Pharmacology: Mechanism of Action: Studies suggest that EPA reduces hepatic very low-density lipoprotein triglycerides (VLDL-TG) synthesis and/or secretion and enhances TG clearance from circulating VLDL particles. Potential mechanisms of action include increased β-oxidation; inhibition of acyl-CoA:1,2-diacylglycerol acyltransferase (DGAT); decreased lipogenesis in the liver; and increased plasma lipoprotein lipase activity.
The mechanisms of action contributing to reduction of cardiovascular events with VASCEPA (icosapent ethyl) are not completely understood but are likely multi-factorial. Increased EPA lipid composition from carotid plaque specimens and increased circulating EPA/arachidonic acid ratio have been observed following EPA treatment. EPA inhibits platelet aggregation under some ex vivo conditions. However, the direct clinical meaning of individual findings is not clear.
Pharmacodynamics: In a 12-week, dose-ranging study in patients with severe hypertriglyceridemia and in the event-driven REDUCE-IT trial, VASCEPA 4 grams per day reduced median TG from baseline relative to placebo [see Clinical Studies as follows].
Clinical Studies: Prevention of Cardiovascular Events: REDUCE-IT (NCT01492361) was a multinational, double-blind, randomized, placebo-controlled, event-driven trial in 8,179 (4,089 VASCEPA, 4,090 placebo) statin-treated adult patients enrolled with LDL-C >40 mg/dL and ≤100 mg/dL and elevated TG levels (90% of enrolled patients had TG ≥ 150 mg/dL and <500 mg/dL) and either established cardiovascular disease (71%) or diabetes and other risk factors for cardiovascular disease (29%). Patients with established cardiovascular disease were defined as being at least 45 years of age and having a documented history of coronary artery disease, cerebrovascular or carotid disease, or peripheral artery disease. Patients with other risk factors for cardiovascular disease were defined as being at least 50 years of age with diabetes and at least one additional risk factor. Patients were randomly assigned 1:1 to receive either VASCEPA (4 grams daily) or placebo. The median follow-up duration was 4.9 years. Overall, 99.8% of patients were followed for vital status until the end of the trial or death.
The median age at baseline was 64 years and 29% were women. The trial population was 90% White, 5% Asian, 2% Black; 4% identified as Hispanic ethnicity. Selected additional baseline risk factors included hypertension (87%), type 2 diabetes mellitus (58%), eGFR < 60 mL/min per 1.73 m
2 (22%), congestive heart failure (18%), and current daily cigarette smoking (15%).
Most patients were taking moderate-intensity (63%) or high-intensity (31%) statin therapy at baseline. Most patients at baseline were taking at least one other cardiovascular medication, including anti-platelet agents (79%) or anti-hypertensives (95%), including beta blockers (71%), angiotensin converting enzyme (ACE) inhibitors (52%), or angiotensin receptor blockers (ARB; 27%).
On stable background lipid-lowering therapy, the median [Q1, Q3] LDL-C at baseline was 75.0 [62.0, 89.0] mg/dL; the mean (SD) was 76.2 (20.3) mg/dL. The median [Q1, Q3] fasting TG was 216.0 [176.0, 272.5] mg/dL; the mean (SD) was 233.2 (80.1) mg/dL.
VASCEPA significantly reduced the risk for the primary composite endpoint (time to first occurrence of cardiovascular death, myocardial infarction, stroke, coronary revascularization, or hospitalization for unstable angina; p<0.0001) and the key secondary composite endpoint (time to first occurrence of cardiovascular death, myocardial infarction, or stroke; p<0.0001). The results of the primary, key secondary, and other secondary efficacy endpoints in the prespecified testing hierarchy to control for type 1 error are shown in Table 1. The Kaplan-Meier estimates of the cumulative incidence of the primary composite endpoints over time are shown in Figure 1. (See Table 1 and Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The median TG and LDL-C baseline values were similar between the VASCEPA group and placebo group. The median change in TG from baseline to Year 1 was -39 mg/dL (-18%) in the VASCEPA group and 5 mg/dL (2%) in the placebo group. The median change in LDL-C from baseline to Year 1 was 2 mg/dL (3%) in the VASCEPA group and 7 mg/dL (10%) in the placebo group.
Severe Hypertriglyceridemia: The effects of VASCEPA 4 grams per day were assessed in a randomized, placebo-controlled, double-blind, parallel-group study of adult patients (76 on VASCEPA, 75 on placebo) with severe hypertriglyceridemia. Patients whose baseline TG levels were between 500 and 2,000 mg/dL were enrolled in this study for 12 weeks. The median baseline TG and LDL-C levels in these patients were 684 mg/dL and 86 mg/dL, respectively. Median baseline HDL-C level was 27 mg/dL. The randomized population in this study was mostly Caucasian (88%) and male (76%). The mean age was 53 years and the mean body mass index was 31 kg/m
2. Twenty-five percent of patients were on concomitant statin therapy, 28% were diabetics, and 39% of the patients had TG levels >750 mg/dL.
The changes in the major lipoprotein lipid parameters for the groups receiving VASCEPA or placebo are shown in Table 2. (See Table 2.)
Click on icon to see table/diagram/image
VASCEPA 4 grams per day reduced median TG, VLDL-C, and Apo B levels from baseline relative to placebo. The reduction in TG observed with VASCEPA was not associated with elevations in LDL-C levels relative to placebo.
Pharmacokinetics: Absorption: After oral administration, VASCEPA is de-esterified during the absorption process and the active metabolite EPA is absorbed in the small intestine and enters the systemic circulation mainly via the thoracic duct lymphatic system. Peak plasma concentrations of EPA were reached approximately 5 hours following oral doses of VASCEPA.
VASCEPA was administered with or following a meal in all clinical studies; no food effect studies were performed. Take VASCEPA with or following a meal.
Distribution: The mean volume of distribution at steady state of EPA is approximately 88 liters. The majority of EPA circulating in plasma is incorporated in phospholipids, triglycerides and cholesteryl esters, and <1% is present as the unesterified fatty acid. Greater than 99% of unesterified EPA is bound to plasma proteins.
Elimination: Metabolism: EPA is mainly metabolized by the liver via beta-oxidation similar to dietary fatty acids. Beta oxidation splits the long carbon chain of EPA into acetyl Coenzyme A, which is converted into energy via the Krebs cycle. Cytochrome P450-mediated metabolism is a minor pathway of elimination of EPA.
Excretion: The total plasma clearance of EPA at steady state is 684 mL/hr. The plasma elimination half-life (t
1/2) of EPA is approximately 89 hours. VASCEPA does not undergo renal excretion.
Specific Populations: Gender: When administered VASCEPA in clinical trials, plasma total EPA concentrations did not differ significantly between men and women.
Pediatric: The pharmacokinetics of VASCEPA have not been studied in pediatric patients.
Hepatic or Renal Impairment: VASCEPA has not been studied in patients with renal or hepatic impairment.
Drug Interaction Studies: Omeprazole: In a drug-drug interaction study with 28 healthy adult subjects, VASCEPA 4 g/day at steady-state did not significantly change the steady-state AUC
τ or C
max of omeprazole when co-administered at 40 mg/day to steady-state.
Rosiglitazone: In a drug-drug interaction study with 28 healthy adult subjects, VASCEPA 4 g/day at steady-state did not significantly change the single dose AUC or C
max of rosiglitazone at 8 mg.
Warfarin: In a drug-drug interaction study with 25 healthy adult subjects, VASCEPA 4 g/day at steady-state did not significantly change the single dose AUC or C
max of
R- and
S-warfarin or the anti-coagulation pharmacodynamics of warfarin when co-administered as racemic warfarin at 25 mg.
Atorvastatin: In a drug-drug interaction study of 26 healthy adult subjects, VASCEPA 4 g/day at steady-state did not significantly change the steady-state AUC
τ or C
max of atorvastatin, 2-hydroxyatorvastatin, or 4-hydroxyatorvastatin when co-administered with atorvastatin 80 mg/day at steady-state.
Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: In a 2-year rat carcinogenicity study with oral gavage doses of 0.09, 0.27, and 0.91 g/kg/day icosapent ethyl, respectively, males did not exhibit drug-related neoplasms. Hemangiomas and hemangiosarcomas of the mesenteric lymph node, the site of drug absorption, were observed in females at clinically relevant exposures based on body surface area comparisons across species relative to the maximum clinical dose of 4 g/day. Overall incidence of hemangiomas and hemangiosarcomas in all vascular tissues did not increase with treatment.
In a 6-month carcinogenicity study in Tg.rasH2 transgenic mice with oral gavage doses of 0.5, 1, 2, and 4.6 g/kg/day icosapent ethyl, drug-related incidences of benign squamous cell papilloma in the skin and subcutis of the tail was observed in high dose male mice. The papillomas were considered to develop secondary to chronic irritation of the proximal tail associated with fecal excretion of oil and therefore not clinically relevant. Drug-related neoplasms were not observed in female mice.
Icosapent ethyl was not mutagenic with or without metabolic activation in the bacterial mutagenesis (Ames) assay or in the
in vivo mouse micronucleus assay. A chromosomal aberration assay in Chinese Hamster Ovary (CHO) cells was positive for clastogenicity with and without metabolic activation.
In an oral gavage rat fertility study, ethyl-EPA, administered at doses of 0.3, 1, and 3 g/kg/day to male rats for 9 weeks before mating and to female rats for 14 days before mating through day 7 of gestation, increased anogenital distance in female pups and increased cervical ribs were observed at 3 g/kg/day (7 times human systemic exposure with 4 g/day clinical dose based on a body surface area comparison).


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image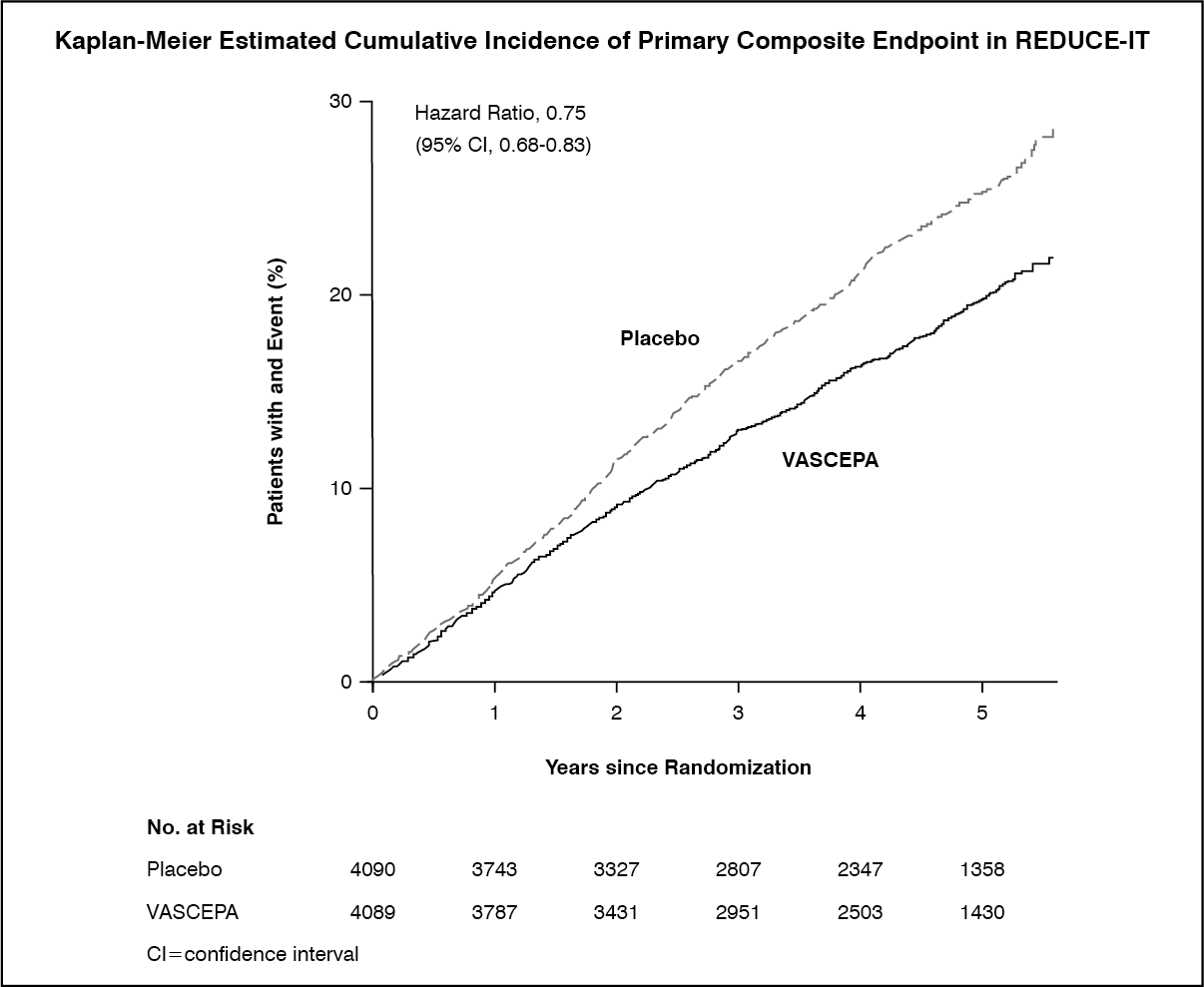 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
