


 Sign Out
Sign Out

Up to approximately one third of the patients treated with Femara in the metastatic setting and approximately 80% of the patients in the adjuvant setting as well as in the extended adjuvant setting experienced adverse reactions. The majority of the adverse reactions occurred during the first few weeks of treatment.
The most frequently reported adverse reactions in clinical studies were hot flushes, hypercholesterolaemia, arthralgia, fatigue, increased sweating and nausea.
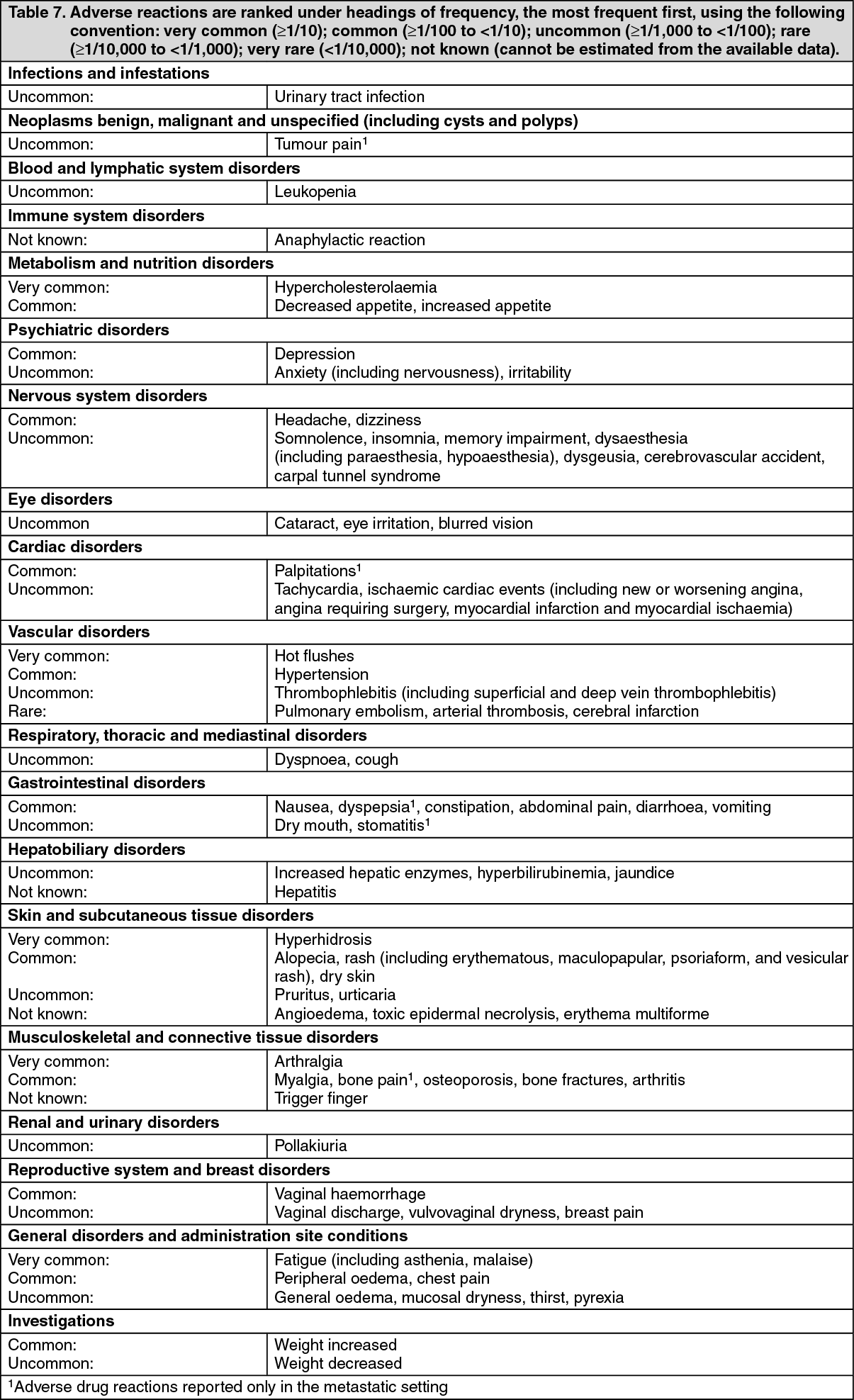
Important additional adverse reactions that may occur with Femara are: skeletal events such as osteoporosis and/or bone fractures and cardiovascular events (including cerebrovascular and thromboembolic events). The frequency category for these adverse reactions is described in Table 7.
Tabulated list of adverse reactions: The frequencies of adverse reactions for Femara are mainly based on data collected from clinical trials.
The following adverse drug reactions, listed in Table 7, were reported from clinical studies and from post-marketing experience with Femara: See Table 7.
 Click on icon to see table/diagram/image
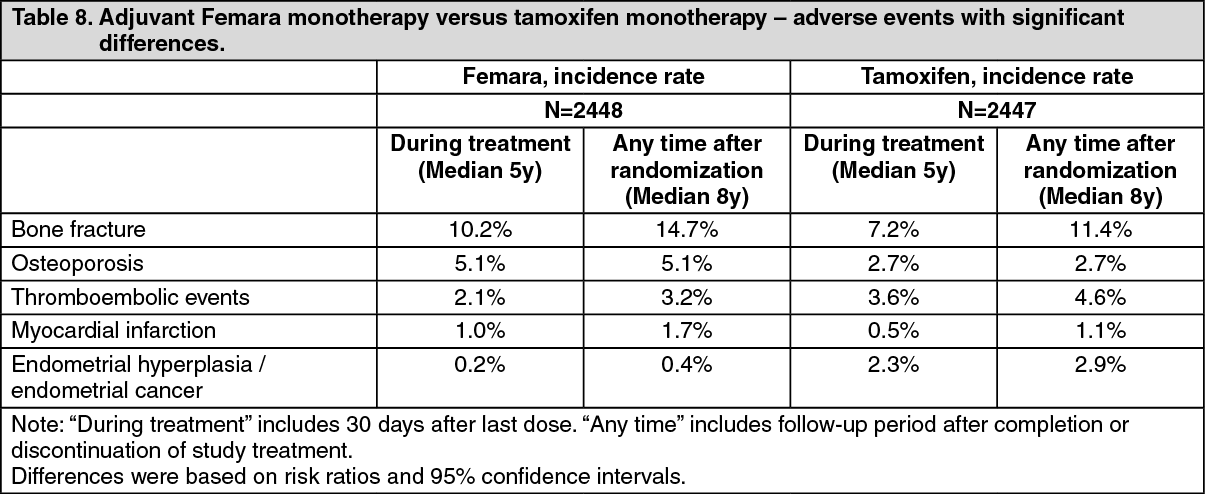
Click on icon to see table/diagram/imageSome adverse reactions have been reported with notably different frequencies in the adjuvant treatment setting. The following tables provide information on significant differences in Femara versus tamoxifen monotherapy and in the Femara-tamoxifen sequential treatment therapy: See Tables 8 and 9.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image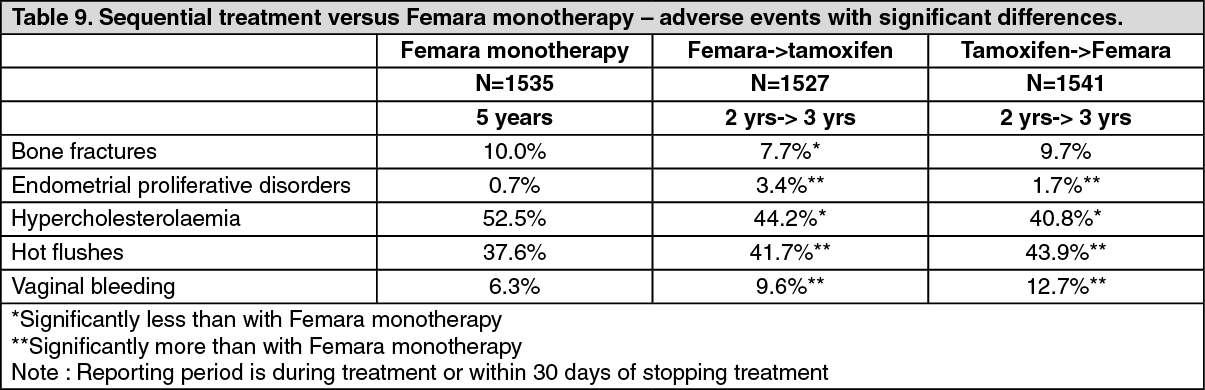 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Cardiac adverse reactions: In the adjuvant setting, in addition to the data presented in Table 8, the following adverse events were reported for Femara and tamoxifen, respectively (at median treatment duration of 60 months plus 30 days): angina requiring surgery (1.0% vs. 1.0%); cardiac failure (1.1% vs. 0.6%); hypertension (5.6% vs. 5.7%); cerebrovascular accident/transient ischaemic attack (2.1% vs. 1.9%).
In the extended adjuvant setting for Femara (median duration of treatment 5 years) and placebo (median duration of treatment 3 years), respectively: angina requiring surgery (0.8% vs. 0.6%); new or worsening angina (1.4% vs. 1.0%); myocardial infarction (1.0% vs. 0.7%); thromboembolic event* (0.9% vs. 0.3%); stroke/transient ischaemic attack* (1.5% vs. 0.8%) were reported.
Events marked * were statistically significantly different in the two treatment arms.
Skeletal adverse reactions: For skeletal safety data from the adjuvant setting, please refer to Table 8.
In the extended adjuvant setting, significantly more patients treated with Femara experienced bone fractures or osteoporosis (bone fractures, 10.4% and osteoporosis, 12.2%) than patients in the placebo arm (5.8% and 6.4%, respectively). Median duration of treatment was 5 years for Femara, compared with 3 years for placebo.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
View ADR Monitoring Form