


 Sign Out
Sign Out

Posology: Rheumatoid arthritis, psoriatic arthritis and axial spondyloarthritis: The recommended dose of upadacitinib is 15 mg once daily.
Consideration should be given to discontinuing treatment in patients with axial spondyloarthritis who have shown no clinical response after 16 weeks of treatment. Some patients with initial partial response may subsequently improve with continued treatment beyond 16 weeks.
Atopic dermatitis: Adults: The recommended dose of upadacitinib is 15 mg or 30 mg once daily based on individual patient presentation.
A dose of 15 mg is recommended for patients at higher risk of venous thromboembolism (VTE), major adverse cardiovascular events (MACE) and malignancy (see Precautions).
A dose of 30 mg once daily may be appropriate for patients with high disease burden who are not at higher risk of VTE, MACE and malignancy (see Precautions) or patients with an inadequate response to 15 mg once daily.
The lowest effective dose to maintain response should be used.
For patients 65 years of age and older, the recommended dose is 15 mg once daily (see Precautions).
Adolescents (from 12 to 17 years of age): The recommended dose of upadacitinib is 15 mg once daily for adolescents weighing at least 30 kg.
Concomitant topical therapies: Upadacitinib can be used with or without topical corticosteroids. Topical calcineurin inhibitors may be used for sensitive areas such as the face, neck, and intertriginous and genital areas.
Consideration should be given to discontinuing upadacitinib treatment in any patient who shows no evidence of therapeutic benefit after 12 weeks of treatment.
Ulcerative colitis: Induction: The recommended induction dose of upadacitinib is 45 mg once daily for 8 weeks. For patients who do not achieve adequate therapeutic benefit by week 8, upadacitinib 45 mg once daily may be continued for an additional 8 weeks (see Adverse Reactions and Pharmacology: Pharmacodynamics under Actions). Upadacitinib should be discontinued in any patient who shows no evidence of therapeutic benefit by week 16.
Maintenance: The recommended maintenance dose of upadacitinib is 15 mg or 30 mg once daily based on individual patient presentation: A dose of 15 mg is recommended for patients at higher risk of VTE, MACE and malignancy (see Precautions).
A dose of 30 mg once daily may be appropriate for some patients, such as those with high disease burden or requiring 16-week induction treatment who are not at higher risk of VTE, MACE and malignancy (see Precautions) or who do not show adequate therapeutic benefit to 15 mg once daily.
The lowest effective dose to maintain response should be used.
For patients 65 years of age and older, the recommended dose is 15 mg once daily (see Precautions).
In patients who have responded to treatment with upadacitinib, corticosteroids may be reduced and/or discontinued in accordance with standard of care.
Crohn's disease: Induction: The recommended induction dose of upadacitinib is 45 mg once daily for 12 weeks. For patients who have not achieved adequate therapeutic benefit after the initial 12-week induction, prolonged induction for an additional 12 weeks with a dose of 30 mg once daily may be considered. For these patients, upadacitinib should be discontinued if there is no evidence of therapeutic benefit after 24 weeks of treatment.
Maintenance: The recommended maintenance dose of upadacitinib is 15 mg or 30 mg once daily based on individual patient presentation: A dose of 15 mg is recommended for patients at higher risk of VTE, MACE and malignancy (see Precautions).
A dose of 30 mg once daily may be appropriate for patients with high disease burden who are not at higher risk of VTE, MACE and malignancy (see Precautions) or who do not show adequate therapeutic benefit to 15 mg once daily.
The lowest effective dose to maintain response should be used.
For patients 65 years of age and older, the recommended maintenance dose is 15 mg once daily (see Precautions).
In patients who have responded to treatment with upadacitinib, corticosteroids may be reduced and/or discontinued in accordance with standard of care.
Interactions: For patients with ulcerative colitis and Crohn's disease receiving strong inhibitors of cytochrome P450 (CYP) 3A4 (e.g., ketoconazole, clarithromycin), the recommended induction dose is 30 mg once daily and the recommended maintenance dose is 15 mg once daily (see Interactions).
Dose initiation: Treatment should not be initiated in patients with an absolute lymphocyte count (ALC) that is <0.5 x 109 cells/L, an absolute neutrophil count (ANC) that is <1 x 109 cells/L or who have haemoglobin (Hb) levels that are <8 g/dL (see Precautions and Adverse Reactions).
Dose interruption: Treatment should be interrupted if a patient develops a serious infection until the infection is controlled.
Interruption of dosing may be needed for management of laboratory abnormalities as described in Table 16. (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSpecial populations: Elderly: Rheumatoid arthritis, psoriatic arthritis, and axial spondyloarthritis: There are limited data in patients 75 years of age and older.
Atopic dermatitis: For atopic dermatitis, doses higher than 15 mg once daily are not recommended in patients 65 years of age and older (see Adverse Reactions).
Ulcerative colitis and Crohn's disease: For ulcerative colitis and Crohn's disease, doses higher than 15 mg once daily for maintenance therapy are not recommended in patients 65 years of age and older (see Adverse Reactions). The safety and efficacy of upadacitinib in patients 75 years of age and older have not yet been established.
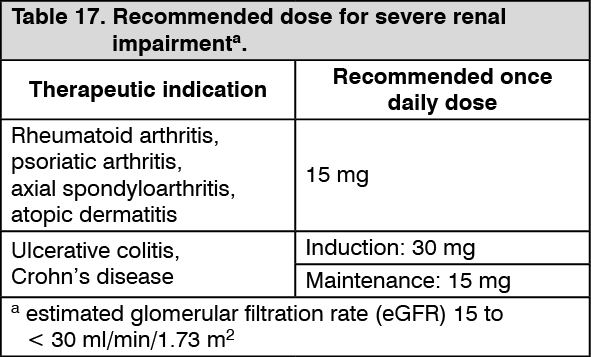
Renal impairment: No dose adjustment is required in patients with mild or moderate renal impairment. There are limited data on the use of upadacitinib in subjects with severe renal impairment (see Pharmacology: Pharmacokinetics under Actions). Upadacitinib should be used with caution in patients with severe renal impairment as described in Table 17 as follows. The use of upadacitinib has not been studied in subjects with end stage renal disease and is therefore not recommended for use in these patients. (See Table 17.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageHepatic impairment: No dose adjustment is required in patients with mild (Child-Pugh A) or moderate (Child-Pugh B) hepatic impairment (see Pharmacology: Pharmacokinetics under Actions). Upadacitinib should not be used in patients with severe (Child-Pugh C) hepatic impairment (see Contraindications).
Paediatric population: The safety and efficacy of RINVOQ in children with atopic dermatitis below the age of 12 years have not been established. No data are available. No clinical exposure data are available in adolescents <40 kg (see Pharmacology: Pharmacokinetics under Actions).
The safety and efficacy of RINVOQ in children and adolescents with rheumatoid arthritis, psoriatic arthritis, axial spondyloarthritis, ulcerative colitis, and Crohn's disease, aged 0 to less than 18 years have not yet been established. No data are available.
Method of administration: RINVOQ is to be taken orally once daily with or without food and may be taken at any time of the day. Tablets should be swallowed whole and should not be split, crushed, or chewed in order to ensure the entire dose is delivered correctly.