study, events of DKA were not reported in any patient in the dapagliflozin group and in 2 patients with type 2 diabetes mellitus in the placebo group.
Vulvovaginitis, balanitis and related genital infections: In the 13-study safety pool, vulvovaginitis, balanitis and related genital infections were reported in 5.5% and 0.6% of subjects who received dapagliflozin 10 mg and placebo, respectively. Most infections were mild to moderate, and subjects responded to an initial course of standard treatment and rarely resulted in discontinuation from dapagliflozin treatment. These infections were more frequent in females (8.4% and 1.2% for dapagliflozin and placebo, respectively), and subjects with a prior history were more likely to have a recurrent infection.
In the DECLARE study, the numbers of patients with serious adverse events of genital infections were few and balanced: 2 patients in each of the dapagliflozin and placebo groups.
In the DAPA-HF study, no patient reported serious adverse events of genital infections in the dapagliflozin group and one in the placebo group. There were 7 (0.3%) patients with adverse events leading to discontinuations due to genital infections in the dapagliflozin group and none in the placebo group.
In the DAPA-CKD study, there were 3 (0.1%) patients with serious adverse events of genital infections in the dapagliflozin group and none in the placebo group. There were 3 (0.1%) patients with adverse events leading to discontinuation due to genital infections in the dapagliflozin group and none in the placebo group. Serious adverse events of genital infections or adverse events leading to discontinuation due to genital infections were not reported for any patients without diabetes.
Urinary tract infections: Urinary tract infections were more frequently reported for dapagliflozin 10 mg compared to placebo (4.7% versus 3.5%, respectively; see Precautions). Most infections were mild to moderate, and subjects responded to an initial course of standard treatment and rarely resulted in discontinuation from dapagliflozin treatment. These infections were more frequent in females, and subjects with a prior history were more likely to have a recurrent infection.
In the dapagliflozin DECLARE study, serious events of urinary tract infections were reported less frequently for dapagliflozin 10 mg compared with placebo, 79 (0.9%) events versus 109 (1.3%) events, respectively.
In the DAPA-HF study, the numbers of patients with serious adverse events of urinary tract infections were 14 (0.6%) in the dapagliflozin group and 17 (0.7%) in the placebo group. There were 5 (0.2%) patients with adverse events leading to discontinuations due to urinary tract infections in each of the dapagliflozin and placebo groups.
In the DAPA-CKD study, the numbers of patients with serious adverse events of urinary tract infections were 29 (1.3%) in the dapagliflozin group and 18 (0.8%) in the placebo group. There were 8 (0.4%) patients with adverse events leading to discontinuations due to urinary tract infections in the dapagliflozin group and 3 (0.1%) in the placebo group. The numbers of patients without diabetes reporting serious adverse events of urinary tract infections or adverse events leading to discontinuation due to urinary tract infections were similar between treatment groups (6 [0.9%] versus 4 [0.6%] for serious adverse events, and 1 [0.1%] versus 0 for adverse events leading to discontinuation, in the dapagliflozin and placebo groups, respectively).
Increased creatinine: Adverse drug reactions related to increased creatinine were grouped (e.g. decreased renal creatinine clearance, renal impairment, increased blood creatinine and decreased glomerular filtration rate). In the 13-study safety pool, this grouping of reactions was reported in 3.2% and 1.8% of patients who received dapagliflozin 10 mg and placebo, respectively. In patients with normal renal function or mild renal impairment (baseline eGFR ≥ 60 mL/min/1.73 m2) this grouping of reactions were reported in 1.3% and 0.8% of patients who received dapagliflozin 10 mg and placebo, respectively. These reactions were more common in patients with baseline eGFR ≥ 30 and < 60 mL/min/1.73m2 (18.5% dapagliflozin 10 mg vs 9.3% placebo).
Further evaluation of patients who had renal-related adverse events showed that most had serum creatinine changes of ≤ 0.5 mg/dL from baseline. The increases in creatinine were generally transient during continuous treatment or reversible after discontinuation of treatment.
In the dapagliflozin cardiovascular outcomes study, including elderly patients and patients with renal impairment (eGFR less than 60 mL/min/1.73 m2), eGFR decreased over time in both treatment groups. At 1 year, mean eGFR was slightly lower, and at 4 years, mean eGFR was slightly higher in the dapagliflozin group compared with the placebo group.
In the DAPA-HF study, eGFR decreased over time in both the dapagliflozin group and the placebo group. The initial decrease in mean eGFR was -4.3 mL/min/1.73 m2 in the dapagliflozin group and -1.1 mL/min/1.73 m2 in the placebo group. At 20 months, change from baseline in eGFR was similar between the treatment groups: -5.3 mL/min/1.73 m2 for dapagliflozin and -4.5 mL/min/1.73 m2 for placebo.
In the DAPA-CKD study, eGFR decreased over time in both the dapagliflozin group and the placebo group. The initial (day 14) decrease in mean eGFR was -4.0 mL/min/1.73 m2 in the dapagliflozin group and -0.8 mL/min/1.73 m2 in the placebo group. At 28 months, change from baseline in eGFR was -7.4 mL/min/1.73 m2 in the dapagliflozin group and -8.6 mL/min/1.73 m2 in the placebo group.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
View ADR Monitoring Form