


 Sign Out
Sign Out

Permanent discontinuation of Retsevmo for treatment emergent adverse events, regardless of attribution occurred in 8.0% of patients. ADRs resulting in permanent discontinuation (2 or more patients) included increased ALT (0.6%), fatigue (0.6%), increased AST (0.5%), hypersensitivity (0.3%), and thrombocytopenia (0.3%).
Tabulated list of adverse drug reactions: The ADRs reported in patients treated with selpercatinib are shown in Table 8.
The ADRs are classified according to the MedDRA system organ class.
Frequency groups are defined by the following convention: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1000 to <1/100); rare (≥1/10000 to <1/1000); very rare (<1/10000), and not known (cannot be estimated from available data).
Within each frequency group, undesirable effects are presented in order of decreasing seriousness. Median time on treatment with selpercatinib was 21.3 months. (See Table 8.)
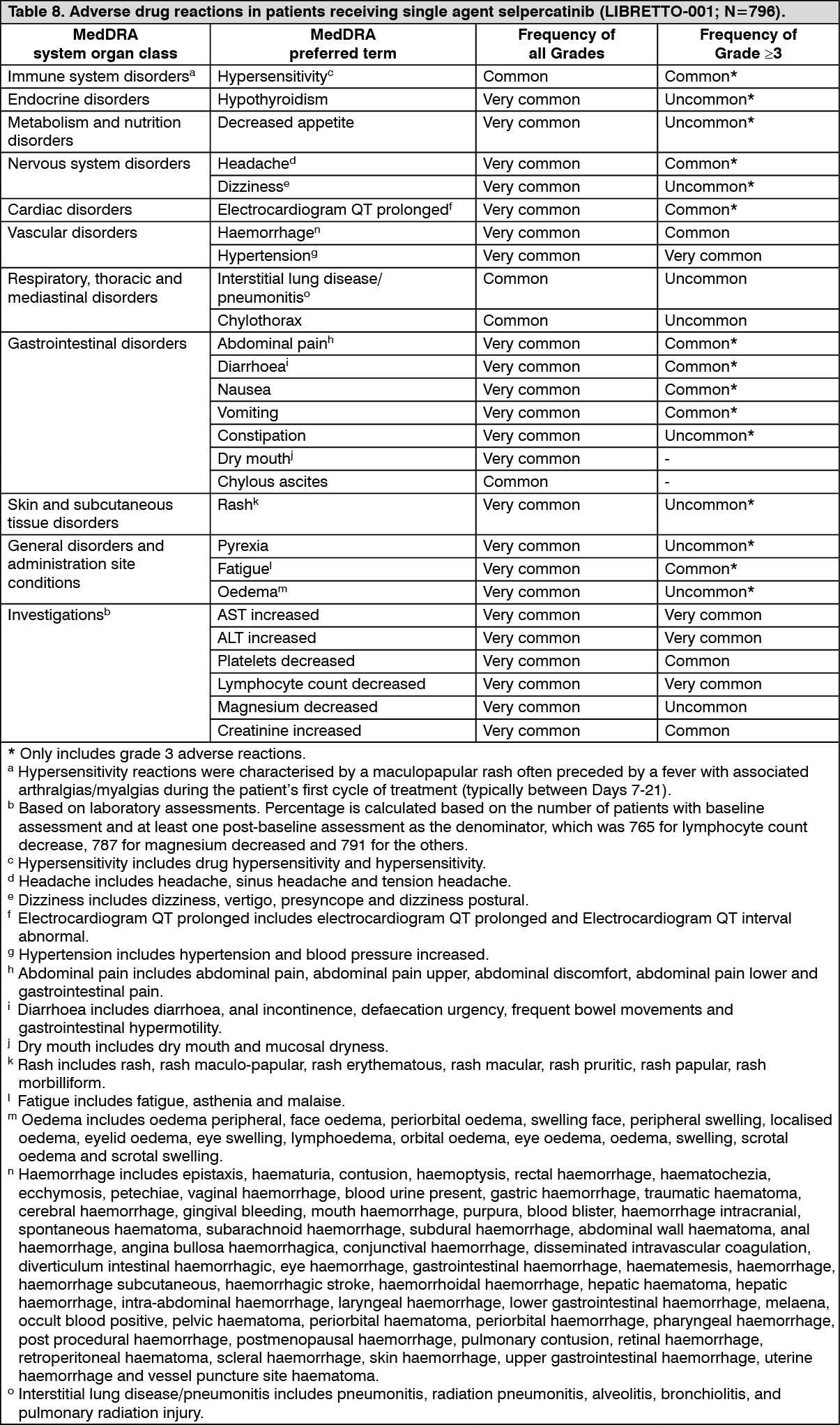 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Aminotransferase elevations (AST/ALT increased): Based on laboratory assessment, ALT and AST elevations were reported in 55.5% and 58.9% patients, respectively. Grade 3 or 4 ALT or AST elevations were reported in 11.8% and 10.6% patients respectively.
The median time to first onset was: AST increase 4.3 weeks (range: 0.7, 151.7), ALT increase 4.3 weeks (range: 0.9, 144.0).
Dose modification is recommended for patients who develop Grade 3 or 4 ALT or AST increase (see Dosage & Administration).
QT interval prolongation: In the 792 patients who had ECGs, review of data showed 7.3% of patients had >500 msec maximum post-baseline QTcF value, and 19.8% of patients had a >60 msec maximum increase from baseline in QTcF intervals. At the time of the last post-baseline measurement, increase in QTc value >60 msec was reported in 2.1% of patients.
There were no reports of Torsade de pointes, sudden death, ventricular tachycardia, ventricular fibrillation, or ventricular flutter related to selpercatinib. No patient discontinued treatment due to QT prolongation.
Retsevmo may require dose interruption or modification (see Dosage & Administration and Precautions).
Hypertension: In the 793 patients who had blood pressure measurements, the median maximum increase from baseline systolic pressure was 31 mm Hg (range: -12, +96). Only 10.8% of patients retained their baseline grade during treatment, 42.2% had an increasing shift of 1 grade, 37.1% of 2 grades, and 9.3% of 3 grades. A treatment emergent adverse event of hypertension was reported in 43.9% patients with history of hypertension (28.2% with grade 3, 4) and 38.8% of patients without history of hypertension (13.7% with grade 3, 4).
Overall, a total of 19.6% displayed treatment-emergent Grade 3 hypertension (defined as maximum systolic blood pressure greater than 160 mm Hg). Grade 4 treatment emergent hypertension was reported in 0.1% of patients. Diastolic blood pressure results were similar, but the increases were of lesser magnitude.
One patient was permanently discontinued due to hypertension. Dose modification is recommended in patients who develop hypertension (see Dosage & Administration). Selpercatinib should be discontinued permanently if medically significant hypertension cannot be controlled with antihypertensive therapy (see Precautions).
Hypersensitivity: Signs and symptoms of hypersensitivity included fever, rash and arthralgias or myalgias with concurrent decreased platelets or increased aminotransferase.
In study LIBRETTO-001, 24.7% (197/796) of patients treated with selpercatinib had previously received anti-PD-1/PD-L1 immunotherapy. Hypersensitivity occurred in a total of 5.9% (47/796) of patients receiving selpercatinib, including Grade 3 hypersensitivity in 1.9% (15/796) of patients.
Of the 47 patients with hypersensitivity, 55.3% (26/47) had NSCLC and had received prior anti-PD-1/PD-L1 immunotherapy.
Grade 3 hypersensitivity occurred in 3.6% (7/197) of the patients previously treated with anti-PD-1/PD-L1 immunotherapy.
The median time to onset was 1.9 weeks (range: 0.7 to 112.1 weeks): 1.7 weeks in patients with previous anti-PD-1/PD-L1 immunotherapy and 4.4 weeks in patients who were anti-PD-1/PD-L1 immunotherapy naïve.
Retsevmo may require dose interruption or modification (see Dosage & Administration).
Haemorrhages: Grade ≥3 haemorrhagic events occurred in 3.1% of patients treated with selpercatinib, including 4 (0.5%) patients with fatal haemorrhagic events, two cases of cerebral haemorrhage, and one case each of tracheostomy site haemorrhage, and haemoptysis. The median time to onset was 24.3 weeks (range: 0.1 week to 147.6 weeks).
Selpercatinib should be discontinued permanently in patients with life-threatening or recurrent severe haemorrhage (see Dosage & Administration).
Additional information on special populations: Paediatric patients: There were 3 patients <18 years (range: 15-17) of age in LIBRETTO-001. The safety of selpercatinib in children aged less than 18 years has not been established.
Elderly: In patients receiving selpercatinib, 24.4% were ≥65-74 years of age, 8.3% were 75-84 years of age, and 1.0% ≥85 years of age. The frequency of serious adverse events reported was higher in patients ≥65-74 years (51.5%), 75-84 years (56.1%), and ≥85 years (100.0%), than in patients <65 years (39.4%) of age.
The frequency of AE leading to discontinuation of selpercatinib was higher in patients ≥65-74 years (7.2%), 75-84 years (18.2%), and ≥85 years (25.0%), than in patients <65 years of age (6.8%).
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions to the Drug Office, Department of Health.
View ADR Monitoring Form