


 Sign Out
Sign Out


Dexketoprofen: Administer with caution in patients with a history of allergic conditions.
The use of dexketoprofen with concomitant other NSAIDs including cyclooxygenase-2 selective inhibitors should be avoided (see Interactions).
Undesirable effects may be minimised by using the lowest effective dose for the shortest duration necessary to control symptoms (see Dosage & Administration, and Gastrointestinal safety and Cardiovascular and cerebrovascular safety as follows).
Gastrointestinal safety: Gastrointestinal bleeding, ulceration or perforation which can be fatal, have been reported with all NSAIDs at anytime during treatment, with or without warning symptoms or a previous history of serious gastrointestinal events. When gastrointestinal bleeding or ulceration occurs in patients receiving dexketoprofen, the treatment should be withdrawn.
The risk of gastrointestinal bleeding, ulceration or perforation is higher with increasing NSAID doses, in patients with a history of ulcer, particularly if complicated with haemorrhage or perforation (see Contraindications), and in older people.
As with all NSAIDs, any history of oesophagitis, gastritis and/or peptic ulcer must be identified in order to ensure their total cure before starting treatment with dexketoprofen. Patients with gastrointestinal symptoms or history of gastrointestinal disease should be monitored for digestive disturbances, especially gastrointestinal bleeding.
NSAIDs should be used with caution in patients with a history of gastrointestinal disease (ulcerative colitis, Crohn's disease) as their condition may be exacerbated (see Adverse Reactions).
Combination therapy with protective agents (e.g. misoprostol or proton pump inhibitors) should be considered for these patients, and also for patients requiring concomitant low dose acetylsalicylic acid, or other drugs likely to increase gastrointestinal risk (see as follows and Interactions).
Patients with a history of gastrointestinal toxicity, particularly when elderly, should report any unusual abdominal symptoms (especially gastrointestinal bleeding) particularly in the initial stages of treatment.
Caution should be advised in patients receiving concomitant medications which could increase the risk of ulceration or bleeding, such as oral corticosteroids, anticoagulants such as warfarin, selective serotonin reuptake inhibitors or anti-platelet agents such as acetylsalicylic acid (see Interactions).
Renal safety: Caution should be exercised in patients with impairment of renal functions. In these patients, the use of NSAIDs may result in deterioration of renal function, fluid retention and oedema. Caution is also required in patients receiving diuretic therapy or those who could develop hypovolaemia as there is an increased risk of nephrotoxicity.
Adequate fluid intake should be ensured during treatment to prevent dehydration and possibly associated increased renal toxicity.
As with all NSAIDs, it can increase plasma urea nitrogen and creatinine. As with other inhibitors of prostaglandin synthesis, it can be associated with adverse effects on the renal system which can lead to glomerular nephritis, interstitial nephritis, renal papillary necrosis, nephrotic syndrome and acute renal failure.
Long-term administration of NSAIDs has resulted in renal papillary necrosis and other renal injury. Renal toxicity has also been seen in patients in whom renal prostaglandins have a compensatory role in the maintenance of renal perfusion. In these patients, administration of a NSAID may cause a dose-dependent reduction in prostaglandin formation and, secondarily, in renal blood flow, which may precipitate overt renal decompensation. Patients at greatest risk of this reaction are those with impaired renal function, heart failure, liver dysfunction, those taking diuretics and ACE inhibitors, and the elderly. Discontinuation of NSAID therapy is usually followed by recovery to the pretreatment state.
No information is available from controlled clinical studies regarding the use of dexketoprofen in patients with advanced renal disease. Therefore, treatment with dexketoprofen is contraindicated in these patients with advanced renal disease. If therapy must be initiated, close monitoring of the patient's renal function is advisable.
Liver safety: Caution should be exercised in patients with impairment of hepatic functions. As with other NSAIDs, it can cause transient small increases in some liver parameters, and also significant increases in aspartate transaminase (AST) also known as serum glutamic oxaloacetic transaminase (SGOT) and Alanine transaminase (ALT), also known as serum glutamic pyruvic transaminase (SGPT). In case of a relevant increase in such parameters, therapy must be discontinued.
Cardiovascular and cerebrovascular safety: Appropriate monitoring and advice are required for patients with a history of hypertension and/or mild to moderate congestive heart failure as fluid retention and oedema have been reported in association with NSAIDs therapy. Special caution should be exercised in patients with a history of cardiac disease, in particular those with previous episodes of heart failure as there is an increased risk of triggering heart failure.
Clinical trial and epidemiological data suggest that use of some NSAIDs (particularly at high doses and in long-term treatment) may be associated with a small increase in the risk of arterial thrombotic events (for example myocardial infarction or stroke), which can be fatal. There are insufficient data to exclude such a risk for dexketoprofen. This risk may increase with duration of use. Patients with cardiovascular disease or risk factors for cardiovascular disease may be at greater risk.
Patients with uncontrolled hypertension, congestive heart failure, established ischaemic heart disease, peripheral arterial disease, and/or cerebrovascular disease should only be treated with dexketoprofen after careful consideration. Similar consideration should be made before initiating long-term treatment of the patients with risk factors for cardiovascular disease (e.g. hypertension, hyperlipidaemia, diabetes mellitus, smoking).
All non-selective NSAIDs can inhibit platelet aggregation and prolong bleeding time via inhibition of prostaglandin synthesis. Therefore, the use of dexketoprofen in patients who are receiving other therapy that interferes with haemostasis, such as warfarin or other coumarins or heparins is not recommended (see Interactions).
Skin reactions: Serious skin reactions, some of them fatal, including exfoliative dermatitis, Stevens-Johnson syndrome, and toxic epidermal necrolysis, have been reported very rarely in association with the use of NSAIDs (see Adverse Reactions). Patients appear to be at highest risk of these reactions early in the course of therapy, the onset of the reaction occurring in the majority of cases within the first month of treatment. Dexketoprofen should be discontinued at the first appearance of skin rash, mucosal lesions, or any other sign of hypersensitivity.
Masking of symptoms of underlying infections: Dexketoprofen can mask symptoms of infection, which may lead to delayed initiation of appropriate treatment and thereby worsening the outcome of the infection. This has been observed in bacterial community acquired pneumonia and bacterial complications to varicella. When this medicine is administered for pain relief in relation to infection, monitoring of infection is advised. In non-hospital settings, the patient should consult a doctor if symptoms persist or worsen.
Exceptionally, varicella can be at the origin of serious cutaneous and soft tissues infectious complications. To date, the contributing role of NSAIDs in the worsening of these infections cannot be ruled out. Thus, it is advisable to avoid use of dexketoprofen in case of varicella.
Other information: Particular caution is required in patients with: congenital disorder of porphyrin metabolism (e.g. acute intermittent porphyria); dehydration; directly after major surgery.
Severe acute hypersensitivity reactions (anaphylactic shock, for example) have been observed on very rare occasions. Treatment must be discontinued at the first signs of severe hypersensitivity reactions following intake of dexketoprofen. Depending on the symptoms, any medically required procedures must be initiated by specialist healthcare professionals.
Patients with asthma combined with chronic rhinitis, chronic sinusitis, and/or nasal polyposis have a higher risk of allergy to acetylsalicylic acid and/or NSAIDs than the rest of the population. Administration of this medicinal product can cause asthma attacks or bronchospasm, particularly in subjects allergic to acetylsalicylic acid or NSAIDs (see Contraindications).
Dexketoprofen should be administered with caution to patients suffering from haematopoietic disorders, systemic lupus erythematosus or mixed connective tissue disease.
Effects on ability to drive and use machines: The effects known for the single components of SKUDEXA apply to the fixed combination.
Dexketoprofen has minor or moderate influence on the ability to drive and use machines, due to possible occurrence of dizziness or somnolence.
Use in the Elderly: The elderly have an increased frequency of adverse reactions to NSAIDs especially gastrointestinal bleeding and perforation which may be fatal (see Dosage & Administration). These patients should commence treatment on the lowest dose available.
Elderly are more likely to be suffering from impaired renal cardiovascular or hepatic function (see Dosage & Administration).
Use in Children: The safety and efficacy of Skudexa in children and adolescents have not been established. Therefore Skudexa should not be used in children and adolescents.
Tramadol: Tramadol should be used with particular caution in addicted patients, patients with head injury, shock, a reduced level of consciousness of uncertain origin, disorders of the respiratory centre or function, or increased intracranial pressure.
In patients sensitive to opiates the product should be used with caution.
Care should be taken when treating patients with respiratory depression, or if concomitant CNS depressant drugs are being administered (see Interactions), or if the recommended dosage is significantly exceeded (see Overdosage) as the possibility of respiratory depression cannot be excluded in these situations.
Convulsions have been reported in patients receiving tramadol at the recommended dose levels. The risk may be increased when doses of tramadol exceed the recommended upper daily dose limit (400 mg).
In addition tramadol may increase the seizure risk in patients taking other medicinal products that lower the seizure threshold (see Interactions). Patients with epilepsy or those susceptible to seizures should only be treated with tramadol if there are compelling circumstances.
Tolerance, psychic and physical addiction may develop, especially after long-term use. In patients with a tendency to drug abuse or dependence, treatment with tramadol should only be carried out for short periods under strict medical supervision.
Avoid the use of Skudexa in adolescents 12 to 18 years of age who have other risk factors that may increase their sensitivity to the respiratory depressant effects of tramadol unless the benefits outweigh the risks. Risk factors include conditions associated with hypoventilation, such as post-operative status, obstructive sleep apnea, obesity, severe pulmonary disease, neuromuscular disease, and concomitant use of other medications that cause respiratory depression.
When a patient no longer requires therapy with tramadol, it may be advisable to taper the dose gradually to prevent symptoms of withdrawal.
Risk from concomitant use of sedative medicines such as benzodiazepines or related drugs: Concomitant use of Skudexa and sedative medicines such as benzodiazepines or related drugs may result in sedation, respiratory depression, coma and death. Because of these risks, concomitant prescribing with these sedative medicines should be reserved for patients for whom alternative treatment options are not possible. If a decision is made to prescribe Skudexa concomitantly with sedative medicines, the lowest effective dose should be used, and the duration of treatment should be as short as possible.
The patients should be followed closely for signs and symptoms of respiratory depression and sedation. In this respect, it is strongly recommended to inform patients and their caregivers to be aware of these symptoms (see Interactions).
Serotonin syndrome: Serotonin syndrome, a potentially life-threatening condition, has been reported in patients receiving tramadol in combination with other serotonergic agents or tramadol alone (see Interactions, Adverse Reactions and Overdosage).
If concomitant treatment with other serotonergic agents is clinically warranted, careful observation of the patient is advised, particularly during treatment initiation and dose escalations.
Symptoms of serotonin syndrome may include mental status changes, autonomic instability, neuromuscular abnormalities and/or gastrointestinal symptoms.
If serotonin syndrome is suspected, a dose reduction or discontinuation of therapy should be considered depending on the severity of the symptoms. Withdrawal of the serotonergic drugs usually brings about a rapid improvement.
Sleep-related breathing disorders: Opioids can cause sleep-related breathing disorders including central sleep apnoea (CSA) and sleep-related hypoxemia. Opioid use increases the risk of CSA in a dose-dependent fashion. In patients who present with CSA, consider decreasing the total opioid dosage.
Adrenal insufficiency: Opioid analgesics may occasionally cause reversible adrenal insufficiency requiring monitoring and glucocorticoid replacement therapy. Symptoms of acute or chronic adrenal insufficiency may include e.g. severe abdominal pain, nausea and vomiting, low blood pressure, extreme fatigue, decreased appetite, and weight loss.
CYP2D6 metabolism: Tramadol is metabolised by the liver enzyme CYP2D6. If a patient has a deficiency or is completely lacking this enzyme an adequate analgesic effect may not be obtained. Estimates indicate that up to 7% of the Caucasian population may have this deficiency. However, if the patient is an ultra-rapid metaboliser there is a risk of developing of opioid toxicity even at commonly prescribed doses. General symptoms of opioid toxicity include confusion, somnolence, shallow breathing, small pupils, nausea, vomiting, constipation and lack of appetite. In severe cases this may include symptoms of circulatory and respiratory depression, which may be life-threatening and very rarely fatal. Estimates of prevalence of ultra-rapid metabolisers in different populations are summarised as follows: See Table 1.
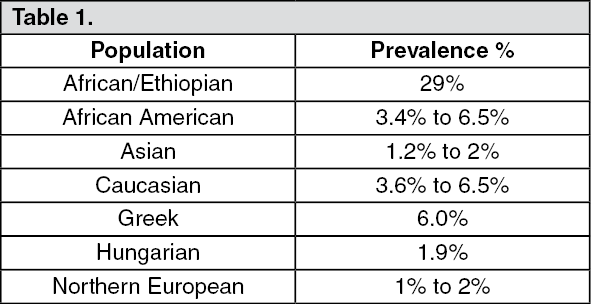 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThis medicinal product contains less than 1 mmol sodium (23mg) per dose, i.e. essentially "sodium-free".
Effects on ability to drive and use machines: The effects known for the single components of SKUDEXA apply to the fixed combination.
Even when taken according to instructions, tramadol may cause effects such as somnolence and dizziness and therefore may impair the reactions of drivers and machine operators.
This applies particularly in conjunction with other psychotropic substances and alcohol.
Use in Children: Post-operative use in children: There have been reports in the published literature that tramadol given post-operatively in children after tonsillectomy and/or adenoidectomy for obstructive sleep apnoea, led to rare, but life-threatening adverse events. Extreme caution should be exercised when tramadol is administered to children for post-operative pain relief and should be accompanied by close monitoring for symptoms of opioid toxicity including respiratory depression.
Children with compromised respiratory function: Tramadol is not recommended for use in children in whom respiratory function might be compromised including neuromuscular disorders, severe cardiac or respiratory conditions, upper respiratory or lung infections, multiple trauma or extensive surgical procedures. These factors may worsen symptoms of opioid toxicity.