Carbotrap 50 Tablet: Each tablet contains: Acarbose 50 mg.
Carbotrap 100 Tablet: Each tablet contains: Acarbose 100 mg.
Pharmacology: Pharmacodynamics: The active ingredient of Carbotrap is acarbose, a pseudotetrasaccharide of microbial origin. Acarbose exerts its activity in the intestinal tract. The action is based on the inhibition of intestinal enzymes (α-glucosidases) involved in the degradation of disaccharides, oligosaccharides and polysaccharides. This leads to a dose-dependent delay in the digestion of these carbohydrates.
Most importantly, glucose derived from carbohydrates is released and taken up into blood more slowly. In this way acarbose postpones and reduces the postprandial rise in blood glucose. As a result of the balancing effect on the uptake of glucose from the intestine, the blood glucose fluctuations over the day are reduced and the mean blood glucose values decrease.
Pharmacokinetics: Following administration, only 1-2% of the active inhibitor was absorbed.
The pharmacokinetics of Acarbose were investigated after oral administration of the 14C-labelled substance (200 mg) to healthy volunteers. On average, 35% of the total radioactivity (sum of the inhibitory substance and any degradation products) was excreted by the kidneys within 96 h. The proportion of inhibitory substance excreted in the urine was 1.7% of the administered dose. 50% of the activity was eliminated within 96 hours in the faeces. The course of the total radioactivity concentration in plasma was comprised of two peaks. The first peak, with an average acarbose equivalent concentration of 52.2±15.7 μg/l after 1.1±0.3 h, is in agreement with corresponding data for the concentration course of the inhibitor substance (49.5±26.9 µg/l after 2.1±1.6 h). The second peak is on average 586.3±282.7 µg/L and is reached after 20.7±5.2 h. The second, higher peak is due to the absorption of bacterial degradation products from distal parts of the intestine. In contrast to the total radioactivity, the maximum plasma concentration of the inhibitory substance are lower by a factor of 10-20. The plasma elimination half-lives of the inhibitory substance are 3.7±2.7 h for the distribution phase and 9.6±4.4 h for the elimination phase.
A relative volume of distribution of 0.32 l/kg body-weight has been calculated in healthy volunteers from the concentration course in the plasma.
Additional therapy in association with diet in patients with diabetes mellitus.
The dosage must be adjusted by the doctor to suit each patient, because efficacy and tolerability vary from one individual to another.
Unless otherwise prescribed, the recommended dosage is as follows: Initially: 3 x 1 tablet of 50 mg acarbose/day or 3 x ½ tablet of 100 mg acarbose/day.
Subsequently: 3 x 2 tablets of 50 mg acarbose/day or 3 x 1 tablet of 100 mg acarbose/day up to 3 x 2 tablets of 100 mg acarbose/day.
The dose may be increased after 4-8 weeks, and if patients show an inadequate clinical response in the later course of the treatment. If distressing complaints develop in spite of strict adherence to the diet the dose should not be increased further, and if necessary should be somewhat reduced. The average dose is 300 mg acarbose/day (corresponding to 3 x 2 tablets of Acarbose 50 mg/day, or 3 x 1 tablet Acarbose 100 mg/day).
Elderly (above 65 years): No alteration of dosage or dosing frequency is recommended with regard to the age of the patients.
Children: See Contraindications and Precautions.
Hepatic impairment: No dose adjustment is required in patients with pre-existing hepatic function.
Renal impairment: See Contraindications.
Nature and duration of use: Acarbose tablets are effective only if swallowed whole with a little liquid directly before the meal or be chewed with the first few mouthfuls of the meal. No limit to the length of time for which Acarbose can be used is envisaged. The limitation on dosage is due to the secondary effects of carbohydrate mal-absorption, in particular distention, flatulence and loose stools. Some adaptation to these effects occurs in the first few weeks of use. The optimal therapeutic dose is established by minimizing whilst reducing postprandial glycaemic rises. Diabetic diet should be adhered during acarbose administration.
When Acarbose tablet are taken with drinks and/or meals containing carbohydrates (disaccharides, oligosaccharides or polysaccharides), overdosage can lead to meteorism, flatulence and diarrhoea.
In the event of Acarbose tablet being taken in an overdose independently of food, excessive intestinal symptoms need not be anticipated.
In cases of overdosage the patients should not be given drinks or meals containing carbohydrates (disaccharides, oligosaccharides or polysaccharides) for the next 4 to 6 hours.
Hypersensitivity to acarbose and/or to inactive constituents.
Chronic intestinal disorders associated with distinct disturbances of digestion and absorption. States which may deteriorate as a result of increased gas formation in the intestine (e.g. Roemheld's syndrome, major hernias, intestinal obstructions, and intestinal ulcers).
Acarbose is contraindicated in-patients with severe renal impairment (creatinine clearance <25 mL/min). Inflammatory bowel disease, such as ulcerative colitis and Crohn's disease, partial intestinal obstructions or in patients predisposed to intestinal obstruction or ileus. Since the information on its effects and tolerability in children and adolescents is still insufficient, Acarbose should not be used in patients under 18 years of age.
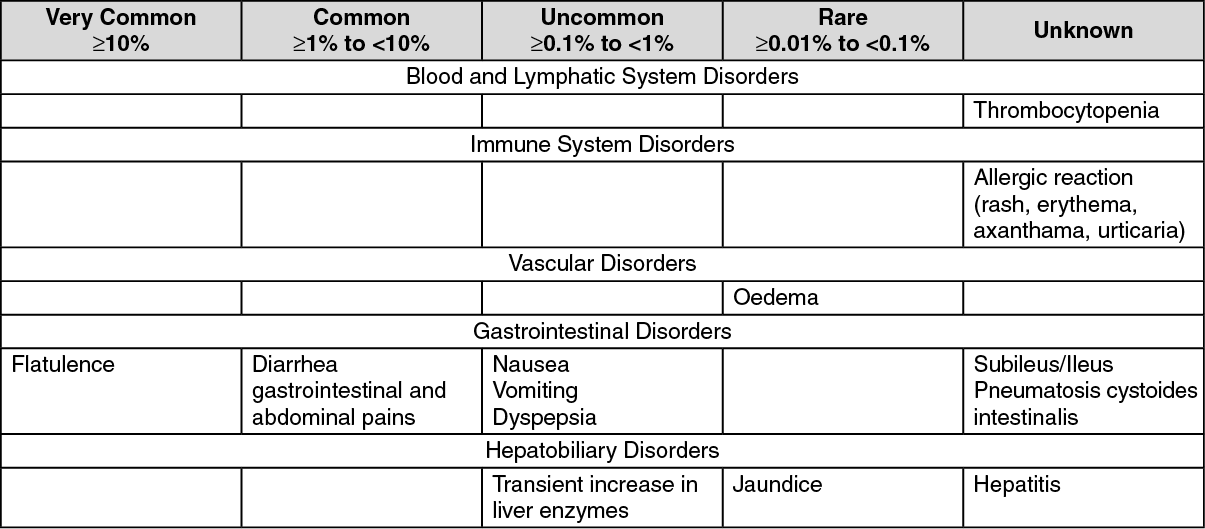
Asymptomatic liver enzyme elevations may occur in individual cases. Therefore, liver enzyme monitoring should be considered during the first 6 to 12 months of treatment. In evaluable cases these changes were reversible on discontinuation of Acarbose therapy. Safety and efficacy of Acarbose in patients under 18 years of age have not been established.
Acarbose should not be administered during pregnancy, as no information is available on its use in pregnant woman. After administration of radio labeled acarbose to lactating rats a small quantity of the radioactivity was found in the milk. There are as yet no corresponding findings in humans. However, as drug-induced effects of acarbose in milk have not been excluded in babies, in principle it is advisable not to prescribe Acarbose during the breast-feeding period.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
If the prescribed diabetic diet is not observed the intestinal side effects may be intensified. If strongly distressing symptoms develop in spite of adherence to the diabetic diet prescribed, the doctor must be consulted and the dose temporarily or permanently reduced. In patients receiving the recommended daily dose of 150 to 300 mg acarbose/day, rarely clinically relevant abnormal liver function tests (three times above upper limit of normal range) were observed. (See Precautions).
Abnormal values may be transient under ongoing acarbose therapy.
Sucrose (cane sugar) and foods containing sucrose often cause abdominal discomfort or even diarrhoea during treatment with Acarbose as a result of increased carbohydrate fermentation in the colon.
Acarbose has an antihyperglycaemic effect, but does not itself induce hypoglycaemia. If Acarbose is prescribed in addition to drugs containing sulphonylureas or metformin, or in addition to insulin, a fall of the blood glucose values into the hypoglycaemic range may necessitate a suitable decrease in the sulphonylurea, metformin or insulin dose. In individual cases hypoglycaemic shock may occur.
If acute hypoglycaemia develops it should be borne in mind that sucrose (cane sugar) is broken down into fructose and glucose more slowly during treatment with Acarbose; for this reason sucrose is unsuitable for a rapid alleviation of hypoglycaemia and glucose should be used instead.
In individual cases Acarbose may affect digoxin bioavailability, which may require dose adjustment of digoxin. Because they may possibly influence the action of Acarbose, simultaneous administration of cholestyramine, intestinal adsorbents, and digestive enzyme products should be avoided. No interaction was observed with dimeticone/simeticone. Certain drugs tend to produce hyperglycaemia and may lead to loss of blood glucose control. These drugs included diuretics (thiazides, furosemide), corticosteroids, phenothiazines, thyroid products, estrogens, oral contraceptive, phenytoin, nicotinic acid, symphatomimetics and isoniazid. When such of drugs are administered to a patient receiving acarbose, the patients should be closely monitored for loss of blood glucose control.
Due to neomycin induced ma-absorption of carbohydrate, concomitant administration of neomycin may lead to an enhanced reduction of post prandial blood glucose and to an increased in the frequently and severity of gastrointestinal adverse reactions. If the symptoms are severe, a temporary dose reduction of acarbose may warranted.
A10BF01 - acarbose ; Belongs to the class of alpha glucosidase inhibitors. Used in the treatment of diabetes.
Carbotrap tab 100 mg
3 × 10's
Carbotrap tab 50 mg
3 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
