Pharmacology: Mechanism of Action: In a calcium influx assay, Ki values of lemborexant for human orexin receptor types 1 (OX1) and 2 (OX2) were 8.1 nmol/L and 0.48 nmol/L, respectively. The metabolite M10, which can be found in human plasma, displayed binding affinity at orexin receptors comparable to that of unchanged drug.
Lemborexant is presumed to shift the brain from wakefulness state to sleep state by reversibly blocking the binding of wake-promoting neuropeptides orexin A and orexin B to the receptors OX1 and OX2, thereby inducing sleep.
Effects on Sleep: Lemborexant reduced sleep latency and increased total sleep time in rats. No significant difference was noted in the ratio of rapid eye movement (REM) sleep time to total sleep time.
Pharmacodynamics: Clinical Studies: Phase III Clinical Study (Study 303): Study 303 was a randomized, double-blind, parallel-group study involving patients with insomnia (n=949: Japanese, n=161; adults [18-64 years old], n=687; and elderly [≥65 years old], n=262) consisting of treatment period 1 (6 months of treatment with placebo as control) followed by treatment period 2 (6 months of treatment with lemborexant in all subjects). Of the 949, 315 patients were randomized to lemborexant 10 mg, a dose that is not approved for use. Patient-reported, subjective assessments of sleep onset latency, sleep efficiency, and wake after sleep onset using sleep diaries in treatment period 1 are shown in Tables 2, 3 and 4; administrations of DAYVIGO at 5 mg, as compared with placebo, led to statistically significant differences after 6 months of treatment (primary assessment time point). (See Tables 2, 3 and 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Clinical Pharmacology Studies: Effects on Driving Performance (Study 106): A total of 24 healthy adult male/female subjects (median age, 49 years), including 1 Japanese subject, and 24 healthy elderly male/female subjects (median age, 67 years) received DAYVIGO 5 or 10 mg before bedtime and were evaluated for effects on driving performance the next morning (approximately 9 h after taking the drug). With DAYVIGO administered at 5 or 10 mg over 8 days, no statistically significant effects on driving performance after one or multiple doses were noted in either healthy adult or healthy elderly subjects as compared to placebo.
Effects on Postural Stability and Cognitive Functions During The Night and The Next Morning (Studies 108 and 304) (Data from Non-Japanese Subjects): Healthy subjects (≥55 years old) received DAYVIGO 5 or 10 mg before bedtime and were evaluated for the effects on postural stability and cognitive functions (attention and memory) upon awakening during the night (approximately 4 h after administration of DAYVIGO) and upon awakening the next morning (approximately 8 h after administration of DAYVIGO). Approximately 4 h after administration of DAYVIGO, as compared with placebo, increased body sway was noted with DAYVIGO 5 and 10 mg, and decreased attention and memory were noted with DAYVIGO 10 mg. Moreover, in patients with insomnia (≥55 years old) receiving DAYVIGO 5 or 10 mg before bedtime, decreased attention was noted upon awakening the next morning (approximately 8 h after administration) with DAYVIGO 5 and 10 mg, as compared with placebo. There was no effect of DAYVIGO on tests of memory or body sway in the morning.
Respiratory Safety (Study 102) (Data from Non-Japanese Subjects): In a study of healthy adult and elderly patients, there were no differences between placebo and lemborexant 10 mg and 25 mg with respect to oxygen saturation during sleep. In a study of patients with mild sleep apnea, there was no effect of lemborexant on the apnea-hypopnea index when compared with placebo following single and multiple doses of lemborexant 10 mg. (See Careful Administration under Precautions.)
Effects on Drug Abuse (Study 103) (Data from Non-Japanese Subjects): With administration of DAYVIGO at 10, 20 or 30 mg in healthy adults (n=39) with experience of drug abuse, subjective assessments regarding DAYVIGO drug preference and other tendencies toward abuse were higher than those with placebo and similar to those with zolpidem at 30 mg and suvorexant at 40 mg.
Note: The approved dose of DAYVIGO is 5 mg.
Pharmacokinetics: Plasma Concentration: The plasma concentration-time profile after administration of DAYVIGO 10 mg on Day 14 in healthy Japanese adult males who received the drug repeatedly for 14 days at 2.5, 10 or 25 mg once daily are shown in Figure 1. The pharmacokinetic parameters at Day 1 and Day 14 in those who received DAYVIGO 10 mg shown in Table 5. The maximum concentration (C
max) and area under the concentration-time curve from 0 to 24 hours (AUC
(0-24h)) of lemborexant increased with increasing dose. C
max was 70.2 ng/mL, and plasma lemborexant concentrations at 3 and 8 hours postdose were 31.4 ng/mL and 17.9 ng/mL, respectively, on Day 14 after administration of 10 mg. (See figure and Table 5.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Effects of Meals (Data from Non-Japanese Subjects): In 24 non-Japanese healthy adults who received DAYVIGO at 10 mg orally as a single dose, the geometric mean ratios (fed/fasted) with 90% confidence intervals (CIs) for C
max and AUC
(0-t) of lemborexant were 0.771 (0.687, 0.866) and 1.18 (1.09, 1.28), respectively. C
max was 23% lower and AUC
(0-t) was 18% higher under fed conditions compared with fasted conditions. Furthermore, t
max (median) was delayed by 2 hours. The terminal elimination half-life (mean) of lemborexant was 50.8 h under fasted conditions and 53.8 h under fed conditions. (See Precautions related to dosage and administration under Dosage & Administration.)
Distribution: The plasma protein binding (
in vitro in human plasma) was 87.4-88.7% at concentrations of 100 to 1000 ng/mL.
Metabolism: Lemborexant was mainly eliminated from the body through metabolism, with the metabolite with systemic exposure greater than 10% of total drug-related exposure being M10 (N-oxide) alone (13%). M10 was confirmed to contribute to a lesser extent to the pharmacological effects than lemborexant.
An
in vitro metabolism study showed that CYP3A is mainly involved in the metabolism of lemborexant. Furthermore, M10 was shown to be generated by oxidative metabolism of lemborexant via CYP3A.
Excretion (Data from Non-Japanese Subjects): In 8 healthy non-Japanese adult males who received
14C-labelled lemborexant at 10 mg orally as a single dose, the total recovery rate for radioactivity was 86.5%, with 57.4% excreted in feces and 29.1% in urine.
Special Population (Data from Non-Japanese Subjects): Elderly: In 5 healthy elderly subjects (66-76 years) who received DAYVIGO repeatedly for 14 days at 25 mg once daily, geometric mean ratios (healthy elderly/healthy adult) with 90% confidence intervals for C
max and AUC
(0-24h) of lemborexant on Day 14 were 1.18 [0.770, 1.79] and 1.12 [0.762, 1.64], respectively. C
max and AUC
(0-24h) were 18% and 12% higher in elderly subjects than in healthy adult subjects, respectively. The terminal elimination half-life (mean) of lemborexant was 49.6 h in healthy adult subjects and 60.1 h in healthy elderly subjects. In population pharmacokinetic analysis involving healthy adult subjects and patients with insomnia in phase I-III clinical studies, apparent clearance of lemborexant was 26% lower in elderly subjects (≥65 years old). (See Use in the Elderly under Precautions.)
Patients with Hepatic Function Disorder: In 8 patients with mild hepatic function disorder (Child-Pugh score: 5-6) and 8 patients with moderate hepatic function disorder (Child-Pugh score: 7-9) who received DAYVIGO at 10 mg as a single dose, geometric mean ratios (patients with hepatic function disorder/healthy adults) with 90% CIs for C
max of lemborexant were 1.58 [1.18, 2.11] and 1.22 [0.915, 1.63], respectively, and those for AUC
(0-inf) were 1.25 [0.880, 1.78] and 1.54 [1.06, 2.22], respectively. C
max was 58% and 22% higher and AUC
(0-inf) was 25% and 54% higher in patients with mild hepatic function disorder and those with moderate hepatic function disorder, respectively, than in healthy adults. The terminal elimination half-lives (mean) of lemborexant were 69.0 h, 78.7 h and 108 h in healthy adult subjects, patients with mild hepatic function disorder and those with moderate hepatic function disorder, respectively. Geometric mean ratios (patients with hepatic function disorder/healthy adults) with 90% CIs for C
max of the main metabolite M10 were 0.947 [0.684, 1.31] and 0.766 [0.552, 1.06], respectively, and those for AUC
(0-inf) of M10 were 0.950 [0.703, 1.28] and 1.04 [0.754, 1.42], respectively. C
max was slightly lower in patients with mild and moderate hepatic function disorder than in healthy adults, but AUC
(0-inf) was similar between these patients and healthy adult subjects. The terminal elimination half-lives (mean) of M10 were 64.3 h, 66.6 h and 91.2 h in healthy adults, patients with mild hepatic function disorder and those with moderate hepatic function disorder, respectively. No study of pharmacokinetics has been conducted in patients with severe hepatic function disorder (Child-Pugh score: 10-15). (See CONTRAINDICATIONS and Careful Administration under Precautions.)
Patients with Renal Impairment: In 8 patients with severe renal impairment (estimated glomerular filtration rate [eGFR] by MDRD equation, 15-29 mL/min/1.73 m
2) who received DAYVIGO at 10 mg as a single dose, geometric mean ratios (patients with renal impairment/healthy adults) with 90% CIs for C
max and AUC
(0-inf) of lemborexant were 1.05 [0.774, 1.42] and 1.50 [1.13, 1.99], respectively. C
max and AUC
(0-inf) were 5% and 50% higher in patients with severe renal impairment than in healthy adults, respectively. The terminal elimination half-lives (mean) of lemborexant were 70.0 h and 74.8 h in health adults and patients with severe renal impairment, respectively. Geometric mean ratios (patients with renal impairment/healthy adults) with 90% CIs for C
max and AUC
(0-inf) of the main metabolite M10 were 0.725 [0.481, 1.09] and 1.36 [0.982, 1.90], respectively. C
max was 28% lower and AUC
(0-inf) was 36% higher in patients with severe renal impairment than in healthy adults, respectively. The terminal elimination half-lives (mean) of M10 were 64.0 h and 64.7 h in healthy adults and patients with severe renal impairment, respectively. (See Careful Administration under Precautions.)
Drug Interactions (Data from Non-Japanese Subjects): Itraconazole: In 15 healthy adults on itraconazole at 200 mg once daily as repeated doses who received DAYVIGO at 10 mg as a single dose, geometric mean ratios (combination therapy/monotherapy) with 90% CIs for C
max and AUC
(0-inf) of lemborexant were 1.36 [1.18, 1.57] and 3.70 [3.18, 4.31], respectively. C
max and AUC
(0-inf) of lemborexant were 36% and 270% higher with combination therapy than those with monotherapy, respectively. Terminal elimination half-lives (mean) of lemborexant with monotherapy and combination therapy were 54.4 h and 118 h, respectively. Geometric mean ratios (combination therapy/monotherapy) with 90% CIs for C
max and AUC
(0-inf) of M10 were 0.130 [0.107, 0.158] and 0.626 [0.465, 0.844], respectively. The terminal elimination half-lives (mean) of M10 with monotherapy and combination therapy were 48.1 h and 150 h, respectively. (See Precautions related to dosage and administration under Dosage & Administration and Interactions.)
Fluconazole: In 14 healthy adults on fluconazole at 200 mg once daily as repeated doses who received DAYVIGO at 10 mg as a single dose, geometric mean ratios (combination therapy/monotherapy) with 90% CIs for C
max and AUC
(0-inf) of lemborexant were 1.62 [1.34, 1.97] and 4.17 [3.83, 4.55], respectively. C
max and AUC
(0-inf) of lemborexant were 62% and 317% higher with combination therapy than those with monotherapy, respectively. The terminal elimination half-lives (mean) of lemborexant with monotherapy and combination therapy were 55.4 h and 99.5 h, respectively. Geometric mean ratios (combination therapy/monotherapy) with 90% CIs for C
max and AUC
(0-inf) of M10 were 0.580 [0.513, 0.657] and 2.33 [1.73, 3.14], respectively. Terminal elimination half-life (mean) of M10 with monotherapy and combination therapy were 45.5 h and 78.6 h, respectively. (See Precautions related to dosage and administration under Dosage & Administration and Interactions.)
Rifampin: In 15 healthy adults on rifampicin at 600 mg once daily as repeated doses who received DAYVIGO at 10 mg as a single dose, geometric mean ratios (combination therapy/monotherapy) with 90% CIs for C
max and AUC
(0-inf) of lemborexant were 0.085 [0.067, 0.107] and 0.034 [0.026, 0.045], respectively. C
max and AUC
(0-inf) of lemborexant were 92% and 97% lower with combination therapy than those with monotherapy, respectively. The terminal elimination half-lives (mean) of lemborexant with monotherapy and combination therapy were 45.6 h and 10.8 h, respectively. Geometric mean ratios (combination therapy/monotherapy) with 90% CIs for C
max and AUC
(0-inf) of M10 were 1.00 [0.884, 1.13] and 0.127 [0.112, 0.145], respectively. The terminal elimination half-lives (mean) of M10 with monotherapy and combination therapy were 39.4 h and 4.07 h, respectively. (See Interactions.)
Midazolam: In 28 healthy adults on DAYVIGO at 10 mg once daily as repeated doses who received midazolam at 2 mg as a single dose, geometric mean ratios (combination therapy/monotherapy) with 90% CIs for C
max and AUC
(0-inf) of midazolam were 1.13 [1.03, 1.24] and 1.13 [1.02, 1.25], respectively. C
max and AUC
(0-inf) of midazolam were 13% and 13% higher with combination therapy than those with monotherapy, respectively. The terminal elimination half-lives (mean) of midazolam with monotherapy and combination therapy were 4.00 h and 4.21 h, respectively.
Alcohol: In 21 healthy adults on DAYVIGO at 10 mg once daily as a single dose, concomitant intake of alcohol resulted in additive declines in cognition. Moreover, geometric mean ratios (with concomitant intake of alcohol/without concomitant intake of alcohol) with 90% CIs for C
max and AUC
(0-72h) of lemborexant were 1.35 [1.14, 1.60] and 1.70 [1.54, 1.89], respectively. C
max and AUC
(0-72h) of lemborexant were 35% and 70% higher with concomitant intake of alcohol than without concomitant intake of alcohol, respectively. The terminal elimination half-lives (mean) of lemborexant were 33.9 h and 29.9 h with and without concomitant intake of alcohol, respectively. (See Interactions.)
Note: The approved dose of DAYVIGO is 5 mg.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image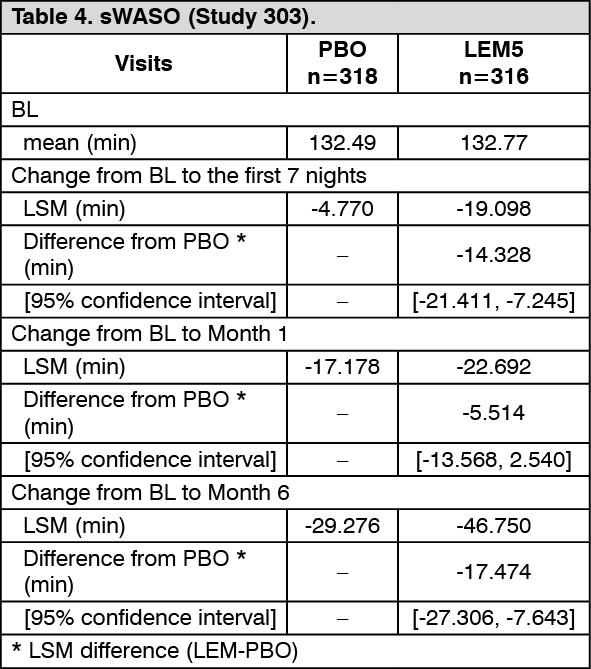 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image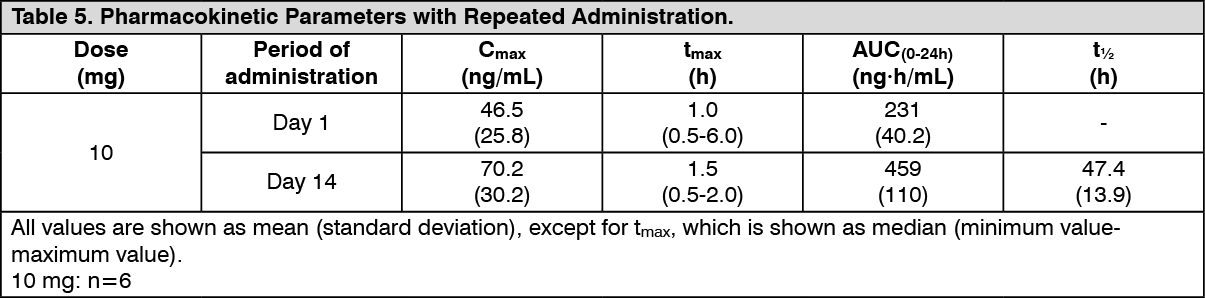 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image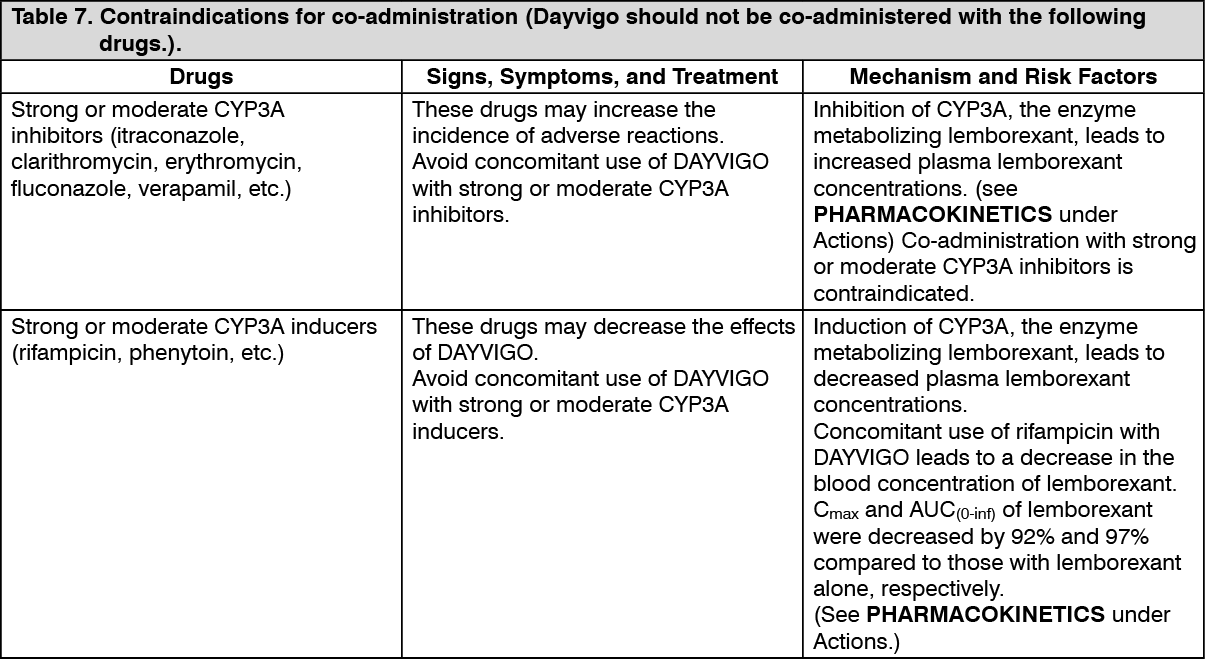 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image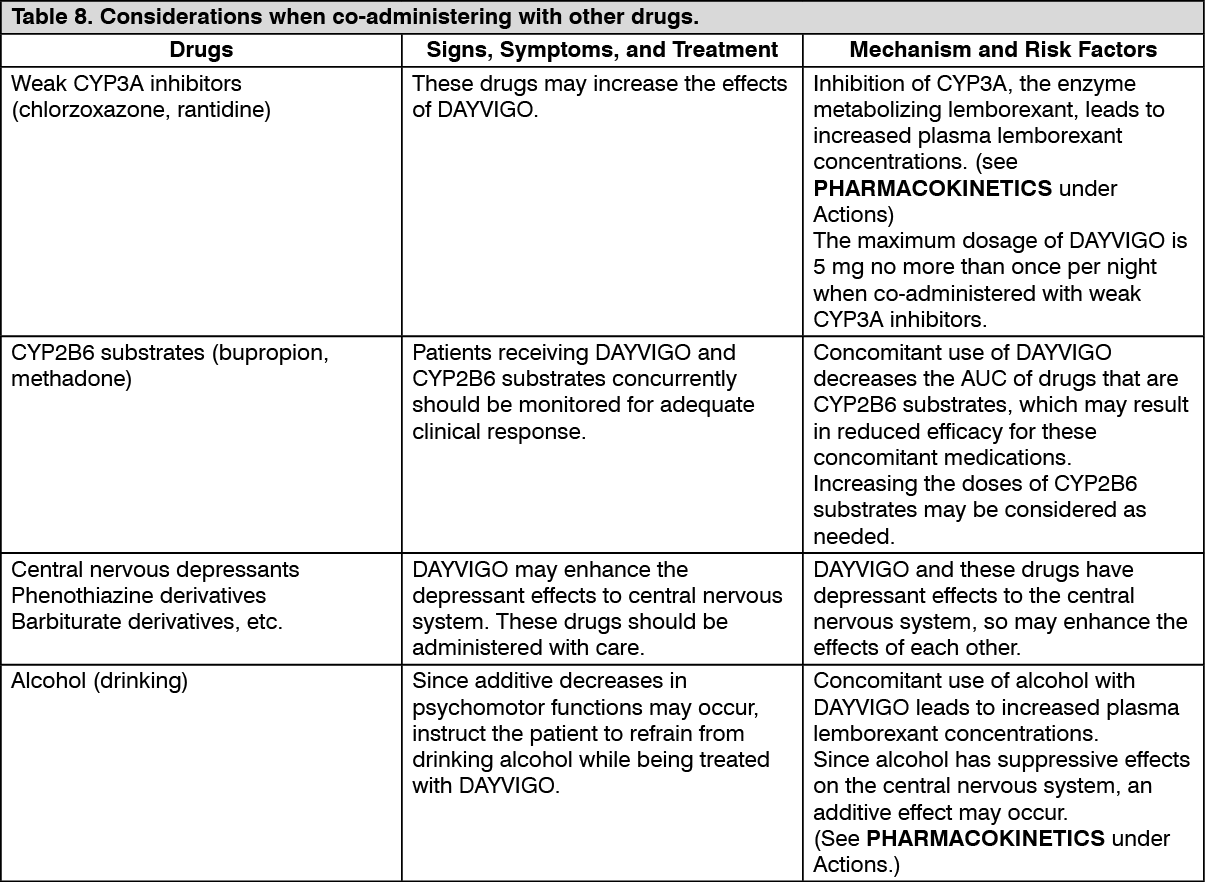 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
