Ezetrol is a new class of lipid-lowering compounds that selectively inhibit the intestinal absorption of cholesterol and related plant sterols.
Pharmacology: Mechanism of Action: Ezetimibe is orally active and potent, with a unique mechanism of action that differs from other classes of cholesterol-reducing compounds [eg, statins, bile acid sequestrants (resins), fibric acid derivatives and plant stanols]. The molecular target of ezetimibe is the sterol transporter, Niemann-Pick C1-Like 1 (NPC1L1), which is responsible for the intestinal uptake of cholesterol and phytosterols.
Ezetimibe localizes at the brush border of the small intestine and inhibits the absorption of cholesterol, leading to a decrease in the delivery of intestinal cholesterol to the liver. This causes a reduction of hepatic cholesterol stores and an increase in clearance of cholesterol from the blood. Ezetimibe does not increase bile acid excretion (like bile acid sequestrants) and does not inhibit cholesterol synthesis in the liver (like statins).
In a 2-week clinical study in 18 hypercholesterolemic patients, Ezetrol inhibited intestinal cholesterol absorption by 54%, compared with placebo. By inhibiting the absorption of intestinal cholesterol, ezetimibe reduces the delivery of cholesterol to the liver. Statins reduce cholesterol synthesis in the liver. Together, these distinct mechanisms provide complementary cholesterol reduction. Ezetrol, administered with a statin, reduces total cholesterol (total-C), low-density lipoprotein cholesterol (LDL-C), apolipoprotein B (Apo B), triglycerides (TG) and increases high-density lipoprotein cholesterol (HDL-C) in patients with hypercholesterolemia, beyond either treatment alone. Administration of Ezetrol with fenofibrate is effective in improving serum total-C, LDL-C, Apo B, TG, HDL-C and non-HDL-C in patients with mixed hyperlipidemia. The effect of ezetemibe given either alone or in addition to an HMG-CoA reductase inhibitor or cardiovascular morbidity and mortality have not been established.
Clinical studies demonstrate that elevated levels of total-C, LDL-C and Apo B, the major protein constituent of LDL, promote human atherosclerosis. In addition, decreased levels of HDL-C are associated with the development of atherosclerosis. Epidemiologic studies have established that cardiovascular morbidity and mortality vary directly with the levels of total-C and LDL-C and inversely with the level of HDL-C. Like LDL, cholesterol-enriched triglyceride-rich lipoproteins, including very low-density lipoproteins (VLDL), intermediate-density lipoproteins (IDL) and remnants can also promote atherosclerosis. The independent effect of raising HDL-C or lowering TG on the risk of coronary and cardiovascular morbidity and mortality has not been determined.
A series of preclinical studies was performed to determine the selectivity of ezetimibe for inhibiting cholesterol absorption. Ezetimibe inhibited the absorption of [
14C]-cholesterol with no effect on the absorption of triglycerides, fatty acids, bile acids, progesterone, ethinyl estradiol, or the fat-soluble vitamins A and D.
Animal Pharmacology: The hypocholesterolemic effect of ezetimibe was evaluated in Rhesus monkeys, a model for the human metabolism of cholesterol, as well as in dogs. Rhesus monkeys were fed a cholesterol-containing diet that mimics a human Western diet. Ezetimibe was found to have an ED
50 of 0.0005 mg/kg/day for inhibiting the rise in plasma cholesterol levels (ED
100=0.003 mg/kg/day). The ED
50 in dogs was found to be 0.007 mg/kg/day. These results are consistent with Ezetrol being an extremely potent cholesterol absorption inhibitor.
In dogs given ezetimibe (≥0.03 mg/kg/day), the concentration of cholesterol in gallbladder bile increased ~2- to 3-fold. However, a dose of 300 mg/kg/day administered to dogs for 1 year did not result in gallstone formation or any adverse hepatobiliary effect. In mice given ezetimibe (0.3-5 mg/kg/day) and fed a normal or cholesterol-rich diet, the concentration of cholesterol in gallbladder bile was either unaffected or reduced to normal levels, respectively. The relevance of these preclinical findings to humans is unknown.
Pharmacokinetics: Absorption: After oral administration, ezetimibe is rapidly absorbed and extensively conjugated to a pharmacologically active phenolic glucuronide (ezetimibe-glucuronide). Mean maximum plasma concentrations (C
max) occur within 1-2 hrs for ezetimibe-glucuronide and 4-12 hrs for ezetimibe. The absolute bioavailability of ezetimibe cannot be determined as the compound is virtually insoluble in aqueous media suitable for injection.
Concomitant food administration (high-fat or nonfat meals) had no effect on the oral bioavailability of ezetimibe when administered as Ezetrol 10-mg tablets. Ezetrol can be administered with or without food.
Distribution: Ezetimibe and ezetimibe-glucuronide are bound 99.7% and 88-92% to human plasma proteins, respectively.
Metabolism: Ezetimibe is metabolized primarily in the small intestine and liver via glucuronide conjugation (a phase II reaction) with subsequent biliary excretion. Minimal oxidative metabolism (a phase I reaction) has been observed in all species evaluated. Ezetimibe and ezetimibe-glucuronide are the major drug-derived compounds detected in plasma, constituting approximately 10-20% and 80-90% of the total drug in plasma, respectively. Both ezetimibe and ezetimibe-glucuronide are slowly eliminated from plasma with evidence of significant enterohepatic recycling. The t
½ for ezetimibe and ezetimibe-glucuronide is approximately 22 hrs.
Elimination: Following oral administration of
14C-ezetimibe (20 mg) to human subjects, total ezetimibe accounted for approximately 93% of the total radioactivity in plasma. Approximately 78% and 11% of the administered radioactivity were recovered in the feces and urine, respectively, over a 10-day collection period. After 48 hrs, there were no detectable levels of radioactivity in the plasma.
Characteristics in Patients (Special Populations): Pediatric Patients: The absorption and metabolism of ezetimibe are similar between children and adolescents (10-18 years) and adults. Based on total ezetimibe, there are no pharmacokinetic differences between adolescents and adults. Pharmacokinetic data in the pediatric population <10 years of age are not available. Clinical experience in pediatric and adolescent patients (9-17 years) has been limited to patients with HoFH.
Geriatric Patients: Plasma concentrations for total ezetimibe are about 2-fold higher in the elderly (≥65 years) than in the young (18-45 years). LDL-C reduction and safety profile are comparable between elderly and young subjects treated with Ezetrol. Therefore, no dosage adjustment is necessary in the elderly.
Hepatic Insufficiency: After a single 10-mg dose of ezetimibe, the mean area under the curve (AUC) for total ezetimibe was increased approximately 1.7-fold in patients with mild hepatic insufficiency (Child-Pugh score 5 or 6), compared to healthy subjects. In a 14-day, multiple-dose study (10 mg daily) in patients with moderate hepatic insufficiency (Child-Pugh score 7-9), the mean AUC for total ezetimibe was increased approximately 4-fold on Day 1 and Day 14 compared to healthy subjects. No dosage adjustment is necessary for patients with mild hepatic insufficiency. Due to the unknown effects of the increased exposure to ezetimibe in patients with moderate or severe (Child-Pugh score >9) hepatic insufficiency, ezetimibe is not recommended in these patients (see Precautions).
Renal Insufficiency: After a single 10-mg dose of ezetimibe in patients with severe renal disease (n=8; mean creatinine clearance ≤30 mL/min/1.73 m
2), the mean AUC for total ezetimibe was increased approximately 1.5-fold, compared to healthy subjects (n=9). This result is not considered clinically significant. No dosage adjustment is necessary for renally impaired patients.
An additional patient in this study (post-renal transplant and receiving multiple medications, including cyclosporine) had a 12-fold greater exposure to total ezetimibe.
Gender: Plasma concentrations for total ezetimibe are slightly higher (<20%) in women than in men. LDL-C reduction and safety profile are comparable between men and women treated with ezetimibe. Therefore, no dosage adjustment is necessary on the basis of gender.
Race: Based on a meta-analysis of pharmacokinetic studies, there were no pharmacokinetic differences between Blacks and Caucasians.
Clinical Studies: Primary Hypercholesterolemia Monotherapy: In 2 multicenter, double-blind, placebo-controlled 12-week studies in 1719 patients with primary hypercholesterolemia, Ezetrol 10 mg significantly lowered total-C, LDL-C, Apo B and TG and increased HDL-C compared to placebo (see Table 1). Reduction in LDL-C was consistent across age, sex, race and baseline LDL-C. In addition, Ezetrol had no effect on the plasma concentrations of the fat-soluble vitamins A, D and E, had no effect on prothrombin time and did not impair adrenocortical steroid hormone production.
 Click on icon to see table/diagram/image
Co-Administration with a Statin:
Click on icon to see table/diagram/image
Co-Administration with a Statin: Ezetrol Initiated Concurrently with a Statin: In 4 multicenter, double-blind, placebo-controlled, 12-week trials in 2382 patients with hypercholesterolemia, Ezetrol 10 mg or placebo was administered alone or with various doses of atorvastatin, simvastatin, pravastatin or lovastatin. In general, the incremental effect on LDL-C reduction was independent of the dose or specific statin used. In addition, LDL-C reduction for Ezetrol co-administered with the lowest tested dose (10 mg) of any of the statins was similar to or greater than the LDL-C reduction of the highest tested dose of the corresponding statin administered alone (see Table 2).
Click on icon to see table/diagram/image
In a pooled analysis of all Ezetrol + statin doses, Ezetrol had a beneficial effect on total-C, Apo B, TG and HDL-C (see Table 3).
Click on icon to see table/diagram/image
Ezetrol Added to Ongoing Statin Therapy: In a multicenter, double-blind, placebo-controlled, 8-week study, 769 patients with hypercholesterolemia already receiving statin monotherapy and not at National Cholesterol Education Program (NCEP) LDL-C goal (100-160 mg/dL, depending on baseline characteristics) were randomized to receive either Ezetrol 10 mg or placebo in addition to their ongoing statin therapy.
Among statin-treated patients not at LDL-C goal at baseline (~82%), LDL-C goal at study endpoint was achieved by 72% and 19% of patients randomized to Ezetrol and placebo, respectively.
Ezetrol, added to ongoing statin therapy, significantly lowered total-C, LDL-C, Apo B and TG and increased HDL-C, compared with placebo (see Table 4). LDL-C reductions were consistent across all statins.
Click on icon to see table/diagram/image
Ezetrol or placebo added to statin therapy reduced median C-reactive protein by 10% or 0% from the baseline, respectively.
In a multicenter, double-blind 14-week study, 621 patients with hypercholesterolemia receiving atorvastation 10 mg daily with an LDL-C >130 mg/dL were randomized to receive atorvastatin 20 mg or Ezetrol 10 mg added to atorvastatin 10-mg therapy. The atorvastatin dose could be titrated up to 80 mg in the atorvastatin arm and up to 40 mg in the Ezetrol plus atorvastatin co-administration arm, based on patients not attaining LDL-C goal (<100 mg/dL). The mean baseline LDL-C was 187 mg/dL and approximately 60% of the patients had heterozygous familial hypercholesterolemia (HeFH). At study end, there was a significant difference in attainment of LDL-C goal between patients in the Ezetrol co-administration arm (22%) and patients on atorvastatin monotherapy (7%). At week 4, there was a significant difference in LDL-C reductions between co-administration patients (24%; Ezetrol + atorvastatin 10 mg) and monotherapy patients (9%; atorvastatin 20 mg). In the subgroup of patients with HeFH, similar results for LDL-C goal attainment and LDL-C reductions were achieved.
In a similarly designed study in 100 patients with hypercholesterolemia receiving simvastatin 20 mg and not at LDL-C goal, the addition of Ezetrol 10 mg to simvastatin titration compared to titration of simvastatin alone produced similar advantages to those observed in the atorvastatin study described previously. For example, significant differences in LDL-C goal attainment (27% for Ezetrol + simvastatin vs 3% for simvastatin alone) and LDL-C reductions (24% for Ezetrol + simvastatin vs 11% for simvastatin alone) were achieved.
Homozygous Familial Hypercholesterolemia (HoFH): A study was conducted to assess the efficacy of Ezetrol in the treatment of HoFH. This double-blind, randomized 12-week study enrolled 50 patients with a clinical and/or genotypic diagnosis of HoFH, with or without concomitant LDL apheresis, already receiving atorvastatin or simvastatin (40 mg). Patients were randomized to 1 of 3 treatment groups, atorvastatin or simvastatin (80 mg), Ezetrol 10 mg administered with atorvastatin or simvastatin (40 mg), or Ezetrol 10 mg administered with atorvastatin or simvastatin (80 mg). Results are shown in Table 5. Ezetrol, administered with atorvastatin (40 or 80 mg) or simvastatin (40 or 80 mg), significantly reduced LDL-C compared with increasing the dose of simvastatin or atorvastatin monotherapy from 40-80 mg.
Click on icon to see table/diagram/image
Co-Administration with Fenofibrate: In a multicenter, double-blind, placebo-controlled clinical study in patients with mixed hyperlipidemia, 625 patients were treated for up to 12 weeks and 576 for up to 1 year. Patients were randomized to receive placebo, Ezetrol alone, fenofibrate 160 mg alone, or Ezetrol and fenofibrate 160 mg.
Ezetrol co-administered with fenofibrate significantly lowered total-C, LDL-C, Apo B and non-HDL-C compared to fenofibrate administered alone. The percent decrease in TG and percent increase in HDL-C for Ezetrol co-administered with fenofibrate were comparable to those for fenofibrate administered alone (see Table 6).
Click on icon to see table/diagram/image
Improvements in lipid endpoints after 1 year of treatment were consistent with the 12-week data mentioned previously.
Toxicology: Acute Toxicity: In animals, no toxicity was observed after single oral doses of ezetimibe 5000 mg/kg in rats and mice and 3000 mg/kg in dogs.
Chronic Toxicity: Ezetimibe was well tolerated by mice, rats and dogs. No target organs of toxicity were identified in chronic studies at daily doses up to 1500 (males) and 500 mg/kg (females) in rats, up to 500 mg/kg in mice, or up to 300 mg/kg in dogs.
The safety of concomitant administration of ezetimibe and statins was assessed in rats and dogs. When ezetimibe was co-administered with atorvastatin, simvastatin, pravastatin or lovastatin, for 3 months, toxicologic findings were consistent with those seen with statins administered alone.
Carcinogenicity: In 2-year studies conducted in mice and rats, ezetimibe was not carcinogenic.
Mutagenicity: Ezetimibe was not genotoxic in a series of
in vivo and
in vitro tests.
Combinations of ezetimibe with atorvastatin, simvastatin, pravastatin or lovastatin were not genotoxic in a series of
in vitro and
in vivo assays.
Reproduction: Ezetimibe did not affect the fertility of male or female rats.
Development: Ezetamibe was not teratogenic in rats or rabbits and had no effect on prenatal or postnatal development.
Concomitant administration of ezetimibe and statins was not teratogenic in rats. In pregnant rabbits, a low incidence of skeletal malformations (fused sternebrae, fused caudal vertebrae, reduced number of caudal vertebrae) was observed when ezetimibe (1000 mg/kg; ≥146 times the human exposure at 10 mg daily based on AUC
0-24hrs for total ezetimibe) was administered with lovastatin (2.5 and 25 mg/kg), simvastatin (5 and 10 mg/kg), pravastatin (25 and 50 mg/kg), or atorvastatin (5, 25 and 50 mg/kg). Exposure to the pharmacologically active form of the statin ranged from 1.4 (atorvastatin) to 547 (lovastatin) times the human exposure at 10 mg daily (simvastatin or atorvastatin) or 20 mg daily (lovastatin or pravastatin) based on AUC
0-24hrs.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image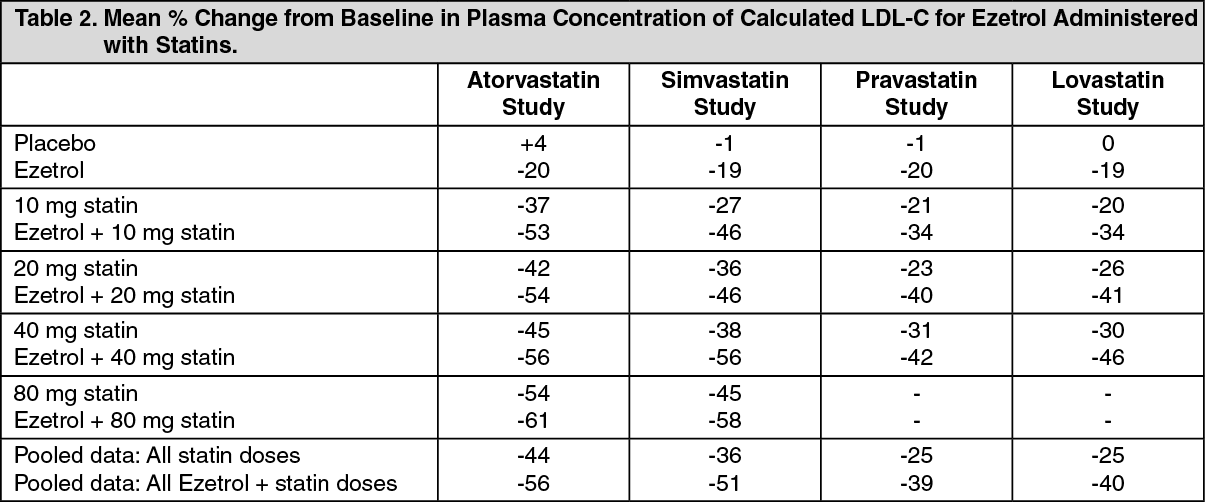 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image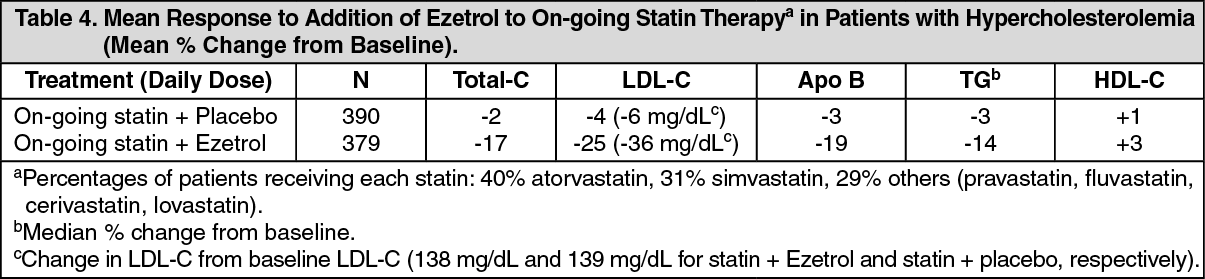 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image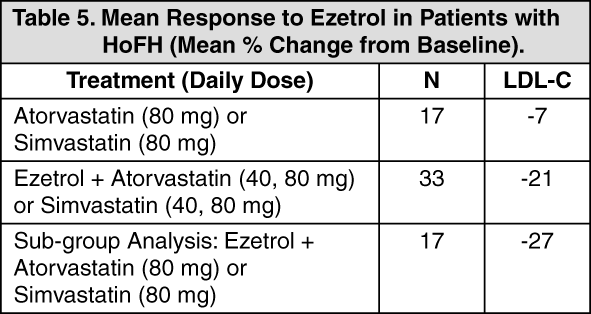 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image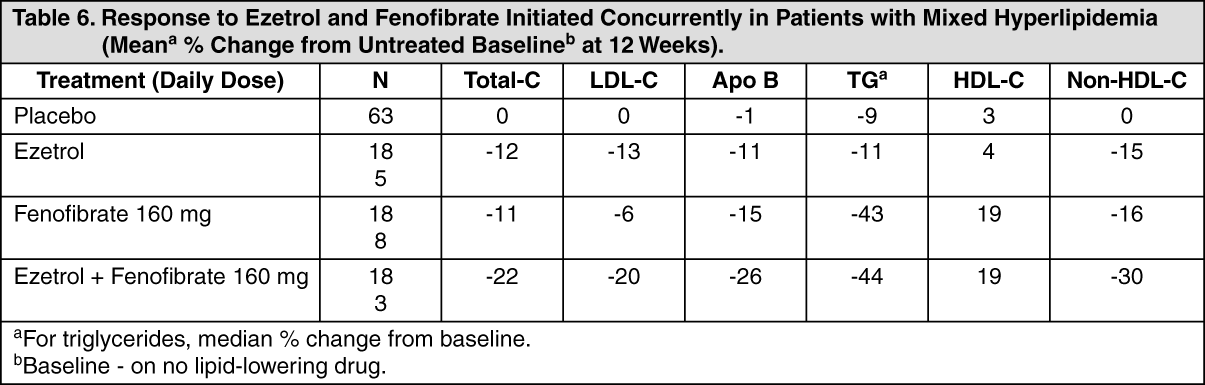 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
